1) 名古屋大学大学院医学系研究科腫瘍外科学
今日,進行再発大腸癌治療において遺伝子検査は必要不可欠なものとなっている.中でもBRAF V600E 変異症例の予後は極めて不良と報告され,その治療選択に悩むことは少なくない.今回,オキサリプラチ ンベースの術後補助化学療法が終了した直後の術後9か月の早期に,頸部リンパ節再発を来し,BRAF
V600E変異型で予後不良が予測された症例に対し,二次治療としてのFOLFIRI+aflibercept療法が著効し,
切除により病理学的完全奏効を確認した1例を経験した.術後経過観察期間は9か月とまだ短いが,外来 で無再発,無治療で経過観察中である.予後不良とされるBRAF V600E変異型であっても野生型と同様に 一定の全身コントロールが可能であれば,転移巣切除を考慮する意義はあると考えられた.
キーワード:RAS変異型大腸癌,BRAF V600E,MSI-high
はじめに
現在,進行再発大腸癌に対する治療戦略を考えるうえで,RAS/BRAF遺伝子検査は必要不可欠である1).
BRAF V600E変異はBRAF変異のうち,95%を占め2),その予後は極めて不良と報告されており,積極的外
科治療の適応は慎重に考慮すべきとの報告もある3).一方で,BRAF変異例において,マイクロサテライト 不安定性(microsatellite instability;以下,MSIと略記)high症例はmicrosatellite stable症例と比較して予後 が良い可能性が示唆されている4)5).今回,BRAF V600E変異に加え,RAS変異型かつMSI-highであった,
極めてまれなサブタイプである右側横行結腸癌の頸部リンパ節再発に対し,FOLFIRI+aflibercept(以下,
Afliと略記)療法が著効したため,1年後に外科的切除を行い,病理学的完全奏効(pathological complete
response;以下,pCRと略記)を確認した1例を経験したので報告する.
症 例
患者:68歳,女性
主訴:左頸部の腫脹と疼痛 既往歴:特記すべきことなし.
家族歴:特記すべきことなし.
現病歴:便潜血陽性の精査で進行右側横行結腸癌と診断され(Fig. 1),結腸拡大右半切除術を施行され た.術後経過は良好で術後14日目に退院した.病理結果は粘液癌,pT4aN1aM0,pStage IIIBであった
〈2020年9月28日受理〉別刷請求先:村田 悠記 〒466-8550 名古屋市昭和区鶴舞町65 名古屋大学大学院医学系研究科腫瘍外科学
(Fig. 2).術後28日目に補助化学療法としてCAPOX(capecitabine+oxaliplatin)療法を開始した.3コース 施行後にGrade 3の末梢神経障害を来したためoxaliplatinは中止し,その後capecitabine単剤を5コース施 行した.外来経過観察中の術後9か月,術後補助化学療法終了後3か月時に,左頸部の腫脹と疼痛を自覚 し,外来受診した.
来院時現症:左頸部から鎖骨上に可動性が乏しく,硬い3 cm大の腫瘤を触知した.
来院時血液検査所見:軽度腎機能障害を認める以外,目立った異常所見は認めなかった.腫瘍マーカー
ではCEAは3.5 ng/ml(正常値5未満)と正常範囲内,CA19-9は49 U/ml(正常値37以下)と軽度上昇を
認めた.
頸部造影CT所見:左頸部に37×28 mm大の不均一な造影効果を伴う腫瘤を認めた(Fig. 3a).
Fig. 1 Contrast-enhanced CT showed wall thickness of the transverse colon and some enlarged lymph nodes along the right branch of the middle colic artery.
Fig. 2 A fixed specimen was cut as shown. The tumor was diagnosed as mucinous adenocarcinoma with regional lymph node metastasis (pStage III: pT4aN1aM0).
PET-CT所見:左頸部の腫瘤はSUVmax 18.71とFDPの高い集積を認めた(Fig. 3b).他部位に明らかな 集積を認めなかった.
以上の所見より,組織学的診断は得られていないが臨床的に,術後補助化学療法終了後早期の頸部リン パ節再発と診断した.初回手術検体を用いた遺伝子検査結果は,RAS変異型(KRAS G12V),BRAF V600E 変異型であり,CAPOXに続く二次治療としてFOLFIRI+Afli療法を導入した.なお,本症例はマルチプ
レックスPCR-フラグメント解析法によるMSI検査でMSI-highであると後に判明したが,導入時には未
測定であった.
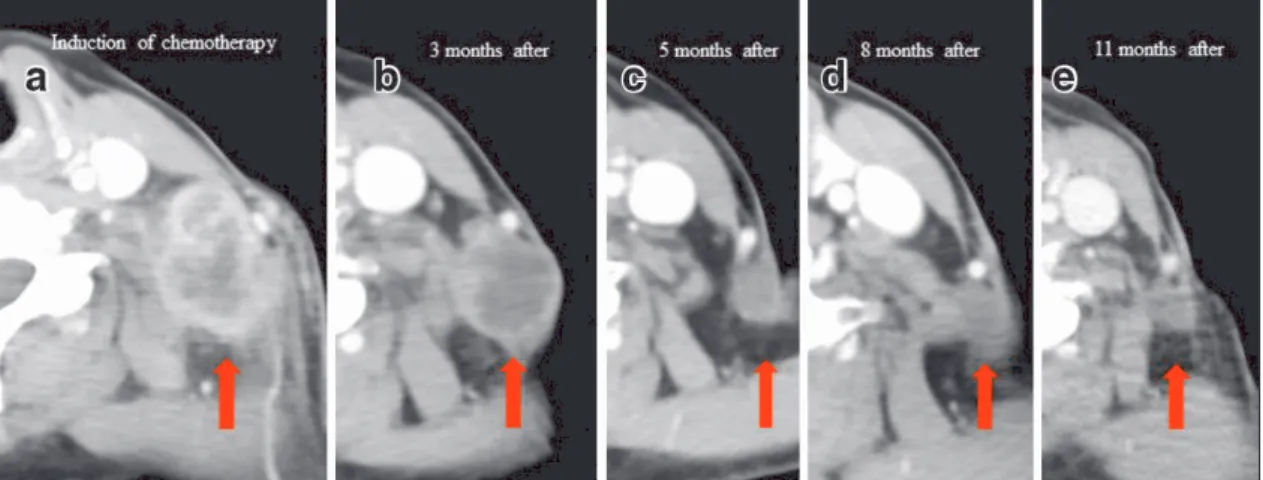
治療経過:5か月後のCTで腫瘤は16×10 mmと著明に縮小を認めた(Fig. 4).11か月後のCTでは12×
9 mmとさらに縮小を認め,PET-CTでのFDG集積も消失した.一方,腫瘍マーカーではCEAは徐々に上 昇し,10か月後の10.0 ng/mlをピークにその後5.8 ng/mlまで低下,CA19-9は治療期間中ほぼ不変であっ た.画像上,ほかに明らかな新規病変を認めず,頸部リンパ節転移巣を切除する方針とした.
手術所見:再発確認後12か月,全身麻酔下に,副神経の損傷を来さないよう細心の注意を払い,左頸部 リンパ節切除を行った.手術時間は20 分,出血量は少量であった.
Fig. 3 a: Contrast-enhanced CT showed a heterogeneous enhanced mass of 37×28 mm in the left neck. b: FDG uptake was observed on PET-CT (SUVmax: 18.71).
Fig. 4 Tumor shrinkage over time (in order from a to e). The tumor shrank rapidly and eventually touched only the scar (e).
病理組織標本所見:壊死組織を認めるのみで,腫瘍細胞の残存は認めず,pCRと診断した(Fig. 5).
術後経過:術後補助化学療法は施行せず,術後9か月が経過した現在,無再発生存中である.
考 察
全身化学療法が発達した現在,進行再発大腸癌の全生存期間の中央値は30か月を越えている6)7).BRAF 遺伝子変異は転移性大腸癌患者の5~12%に認め,その95%がBRAF V600E変異であるとされている2).一 般的に,BRAF V600E変異大腸癌は右側大腸癌や高齢女性に多いとされており,切除不能進行再発症例の みならず,術後補助化学療法後のステージII/III大腸癌においても予後不良因子と報告されている8)9).RAS/
BRAF野生型と異なり,抗EGFR抗体が使用できない変異型においては,CAPOXを用いた術後補助化学 療法後早期再発に対する二次治療は,一般的にイリノテカンベースに血管新生阻害剤を加えたものになる.
現在,本邦ではbevacizumab(以下,Bmabと略記)に加え,2016年にramucirumab(以下,Rmabと略記),
2017年にAfliが保険承認されているが10)~12),3剤の至適な使い分けは確立していない.本症例において もAfliではなくBmabまたはRmabを使用する選択肢はあった.しかし,Bmabはトリフルリジン・チピ ラシル塩酸塩配合錠(FDT/TPI)と併用することで,後の三次治療において良好な無増悪生存期間が得ら れている13).また,一次治療で70%がBmab未使用の症例群でのFOLFIRIに対する上乗せ効果を示してい るAfliに対し,FOLFIRIに対するRmabの上乗せ効果を示したRAISE試験では,一次治療で全例Bmabが 投与されており,Bmab未使用例でのRmab上乗せ効果を示すデータはない11)12),ため本症例へのAfliの導 入を決めた.
本症例では組織学的診断は得られていないものの,臨床的に明らかな頸部リンパ節転移に対する著明な 縮小が得られたため,一般的には手術適応とならない遠隔転移巣に対し,約1年間の化学療法後に切除へ 踏み切った.積極的な切除が予後を改善することが受け入れられている大腸癌肝転移ですら,BRAF V600E 変異例に対しての手術適応には議論の余地を残す3)14)15).しかし,本症例では,他部位に新たな転移を認め ないが,局所も縮小を保つが消失はしないため,化学療法を継続することは患者のPSを落すのみで有意 義ではない点,外科的切除により癌細胞遺残の有無が病理学的にも証明できる点,切除の難易度がそれほ ど高くない点を考慮し,切除に踏み切った.結果はpCRと診断され,まだ9か月と短期間ではあるもの の,現在は化学療法なしで非常に高いQOLが保たれている.たとえBRAF V600E変異型であっても,一 定の全身コントロールが可能であれば,BRAF V600E野生型と同様に,転移巣の切除を考慮する意義はあ ると考えられた.
BRAF V600E変異型大腸癌で,かつ補助化学療法終了後早期再発例であり,予後不良と考えられた本症
Fig. 5 A resected specimen of the left cervical lymph node showed only necrotic tissue without cancer cells (a), indicating a pathological complete response (b).
MSI statusも含めた治療方針決定が重要となる可能性があると思われた.
利益相反:上原 圭 講演料など:日本イーライリリー株式会社,中外製薬株式会社,サノフィ株式会 社,メルクバイオファーマ株式会社,武田薬品工業株式会社,大鵬薬品工業株式会社,第一三共株式会社,
科研製薬株式会社
文献
1) Hashiguchi Y, Muro K, Saito Y, Ito Y, Ajioka Y, Hamaguchi T, et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int J Clin Oncol. 2020 Jan;25(1):1–42.
2) Sorbye H, Dragomir A, Sundström M, Preiffer P, Thunberg U, Bergfors M, et al. High BRAF mutation frequency and marked survival differences in subgroups according to KRAS/BRAF mutation status and tumor tissue availability in a prospective population-based metastatic colorectal cancer cohort. PLoS One. 2015 Jun;10(6):e0131046.
3) Schirripa M, Bergamo F, Cremolini C, Casagrande M, Lonardi S, Aprile G, et al. BRAF and RAS mutations as prognostic factors in metastatic colorectal cancer patients undergoing liver resection. Br J Cancer. 2015 Jun;112(12):1921–8.
4) Hamilton SR. BRAF mutation and microsatellite instability status in colonic and rectal carcinoma: context really does matter. J Natl Cancer Inst. 2013 Aug;105(15):1075–7.
5) Seppälä TT, Böhm JP, Friman M, Lahtinen L, Väyrynen VM, Liipo TK, et al. Combination of microsatellite instability and BRAF mutation status for subtyping colorectal cancer. Br J Cancer. 2015 Jun;112(12):1966–75.
6) Loupakis F, Cremolini C, Masi G, Lonardi S, Zagonel V, Salvatore L, et al. Initial therapy with FOLFOXIRI and bevacizumab for metastatic colorectal cancer. N Engl J Med. 2014 Oct;371(17):1609–18.
7) Yamada Y, Denda T, Gamoh M, Iwanaga I, Yuki S, Shimodaira H, et al. S-1 and irinotecan plus bevacizumab versus mFOLFOX6 or CapeOX plus bevacizumab as first-line treatment in patients with metastatic colorectal cancer (TRICOLORE):
a randomized, open-label, phase III, noninferiority trial. Ann Oncol. 2018 Mar;29(3):624–31.
8) Richman SD, Seymour MT, Chambers P, Elliott F, Daly CL, Meade AM, et al. KRAS and BRAF mutations in advanced colorectal cancer are associated with poor prognosis but do not preclude benefit from oxaliplatin or irinotecan: results from the MRC FOCUS trial. J Clin Oncol. 2009 Dec;27(35):5931–7.
9) Zhu L, Dong C, Cao Y, Fang X, Zhong C, Li D, et al. Prognostic role of BRAF mutation in Stage II/III colorectal cancer receiving curative resection and adjuvant chemotherapy: a meta-analysis based on randomized clinical trials. PLoS One. 2016 May;11(5):e0154795.
10) Bennouna J, Sastre J, Arnold D, Österlund P, Greil R, Van Cutsem E, et al. Continuation of bevacizumab after first progression in metastatic colorectal cancer (ML18147): a randomised phase 3 trial. Lancet Oncol. 2013 Jan;14(1):29–37.
11) Tabernero J, Yoshino T, Cohn AL, Obermannova R, Bodoky G, Garcia-Carbonero R, et al. Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with metastatic colorectal carcinoma that progressed during or after first- line therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine (RAISE): a randomised, double-blind, multicentre, phase 3 study. Lancet Oncol. 2015 May;16(5):499–508.
12) Van Cutsem E, Tabernero J, Lakomy R, Prenen H, Prausová J, Macarulla T, et al. Addition of aflibercept to fluorouracil, leucovorin, and irinotecan improves survival in a phase III randomized trial in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimen. J Clin Oncol. 2012 Oct;30(28):3499–506.
13) Pfeiffer P, Yilmaz M, Möller S, Zitnjak D, Krogh M, Petersen LN, et al. TAS-102 with or without bevacizumab in patients with chemorefractory metastatic colorectal cancer: an investigator-initiated, open-label, randomised, phase 2 trial. Lancet Oncol. 2020 Mar;21(3):412–20.
14) Bachet JB, Moreno-Lopez N, Vigano L, Marchese U, Gelli M, Raoux L, et al. BRAF mutation is not associated with an increased risk of recurrence in patients undergoing resection of colorectal liver metastases. Br J Surg. 2019 Aug;106(9):1237–
47.
15) Gagnière J, Dupré A, Gholami SS, Pezet D, Boerner T, Gönen M, et al. Is hepatectomy justified for BRAF mutant colorectal liver metastases?: a multi-institutional analysis of 1497 Patients. Ann Surg. 2020 Jan;271(1):147–54.
16) Sahin IH, Kazmi SM, Yorio JT, Bhadkamkar NA, Kee BK, Garrett CR, et al. Rare though not mutually exclusive: a report of three cases of concomitant KRAS and BRAF mutation and a review of the literature. J Cancer. 2013;4(4):320–2.
17) Midthun L, Shaheen S, Deisch J, Senthil M, Tsai J, Hsueh CT, et al. Concomitant KRAS and BRAF mutations in colorectal cancer. J Gastrointest Oncol. 2019 Jun;10(3):577–81.
18) Ates O, Yalcin S. Concomitant RAS and BRAF mutation in colorectal cancer—a report of 7 cases. Indian J Cancer. 2019 Apr–
Jun;56(2):176–9.
19) Deshwar A, Margonis GA, Andreatos N, Barbon C, Wang J, Buettner S, et al. Double KRAS and BRAF mutations in surgically treated colorectal cancer liver metastases: an international, multi-institutional case series. Anticancer Res. 2018 May;38(5):2891–5.
Patients with colorectal cancer with the BRAF V600E mutation, which rarely coexists with a RAS mutation, have an extremely poor prognosis. In contrast, the outcomes of patients with a BRAF mutation and high microsatellite instability (MSI-high) have been found to be favorable. Thus, the significance of having multiple mutations remains unclear. We experienced a rare case with cervical lymph node metastasis from right-sided transverse colon cancer with RAS mutation, BRAF mutation and MSI-high, which developed 9 months after primary resection, just after completion of oxaliplatin-based 6-month adjuvant chemotherapy. As second-line chemotherapy, the patient received FOLFIRI plus aflibercept for 12 months. The tumor shrank markedly from 37 mm to 12 mm in maximum diameter and no new lesion was found; therefore, she underwent conversion surgery. Pathological findings confirmed no residual cancer cells (pathological complete response). Although the postoperative follow-up period is still <9 months, the patient has had no additional treatment after conversion surgery and is alive without recurrence. This case suggests that even in patients with metastatic colorectal cancer with the BRAF V600E mutation, aggressive surgical treatment might be an option in a situation of well-controlled systemic disease similar to that without a BRAF mutation. Further investigation of the significance of coexisting MSI-high with a BRAF mutation is required.
Key Words: colorectal cancer with BRAF mutation, BRAF V600E, MSI-high
[Jpn J Gastroenterol Surg. 2021;54(4):278-284]
Reprint requests: Yuki Murata Division of Surgical Oncology, Department of Surgery, Nagoya University Graduate School of Medicine
65 Tsurumai-cho, Showa-ku, Nagoya, 466-8550 JAPAN Accepted: September 28, 2020
© 2021 The Japanese Society of Gastroenterological Surgery