Dorsal sector
における門脈胆管枝の走行形態をもとにした尾状葉右側境界の検討
青木 修一
1)水間 正道
1)坂田 直昭
1)大塚 英郎
1)林 洋毅
1)中川 圭
1)森川 孝則
1)元井 冬彦
1)内藤 剛
1)海野 倫明
1)1) 東北大学消化器外科学
目的:肝門部領域胆管癌の術前 multi-detector row CT(以下,MDCT と略記)をもとに dorsal sector の門 脈胆管枝の走行形態を検討し,左側肝切除で切除すべき尾状葉の右側境界を明らかにする.方法:2008 年 から 2012 年まで,肝門部領域胆管癌 110 例の術前 MDCT において,dorsal sector を走行する門脈胆管枝を 同定し,Couinaud の定義をもとに dorsal sector の b,c,d,cp,l 領域を走行する門脈枝(P-b,P-c,P-d, P-cp,P-l)および胆管枝(B-b,B-c,B-d,B-cp,B-l)の分岐合流部位を検討した.結果:P-d の 85%,B-dの 91%は前/後区域枝などの二次分枝に,P-c の 91%,B-c の 96%は一次分枝に分岐合流した.P-b の 98%,P-cp と P-l は全例が一次分枝から分岐し,B-b と B-l は全例,B-cp の 92%が一次分枝に合流した.B-cの 61%および B-cp の 35%が前後区域分岐部周辺に合流し,尾状葉胆管枝の合流部位は,前後区域分岐部 周辺の頻度が最も高かった.結語:尾状葉の右側境界は c 領域と d 領域の境界にほぼ一致するが,5~10% において,c もしくは d 領域側に偏移する.左側肝切除に伴う尾状葉切除の際には,c 領域の肝実質切除と ともに,前後分岐部の胆管を完全に切除することが必須であり,右側境界が d 領域側へ偏移する症例は, d領域までの切除を考慮する必要がある. キーワード:尾状葉,computed tomography,肝門部領域胆管癌
はじめに
肝門部領域胆管癌において外科的切除は予後を期待できる唯一の方法であり,近年の R0 切除率は 66~ 95%と報告され,R0 切除は最も重要な予後因子である1)~3).肝門部領域胆管癌は,胆管に沿って水平方向 へ進展すると同時に,隣接する血管や肝実質へ垂直方向に浸潤し,この特有な腫瘍学的性質が,R0 切除を 困難にしている要因である.そのため,R0 切除には,肝門部胆管を周囲の肝実質とともに一括して切除 し,surgical margin の陰性を達成することが必須である.尾状葉は肝門部胆管に隣接する肝葉であるため, 片側の肝葉に尾状葉を合併切除することが,R0 切除率の向上および予後の延長をもたらし,現在,肝門部 領域胆管癌に対する標準術式となっている4)~6). 尾状葉は肝両葉の背側で下大静脈を取り囲むように位置している.Healey7)8)や公文9)は,尾状葉を門脈 segmentationの立場から「門脈本管もしくは一次分枝で支配される領域」と定義し,尾状葉を spiegel 葉, paracaval portion,caudate process の三つに分類し,現在ではこの定義が一般的となっている.一方, Couinaud10)11)は,形態学的に,「肝門から主要肝静脈の背側にかけて下大静脈を取り囲む領域」を dorsalsectorと捉え,さらに dorsal sector を left dorsal sector,right dorsal sector,caudate process に分類し,後に left および right dorsal sector をそれぞれ segment I および IX と分類した.このように,「尾状葉」と「dorsal
sector」の概念は異なっており,両者の領域は完全には一致しない. 肝門部領域胆管癌に対する左側肝切除では,dorsal sector のどの範囲までを尾状葉として扱い切除するべ きか,つまり尾状葉の右側境界について,いまだ一致した見解は得られていない.尾状葉もしくは dorsal sectorの門脈胆管枝の走行形態は,今まで,鋳型切除標本や CT angiography(CTA)などにより報告されて いるが12)~15),multi-detector row CT(以下,MDCT と略記)での検討は報告されていない.近年,画像技 術の進歩により,MDCT による肝門部周辺の詳細な血管や胆管の立体解剖が明らかとなり,術前に dorsal sectorにおける門脈胆管枝の走行形態を把握することが可能となった.
目
的
肝門部領域胆管癌切除症例の術前に撮像した MDCT を用いて,dorsal sector の門脈および胆管枝の走行 形態を検討し,門脈本幹もしくは一次分枝で支配される領域を尾状葉として捉え,肝門部領域胆管癌に対 する外科的切除の際に切除すべき尾状葉の右側境界を明らかにする.方
法
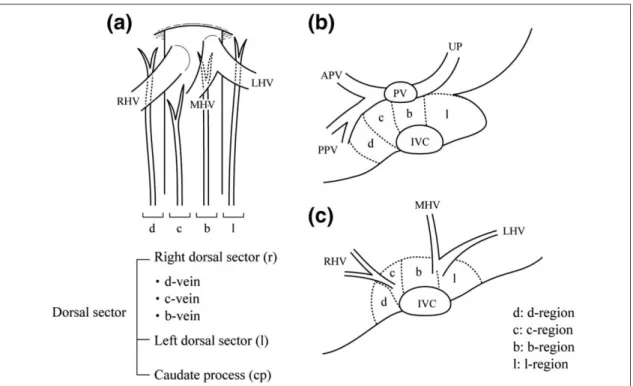
1. 対象 2008年 1 月から 2012 年 5 月まで当院で肝門部領域胆管癌の診断で術前に MDCT を撮像し,その後手術 を行った 110 名を対象とした.男性が 42 名,女性が 68 名であり,年齢中央値は 68 歳であった.手術術式 は右側肝切除が 58 例(52.7%)で,右肝切除が 54 例,右三区域切除術が 4 例であった.左側肝切除は 50 例(45.4%)で,左肝切除が 42 例,左三区域切除が 8 例であった.胆管切除は 2 例であった.東北大学大 学院医学系研究科倫理委員会は,本研究が通常の臨床で収集されたカルテ情報を基に行われた後方視的研 究であることから,被験者の同意は必要としないが,東北大学大学院医学系研究科のホームページに本研 究内容を公開し被験者のオプトアウトの権利を明示することで,本研究を承認した. 2. MDCT撮像プロトコル 64列 MDCT を用いて撮像した.非イオン性造影剤(300 mg/dl)を 5 ml/sec で 30 秒間注入し,早期動脈 相,後期動脈相,門脈相および平衡相を bolus-tracking method を用いて撮像した.2 mm スライスでの MDCT 画像を作製した. 3. Dorsal sectorの領域分類 Couinaudの分類に従い,肝門から主要肝静脈根部にかけて,門脈一次分岐部から中肝静脈根部を結び下 大静脈と平行な断面で左右二分した領域を,right および left dorsal sector(r-region,l-region)とし,肝門よ り尾側の下大静脈を取り囲む領域を caudate process(cp-region)と分類した.さらに,Couinaud の分類に ならい,right dorsal sector は,下大静脈前面の領域で b-vein(P-b)から供血される b-region,下大静脈の右 側から右肝静脈根部前面の領域で c-vein(P-c)から供血される c-region,下大静脈の右背側から右肝静脈 根部背側の領域で d-vein(P-d)から供血される d-region に分類した(Fig. 1).各領域を供血する門脈枝を P-b,P-c,P-d,P-l,P-cp とし,胆管枝も同様に B-b,B-c,B-d,B-l,B-cp とした. 4. Dorsal sectorの門脈胆管枝の走行形態 はじめに,dorsal sector の門脈枝(P-b,P-c,P-d,P-l,P-cp)の分岐部位を MDCT をもとに検討した. 分岐部位は I)門脈前後区域枝(二次分枝),II)門脈前後区分岐部周辺,III)門脈右枝(右一次分枝), IV)門脈本幹,V)門脈左枝(左一次分枝),VI)門脈臍部移行部の 6 分類とし(Fig. 2),腫瘍浸潤により 分岐部位が判別できない場合は評価不能とした.門脈 segmentation の立場では,上記分類での II)から VI)の部位で分岐する門脈枝が尾状葉枝であり,それらが供血する領域が尾状葉である. 次に,dorsal sector の胆管枝(B-b,B-c,B-d,B-l,B-cp)の肝門での合流部位を MDCT をもとに門脈枝 と同様に検討した.合流場所は I)後区域胆管枝(二次分枝),II)前後区域胆管枝の合流部周辺,III)右Fig. 1 Schema of the areas of the dorsal sector according to Couinaud’s report. (a) The dorsal sector consists of three parts: the right (r), left dorsal sector (l), and the caudate process (cp). The portal branches of the right dorsal sector are classified into three categories: b-veins located in front of the IVC, c-veins located along the right side of the IVC with the anterior of the root of the RHV, and d-veins located at the dorsolateral side of the IVC with dorsal to the root of the RHV. (b, c) Schema of the dorsal liver in axial view, showing d-, c-, b-, and l-region. RHV, right hepatic vein; LHV, left hepatic vein; APV, anterior portal vein; PPV, posterior portal vein; UP, umbilical portion; PV, portal vein; IVC, inferior vena cava; MHV, middle hepatic vein.
Fig. 2 Classification of the ramification/confluence portions of the portal/biliary branches. PV, portal vein; CHD, common hepatic duct; Pant, anterior portal vein; Bant, anterior biliary duct; Ppost, posterior portal vein; Bpost, posterior biliary duct.
肝管(右一次分枝),IV)左右肝管合流部,V)左肝管(左一次分枝),VI)門脈臍部移行部周辺の 6 分類 とした.腫瘍が左右肝管のどちらか片側に優位に存在し,腫瘍側の dorsal sector 胆管枝のみの拡張を認め る場合は,拡張し同定できる胆管枝のみを対象とした.腫瘍浸潤により合流形態が判別できない場合や, ドレナージチューブによる画質の乱れで合流形態が判別できない場合は,評価不能とした.
結
果
対象症例 110 例の術前 MDCT において,dorsal sector の門脈枝を計 360 本認め,P-d,P-c,P-b,P-cp, P-lをそれぞれ,60 本,34 本,42 本,61 本,163 本同定した(Table 1).P-d の 60 本のうち,51 本(85%) は前区域もしくは後区域門脈枝の二次分枝から分岐し,残りの 9 本(15%)は,一次分岐から分岐してい た(Fig. 3a).一方で,P-c の 9%が,前区域門脈枝から分岐し,P-c の 91%が門脈一次分岐から分岐してい た(Fig. 3b).P-b においては,前区域枝もしくは後区域枝の二次分枝から分岐する門脈枝は 2%のみで, 98%が門脈一次分枝由来であった.P-cp と P-l においては,全て一次分枝から分岐していた.門脈 segmentation の立場から「門脈本幹および一次分枝から分岐する枝」を尾状葉枝と定義すると,P-l,P-cp,P-b,P-c の それぞれ,100%,100%,98%,91%は尾状葉門脈枝であった.一方で,P-d の 15%は尾状葉門脈枝である が,85%は尾状葉門脈枝ではなく前後区域枝由来であった. Dorsal sectorの胆管枝は計 410 本認められ,B-d,B-c,B-b,B-cp,B-l をそれぞれ,56 本,51 本,79 本,46 本,178 本同定した(Table 2).B-d の 56 本のうち 51 本(91%)が,後区域胆管枝(二次分枝)にTable 1 The number of portal branches in the dorsal liver according to branch site
P-d P-c P-b P-cp P-l
Anterior/Posterior trunk 51 (85%) 3 (9%) 1 (2%) 0 (0%) 0 (0%) Bifurcation of anterior/Posterior trunk 3 (5%) 11 (32%) 1 (2%) 1 (2%) 3 (2%) Right portal vein 6 (10%) 15 (44%) 16 (39%) 38 (62%) 23 (14%) Main portal vein 0 (0%) 3 (9%) 1 (2%) 17 (27%) 15 (9%) Left portal vein 0 (0%) 1 (3%) 14 (34%) 1 (2%) 34 (21%) The transition to umbilical portion 0 (0%) 1 (3%) 9 (21%) 4 (7%) 88 (54%) Total 60 (100%) 34 (100%) 42 (100%) 61 (100%) 163 (100%)
Fig. 3 In the conventional configuration of the portal branches in the dorsal sector, 85% of P-d diverged from the anterior/posterior veins (a: white dotted arrow), which were not considered caudate branches, while over 90% of P-c (b: black dotted arrow) diverged from the first bifurcated portal branches. The boundary between the c- and d-regions closely corresponded to the right margin of the caudate lobe. On the other hand, 15% of P-d, instead of branching off the posterior portal veins, consisted of the alternately well-developed portal branches from the right portal vein, which ran dorsocranically under the inflow portion of the right hepatic vein; these were indicated to be caudate branches (a: black dotted arrow). The caudate lobe was likely to develop a dorsolateral shift toward to the d-region. On the other hand, 9% of P-c diverged from the anterior portal vein (b: white dotted arrow), which region was considered as a part of anterior segment. In these cases, the area of the anterior segment alternately developed and expanded to the central side towards the b-region.
合流し,5 本(9%)が前後区域枝合流部周辺の胆管一次分枝に合流していた.B-c の 4%が胆管二次分枝に 合流し,96%が胆管一次分枝に合流していた.B-b と B-l においては胆管二次分枝に合流したものは認めら れず,全て一次分枝に合流していた.B-cp の 8%は胆管二次分枝に合流し,残りの,92%は胆管一次分枝 に合流していた.Dorsal sector の胆管枝の合流形態は,門脈枝の分岐形態と類似していた. 前後区域分岐部周辺から分岐する門脈枝は,P-d,P-c,P-b,P-cp,P-l の 5%,32%,2%,2%,2%であ るが(Table 1),前後区域分岐部周辺に合流する胆管枝は,B-d,B-c,B-b,B-cp,B-l の 9%,61%,11%, 35%,11%であった(Table 2).前後区域分岐部周辺に分岐合流する頻度は,胆管枝の方が門脈枝より高 かった.B-c および B-cp において,前後区域分岐部周辺に合流する胆管枝の頻度は,他部位に合流する胆 管枝の頻度と比べ最も高かった.
考
察
尾状葉は,門脈 segmentation の立場から門脈本幹または一次分岐により還流される領域として定義さ れ7)~9),広く受け入れられているが,尾状葉の脈管走行を含めた解剖学的詳細はいまだ不明確な点も多く, 特に尾状葉と肝右葉の境界については一定の見解が得られていない.本検討では,P-d および B-d の約 90% が後区域枝の支配を示し,P-c,b,cp,l および B-c,b,cp,l の約 95%以上が一次分枝の支配を受けるこ とから,一般的には d 領域は尾状葉ではなく後区域の一部と考えるのが妥当であり,尾状葉の右側境界は, d領域と c 領域の境界にほぼ一致すると考えられた.この結果は,d-vein を後区域門脈枝と捉え,d-vein で 還流される領域を segment VII の一部と考える過去の報告と類似している16).石山17)は,尾状葉と肝右葉の 境界付近に,後区域門脈枝から分岐し,下大静脈の右側を平行に頭背側に向かって走行する門脈枝が存在 することを指摘しており,我々の検討における P-d の多くがこの門脈枝に一致すると考えられた.また, 谷崎ら16)は,d 領域の門脈枝は全て後区域枝から分岐し,一次分枝から分岐する d 領域の門脈枝は存在し ないと報告しているが,本検討では,10%程度の P-d は,門脈一次分枝から分岐し(Fig. 4),これら症例 の P-d は,門脈 segmentation の立場からは後区域門脈枝ではなく尾状葉門脈枝と捉えるべきである.つま り,この場合の d 領域は尾状葉の一部であり,通常よりも尾状葉の右側境界が d 領域側に偏移する. 尾状葉は,後区域と境界を接しているのと同様に,前区域(S8 と S5)とも隣接している.特に前区域 門脈枝の中枢側から分岐し右肝静脈前面に向けて頭側に走行する門脈枝(しばしば“P-8d”と呼ばれる門 脈枝)が還流する領域は,dorsal sector の c 領域と隣接する.本検討では,P-c の 91%が門脈一次分枝から 分岐しており,paracaval 門脈枝と考えられるが,残り 9%の P-c は前区域門脈枝から分岐しており,これら 門脈枝の多くは P-8d と考えられる.この場合における c 領域は S8 の一部と捉えることができ,前区域が 下大静脈側に張り出し,尾状葉右側境界は b 領域側へ偏移する.Cho ら14)は,P-8d がより中枢側から分岐 する症例では,太く発達した paracaval 門脈枝を認めないと報告しているが,本検討においても,c 領域を P-8dが還流し前区域が下大静脈側に張り出している 9%の症例では,c 領域に門脈一次分枝から分岐する paracaval門脈枝を認めることはなく,Cho らの報告を支持するものであった.Table 2 The number of biliary ducts in the dorsal liver according to confluence portions
B-d B-c B-b B-cp B-l
Posterior biliary ducts 51 (91%) 2 (4%) 0 (0%) 4 (8%) 0 (0%) Bifurcation of anterior/Posterior ducts 5 (9%) 31 (61%) 9 (11%) 16 (35%) 20 (11%) Right hepatic ducts 0 (0%) 10 (20%) 10 (13%) 12 (26%) 22 (12%) Main hepatic ducts 0 (0%) 2 (4%) 14 (18%) 3 (7%) 24 (13%) Left hepatic ducts 0 (0%) 6 (11%) 45 (57%) 9 (20%) 106 (59%) Ducts around transition of umbilical portion 0 (0%) 0 (0%) 1 (1%) 2 (4%) 6 (3%) Total 56 (100%) 51 (100%) 79 (100%) 46 (100%) 178 (100%)
Nimuraら4)は,尾状葉切除を伴う肝門部領域胆管癌切除 45 例のうち,44 例において尾状葉胆管への癌 浸潤を認め,尾状葉合併切除の必要性を提唱している.尾状葉の切除範囲については,肝門部領域胆管癌 では尾状葉胆管枝の合流部位と浸潤範囲を個々の症例で尾状葉胆管枝全枝について的確に術前把握するこ とは癌浸潤などで困難であることから,肝門部領域胆管癌の根治術では原則全尾状葉切除とすべきと考え られる.本検討から,肝門部領域胆管癌に対する左側肝切除において切除すべき尾状葉の右側範囲は,c 領域までの肝実質を十分に切除することが少なくとも必須であるが,術前の MDCT で尾状葉の右側境界が d領域に偏位している症例で,特に右側優位な肝門部胆管症例においては,d 領域胆管枝への癌進展を疑 い,d 領域までの切除を考慮する必要があると考えられる.さらに,本検討では,尾状葉胆管枝が前後区 域分岐部に合流する頻度が比較的高く,特に c 領域の胆管枝の約 60%が前後区域分岐部周辺に合流するこ とが明らかにされたことから,左側肝切除を伴う尾状葉切除の際には,前後区域分岐部の胆管を含めて尾 状葉を en block に切除することが,断端陰性の確保に重要と考えられる. MDCTは,肝門部領域胆管癌の術前診断において,癌の進展や隣接する臓器への浸潤を評価するうえで
必須の検査である.近年,multi planar reconstruction(MPR)技術の進歩により,肝門の脈管解剖を 3D イ メージとして詳細に把握することが可能となった.さらに,SYNAPSE Vincent ®(Fujifilm)などの画像解 析ソフトの登場により,脈管構造の三次元可視化や,還流領域の把握が可能となった18)19).しかし,これ らのソフトによる血管の自動解析能力には限界があり,特に尾状葉門脈枝のような,細くて複雑な走行形 態を示す脈管を正確に描出できるとは限らない.尾状葉右側境界の把握には,従来通り MDCT を詳細に検 討し,尾状葉門脈枝の立体解剖を細かく構築することが必要と思われる. 本検討では,癌の浸潤により dorsal sector の門脈胆管枝の分岐合流形態が詳細に把握できなかった症例 を 9 例認めた.腫瘍の直接浸潤やドレナージチューブによる画質の低下で正確な門脈胆管枝の走行形態の 把握が困難になる点が,本検討の限界であった.また,癌が片側に局在していたために,対側の非拡張の 尾状葉胆管枝の評価が行えなかった症例が 10 例あり,本検討が尾状葉胆管枝全てを検討したとはいえな い.Thin slice MDCT の画質の向上は,より細い門脈胆管枝の分岐部位や走行形態の術前評価を可能にした
Fig. 4 MDCT images of the axial view in late arterial phase in a 57-year-old woman with perihilar cholangio-carcinoma. P-d (arrows) diverged from the right portal vein and ran towards the dorsolateral side of the IVC. B-d (arrowheads) converged around the bifurcation of the posterior duct. In this case, the d-region was considered a part of the caudate lobe. The right margin of the caudate lobe was shifted to the d-region.
が,全ての尾状葉門脈胆管枝を把握することはいまだできず,MDCT や他の画像検査法のさらなる改良が 望まれる.本検討では,d 領域胆管枝への病理組織学的癌浸潤を評価していないため,d 領域側に尾状葉右 側境界が偏移する症例に対する d 領域切除の必要性を病理組織学的見地から評価することが今後の課題と 思われる. 尾状葉の右側境界は dorsal sector の c 領域と d 領域の境界とほぼ一致するが,5~10%の症例において, 右側境界が d 領域側にもしくは c 領域側に偏移していた.左側肝切除に伴う尾状葉切除の際には,c 領域 の肝実質切除とともに,前後分岐部の胆管を完全に切除することが断端陰性のためには必須であるが,右 側境界が d 領域側へ偏移する症例の場合は,d 領域までの切除を考慮する必要がある. 利益相反:なし
文献
1) Hemming AW, Mekeel K, Khanna A, Baquerizo A, Kim RD. Portal vein resection in management of hilar cholangiocarcinoma. J Am Coll Surg. 2011;212(4):604–13; discussion 13–6.
2) Nagino M, Nimura Y, Nishio H, Ebata T, Igami T, Matsushita M, et al. Hepatectomy with simultaneous resection of the portal vein and hepatic artery for advanced perihilar cholangiocarcinoma: an audit of 50 consecutive cases. Ann Surg. 2010;252(1): 115–23.
3) Kondo S, Hirano S, Ambo Y, Tanaka E, Okushiba S, Morikawa T, et al. Forty consecutive resections of hilar cholangiocarcinoma with no postoperative mortality and no positive ductal margins: results of a prospective study. Ann Surg. 2004;240(1):95–101.
4) Nimura Y, Hayakawa N, Kamiya J, Kondo S, Shionoya S. Hepatic segmentectomy with caudate lobe resection for bile duct carcinoma of the hepatic hilus. World J Surg. 1990;14(4):535–43; discussion 44.
5) Mizumoto R, Suzuki H. Surgical anatomy of the hepatic hilum with special reference to the caudate lobe. World J Surg. 1988;12(1):2–10.
6) Bismuth H, Nakache R, Diamond T. Management strategies in resection for hilar cholangiocarcinoma. Ann Surg. 1992;215(1): 31–8.
7) Healey JE Jr, Schroy PC. Anatomy of the biliary ducts within the human liver; analysis of the prevailing pattern of branchings and the major variations of the biliary ducts. AMA Arch Surg. 1953;66(5):599–616.
8) Healey JE Jr. Clinical anatomic aspects of radical hepatic surgery. J Int Coll Surg. 1954;22(5 Sect. 1):542–50. 9) 公文 正光.肝鋳型標本とその臨床応用 尾状葉の門脈枝と胆道枝.肝臓.1985;26(9):1193–9. 10) Couinaud C. Surgical anatomy of the liver revisited. Paris: Acheve Dimprimer Sur Les Presses; 1989. 11) Couinaud C. The paracavalsegments of the liver. J Hep Bil Pancr Surg. 1995;2:145–51.
12) Kitagawa S, Murakami G, Hata F, Hirata K. Configuration of the right portion of the caudate lobe with special reference to identification of its right margin. Clin Anat. 2000;13(5):321–40.
13) Kogure K, Kuwano H, Yorifuji H, Ishikawa H, Takata K, Makuuchi M. The caudate processus hepatic vein: a boundary hepatic vein between the caudate lobe and the right liver. Ann Surg. 2008;247(2):288–93.
14) Cho A, Okazumi S, Takayama W, Takeda A, Iwasaki K, Sasagawa S, et al. Anatomy of the right anterosuperior area (segment 8) of the liver: evaluation with helical CT during arterial portography. Radiology. 2000;214(2):491–5.
15) Takayama T, Tanaka T, Higaki T, Katou K, Teshima Y, Makuuchi M. High dorsal resection of the liver. J Am Coll Surg. 1994;179(1):72–5.
16) 谷崎 裕志,竜 崇正,趙 明浩,河野 至明.Segment IX の胆管枝に関する研究 胆管造影 CT を用いて.胆道. 2001;15(5):381–7.
17) 石山 秀一.Dorso-lateral paracaval portion(dl-PCP)の意義.胆と膵.2003;24:75–80.
18) Ohshima S. Volume analyzer SYNAPSE VINCENT for liver analysis. J Hepatobiliary Pancreat Sci. 2014;21(4):235–8. 19) Sakai H, Okuda K, Yasunaga M, Kinoshita H, Aoyagi S. Reliability of hepatic artery configuration in 3D CT angiography
compared with conventional angiography—special reference to living-related liver transplant donors. Transpl Int. 2005;18(5): 499–505.
The Boundary between the Caudate Lobe and the Right Liver:
Anatomical Evaluation of Portal and Biliary Branches in the Dorsal Sector
Using Multidetector Computed Tomography
Shuichi Aoki
1), Masamichi Mizuma
1), Naoaki Sakata
1), Hideo Otsuka
1),
Hiroki Hayashi
1), Kei Nakagawa
1), Takanori Morikawa
1), Fuyuhiko Motoi
1),
Takeshi Naitoh
1)and Michiaki Unno
1)1) Department of Surgery, Tohoku University Graduate School of Medicine
Purpose: Combined resection of the caudate lobe of the liver is necessary to achieve curative resection for perihilar
cholangiocarcinoma (PHCC). However, the location of the right boundary of the caudate lobe, which should be removed in the left-sided hepatectomy for PHCC, is still controversial. The aim of this study was to investigate the configuration of the portal and biliary branches in the dorsal sector using preoperative multidetector CT (MDCT) images in patients with PHCC and to clarify the optimal extent of the caudate lobe in the resection for PHCC.
Methods: Between January 2008 and May 2012, 110 consecutive patients with PHCC underwent preoperative
MDCT. The regions of the dorsal sector were classified as l-, b-, c-, d- and cp-region, according to the areas supplied by portal branches of the dorsal sector proposed by Couinaud, namely l, b, c, d and cp veins. The number and the ramification patterns of the portal (P-l, P-b, P-c, P-d, P-cp) and biliary (B-l, B-b, B-c, B-d, B-cp) branches in each region were investigated. Results: Eighty-five percent of P-d and 91% of B-d diverged from the anterior or posterior trunk, while 91% of P-c and 96% of B-c were from the left or right portal vein/hepatic duct. Ninety-eight percent of P-b and all of P-cp and P-l diverged from the first bifurcated branches. In addition, 92% of B-cp and all of B-b and B-l converged to the first bifurcated branches. Moreover, 61% of B-c and 35% of B-cp converged around the bifurcation of the anterior and posterior trunk. Conclusion: The boundary between c- and d-regions in the dorsal sector closely corresponds to the right margin of the caudate lobe, which was shifted to the d-region in 5–10% of cases. In left-sided hepatectomy with caudate lobectomy for PHCC, complete resection of the c-region and clearance of the confluence of the posterior/anterior bifurcation should be performed, while in cases in which the right margin shifted to the d-region, removal of the d-region should be considered.
Key Words: caudate lobe, computed tomography, hilar cholangiocarcinoma
[Jpn J Gastroenterol Surg. 2017;50(1):1-8] Reprint requests: Masamichi Mizuma Department of Surgery, Tohoku University Graduate School of
Medicine
1-1 Seiryomachi, Aobaku, Sendai, 980-8574 JAPAN
Accepted: July 27, 2016