髄膜腫は中枢神経系に発生する腫瘍の 1 つで,全脊髄
腫瘍の中でも神経鞘種についで頻度が多いとされ,全脊
髄腫瘍の 25~46%を占めるとの報告がある
1).また,髄
膜腫全体の中では脊髄に発生する割合は 1.2~12.5%と
報告されている.好発年齢としては,頭蓋内髄膜腫と同
様に脊髄髄膜腫も中年以降に多いとされ,18 歳以下の小
児に認めることは比較的少ない
2).病理学的には髄膜皮
性髄膜腫(meningothelial meningioma)などの WHO
grade Ⅰが一般的であり,異型性髄膜腫(atypical
menin-gioma
)を含む grade Ⅱが占める割合は成人における脊
髄髄膜腫のうち 4.7~7.2%と低く
3),さらに小児に関し
ては報告がきわめてまれである
2,4).このように,脊髄に
はじめに
外傷性脊髄損傷を契機に診断にいたった
小児脊髄異型性髄膜腫の 1 例
Pediatric Spinal Atypical Meningioma Revealed after Cervical Cord Injury
―A Case Report and Review of Literature―
山 名 慧 川 村 大 地 大 橋 洋 輝 谷 諭 村 山 雄 一
Satoshi Yamana, M.D., Daichi Kawamura, M.D., Hiroki Ohashi, M.D., Ph.D., Satoshi Tani, M.D., Ph.D., Yuichi Murayama, M.D., Ph.D.
Abstract
Spinal atypical meningiomas in pediatric patients are very rare, and no consensus exists
regard-ing their characteristics, treatment, and prognosis. We report a case of this type of tumor in a 16‒
year‒old boy who had experienced a gradual decline in muscle strength for several years and
devel-oped sudden quadriplegia after falling down the stairs. Computed tomography(CT)and magnetic
resonance imaging(MRI)showed a homogeneously enhanced tumor with calcifications inside the
spinal canal at C2 level, and the tumor was firmly compressing the spinal cord. Intraoperative
find-ings revealed that the tumor was highly calcified, but there was no spinal cord invasion. Since it was
an emergency, tumor resection was performed after initial preservation of adjacent roots, access to
the attachment site ventrolaterally after debulking, and precise dissection through a well‒defined
plane from the medulla, achieving Simpson grade II resection. Histopathological examination
revealed that most of the findings were consistent with meningothelial meningioma; however, some
features of atypical meningioma were present, and the MIB‒1 index was 11.2%. Therefore, the
lesion was considered an atypical meningioma. Two years after the surgery, there was no
recur-rence. Because of its pathological grade and no excision of the attachment dura, careful follow‒up is
required.
(Received:August 5, 2019;accepted:November 18, 2019)
Key words
atypical meningioma, spine, pediatric
東京慈恵会医科大学脳神経外科講座/Department of Neurosurgery, Jikei University School of Medicine
連絡先:〒105‒8471 港区西新橋 3‒19‒18 東京慈恵会医科大学脳神経外科講座 山名 慧(Address reprint requests to:Satoshi Yamana, M.D., Department of Neurosurgery, Jikei University School of Medicine, 3‒19‒18 Nishi‒shinbashi, Minato‒ku, Tokyo 105‒8471, Japan)
Case Report
症 例 報 告
発生した小児の atypical meningioma は非常にまれであ
り,その特徴や治療,予後などに関しては一定の見解が
得られていないのが現状である.
今回われわれは,外傷性脊髄損傷を契機に診断にい
たった小児の脊髄異型性髄膜腫(spinal atypical
meningi-oma)の 1 例を経験したため,文献的考察を加え報告す
る.
患 者:16 歳,男児
主 訴:四肢麻痺
既往歴・家族歴:特記すべきことなし
現病歴:当科初診の 3 年ほど前から,四肢の筋力低下
およびしびれを自覚するようになり,複数の医療機関を
受診していた.しかし原因が特定できず,その後も筋力
低下は徐々に進行していった.某日,階段から転落し,
その直後から四肢麻痺を認め,近医へ救急搬送された.
脊髄損傷〔American Spinal Injury Association(ASIA)分
類 B〕の状態であり,また頚髄 MRI で C2 椎体レベルに
腫瘍性病変を認めたため,当院へ転院搬送となり,同日
に緊急手術を行った.
来 院 時 現 症: 意 識 清 明,manual muscle testing
(MMT)
:三角筋 1/1,上腕二頭筋 2/2,上腕三頭筋 2/2,
手関節背屈 3/3,手関節屈曲 3/3,手指骨間筋 3/3,腸腰
筋 3/3,大腿四頭筋 3/3,前脛骨筋 3/1,腓腹筋 3/3,痛
覚:(右)C5‒T3 領域 3/10,T4‒T9 領域 6/10,(左)C5‒
T3
領域 6/10 程度に低下,T4 領域以下は正常.
深部腱反射:四肢ともに左右差なくすべて亢進.
病的反射:Babinski 徴候両側陽性,膀胱直腸障害(肛
門括約筋は弛緩していたが,感覚はわずかに保持).
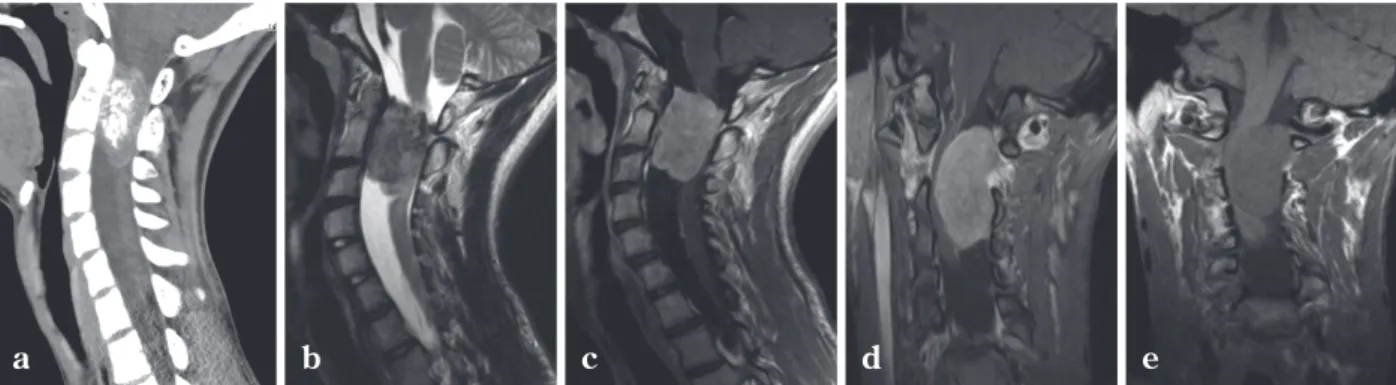
放射線学的所見:頚椎 CT では,C2 椎体レベルの脊髄
腹側に石灰化を伴う腫瘍性病変を認め,脊柱管の拡大を
伴っていた.頚髄の単純 MRI では T1 強調画像で等信号,
T2
強調画像で等信号(一部,石灰化を示唆する低信号)
を呈し,造影 MRI では均一に造影効果を伴う硬膜内髄外
腫瘍が,腹側および左外側から脊髄を強く圧排してい
た.腫瘍の一部は,C1/2 レベルで左椎間孔内へ浸潤して
いた(Fig. 1).
手術所見:全身麻酔下で transcranial(motor evoked
potential
(MEP)モニタリングを行った.腹臥位で,C1~
C4
の椎弓を一塊にして切除し,硬膜を露出した.硬膜切
開を行うと,くも膜下に腫瘍を認め,その背側を左 C2
神経根が走行していた.さらに,腫瘍の圧迫により著明
に菲薄化した脊髄を認めた.腫瘍は石灰化により非常に
固く,SONOPET
®(Stryker 社)を用いて内減圧を行い
ながら,硬膜との付着部を確認し,腫瘍を剝離した.腫
瘍の一部は左 C1/2 の椎間孔内に進展していたが,この
部位も含めて肉眼的に全摘出した.なお,脊髄や神経根
への浸潤は認めなかった.MEP モニタリングでは,右前
脛骨筋と両側腓腹筋を除いて腫瘍摘出後に波形の改善を
認めた.術中所見より髄膜腫と考え,付着部硬膜を凝固
し,Simpson grade Ⅱで摘出を終了した(Fig. 2).
病理所見:摘出した腫瘍検体を病理検査に提出し,
Hematoxylin‒Eosin(HE)染色および免疫染色を行った.
HE
染色では,大部分に meningothelial meningioma に特
徴的な渦巻き状の細胞配列(whorl formation)や砂粒体
(psammoma body)を認めたが,一部では,N/C 比の高
い細胞のパターンのない増殖や好中球浸潤を認め,免疫
染色では一部が MIB‒1 index 11.2%と高値を示したこと
から,atypical meningioma と診断された(Fig. 3).
経 過:術後約 2 週間のリハビリテーションにより,
症例提示
Fig. 1 Computed tomography(CT)scan and magnetic resonance imaging(MRI)in the initial presentation a :Sagittal CT shows a tumor with calcification and an enlargement of the spinal canal at C2 level.
b ~ e :Sagittal T2‒weighted MRI(b), sagittal/coronal T1‒weighted MRI with gadolinium enhancement(c, d), and coronal T1‒weighted
MRI(e)show the intradural extramedullary tumor with homogeneous enhancement, which strongly presses the spinal cord from the ventral and left lateral sides.
四肢筋力は MMT 4/5 程度まで改善を認めた.さらなる
回復を目指しリハビリテーション病院へ転院し,MMT
5/5 まで改善した.受診前よりも ADL は向上し,明らか
な後遺症も認めていない.現在のところ,術後 1 年 6 カ
月が経過しているが,画像上も再発を認めておらず,放
射線治療などの後療法は行っていない(Fig. 4).
髄膜腫はくも膜細胞を発生母地とする腫瘍で,わが国
における原発脳腫瘍のうち 26.4%を占め,最も頻度の高
い腫瘍とされている
5).好発年齢として 50~60 歳前後の
中年者に多くみられるが
2),小児の占める割合は 1.5~
2
%と非常に少ない
6).小児脳腫瘍全体でみても,髄膜腫
はわずか 1~4%ともいわれており
7),neurofibromatosis
type 2(NF‒2)に関連したものを除くと,その数は非常
に少ないとされる
8).
一般に髄膜腫の大半は頭蓋内に発生するが,脊髄や眼
窩内などに発生することもあり,とりわけ脊髄に発生す
るものは 1.2~12.5%とされ,小児髄膜腫にかぎれば,脊
髄に発生する頻度は 4~10%との報告がある
2,9).脊髄髄
膜腫の発生部位として,成人例では胸椎に発生すること
が多いとする報告が多く,その割合は 64~84%を占め,
頚椎,腰椎はそれぞれ 14~27%,2~14%とされる
10~12).
成人の atypical meningioma においても同様で,胸椎に多
いとの報告
11)がある一方で,小児例の報告は少ないなが
考 察
Fig. 2a:Intraoperative images in the microscope(the left side:cranial).
The spinal cord is very thinning(arrowhead)and pressed strongly by the tumor with calcification(black arrow:tumor, white arrow: left C2 dorsal root).
b :Final image after total resection of the tumor.
a
b
Fig. 3
Photomicrograph shows the typical findings of meningothelial meningioma, such as whorl formation and psammoma body(a:hematoxylin and eosin stain, ×20). In some photomi-crograph parts, cells with a high N/C ratio are pattern‒less proliferating and accompanied by neutrophil infiltration(hematoxylin and eosin stain, b:×100, c:×400). MIB‒1 label-ing index is 11.2%(d:×40).
aa
bb
ら,頚椎を好発部位であるとする報告が散見される
2,6).
性別では,一般的に頭蓋内髄膜腫は女性に多くみられる
ことが知られており,脊髄髄膜腫においても成人では女
性 が 男 性 の 2.5~4 倍 の 頻 度 で 発 症 す る と さ れ て い
る
10,12).一方,小児例では男児に比較的多いことが報告
されているが,その原因については明らかにされていな
い
2,6).このように,脊髄髄膜腫に関して小児例では成人
例と異なった疫学的特徴を有しているといえるが,文献
での報告がいまだ少なく,一定の見解を得るには十分と
はいえない.
2016 年に改訂された WHO 分類において,髄膜腫は 15
の subtype に分類されており,その多くは grade Ⅰに該
当し,進行は緩徐で良性腫瘍の性格を有している
13).そ
の中にあって,atypical meningioma は chordoid
meningi-oma
や clear cell meningioma とともに grade Ⅱの中間悪
性型に位置づけられ,増殖能が高く,組織への浸潤が懸
念される.成人の髄膜腫は,大部分が grade Ⅰであり,
grade
Ⅱは 4.7~7.2%,grade Ⅲは 1.0~2.8%を占める.
小児の髄膜腫も似た傾向をもち,grade Ⅰが 80.6%,
grade Ⅱと grade Ⅲはそれぞれ 10.4%,8.1%を占めると
報告されている
14).脊髄髄膜腫にかぎると,成人におけ
る atypical meningioma の割合は 4.7~7.2%との報告があ
るが,小児に関する疫学的報告は認めなかった
3).自験
例および過去に報告された grade Ⅱの小児脊髄髄膜腫 25
例をまとめたところ,80%以上を clear cell meningioma
が占めていることがわかった(Table 1).近年,髄膜腫
における遺伝子異常が注目されるようになり,脊髄髄膜
腫の中でも clear cell meningioma で SMARCE1 遺伝子の
異常による家族性発症に関連した報告が散見されるよう
になっている.その結果として,脊髄髄膜腫における
clear cell meningioma
の報告が増えているということも
考えられるが,小児脊髄髄膜腫の疫学的特徴として clear
cell meningioma
が grade Ⅱの多くを占めている可能性
が示唆される
8,15).日本脳腫瘍病理学会によれば,atypi-cal meningioma
の診断には,病理学的に細胞分裂像の増
加(強拡大 10 視野で細胞分裂像が 4 個以上)が認められ
るか,5 項目(細胞密度の上昇,腫瘍細胞の小型化と N/
C
比の増大,核小体の大型化,特徴的なパターンのない
シート状増殖,地図状の腫瘍細胞壊死)のうち 3 項目以
上が当てはまることが必要である
16).
本症例の病理検体では,grade Ⅰに分類される
menin-gothelial meningioma
の所見とされる whorl formation や
psammoma body
が大部分を占めたが,一部において腫
瘍細胞の N/C 比の増大やパターンのないシート状増殖
に加え,好中球の浸潤を伴っており,腫瘍壊死の可能性
を否定できなかったことから,atypical meningioma の診
断にいたった.
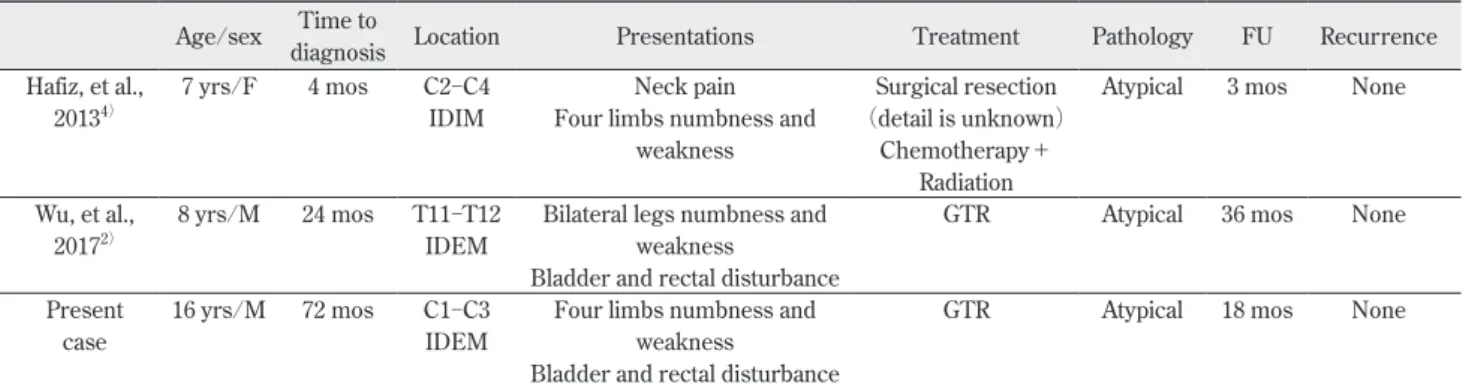
これまでに示したように,小児の spinal atypical
meningioma
はきわめてまれであり,われわれが渉猟し
得たかぎりで,同様の報告は本症例のほかに 2 例を認め
るのみであった(Table 2).その少なさゆえに,小児の
spinal atypical meningioma
に対する明確な治療指針は示
されていない.先に述べた grade Ⅱの小児脊髄髄膜腫 25
例においては,症例ごとに摘出の程度に差異を認めるも
のの,すべての症例において外科的摘出術が選択されて
いた.Wu ら
2)は,grade Ⅱの小児脊髄髄膜腫 5 例(spinal
atypical meningioma
はうち 1 例)の治療成績を報告して
おり,部分摘出に終わり最終的に死亡した clear cell
meningioma
の 1 例を除き,最長で 144 カ月の再発を認
めなかったとしている.また,成人における spinal
atyp-ical meningioma 17
例の治療成績を報告した Noh ら
11)に
よれば,頭蓋内原発髄膜腫の脊髄髄内転移に対して部分
摘出に終わった 2 例を除けば,Simpson grade Ⅰ/Ⅱで摘
出し得た症例に関しては再発を認めなかったとしてい
る.こうした報告から,小児の spinal atypical
meningi-oma
においても,成人同様に手術加療を第一選択とし,
また可能なかぎり Simpson grade Ⅰ/Ⅱの摘出を目指す
ことが患者の長期予後に寄与する可能性が示唆される.
一方,手術以外の治療としては,放射線療法の報告が
みられる.部分摘出に終わった,あるいは再発をきたし
た症例においては,術後放射線療法が効果的という報告
がみられる一方で,効果がないとする報告も散見されて
おり,一定の見解が得られていない
2).前出の 25 例にお
いて,9 例で術後放射線療法が行われており,うち 2 例
では初回摘出術後ただちに放射線療法を行っているが,
そのどちらも再発を認めなかった.また,再発に対する
治療として放射線療法を行った 7 例では,再発後に死亡
転帰となった 1 例を除き,追跡期間中の再発は認めな
かった.こうしたことから,その後の長期経過における
再発の可能性は不明であるものの,術後放射線療法の有
効性も示唆される.しかしながら,放射線障害のリスク
があるため,放射線療法を行う際には十分に注意を要す
る
11).今後さらなる症例を重ね,全摘出が困難な場合に
おける手術以外の治療法を確立させていく必要がある.
術後の画像検査や外来通院のタイミングについて具体
的に言及した報告は認めなかったが,Wu ら
2)によれば,
grade
Ⅱの小児脊髄髄膜腫 5 例のうち,1 例において術後
5
年で再発を認め,最終的に死亡にいたったとされてい
る.このことから,本症例のように全摘出をなし得てい
ても,今後の経過で再発を認める可能性を念頭に置き,
注意深い経過観察を継続する必要があると考えられる.
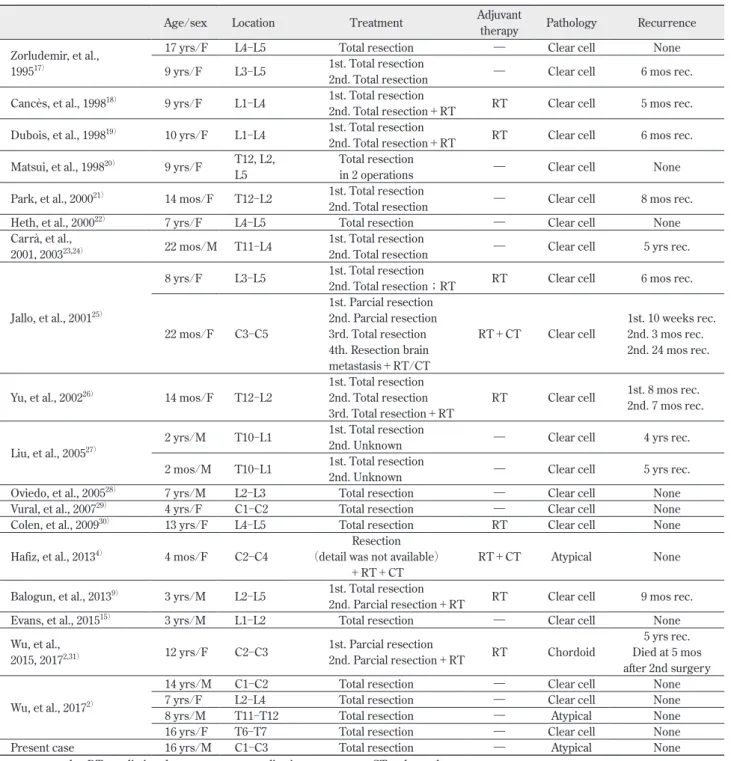
Table 1 Summary of the case reports of pediatric spinal meningioma, WHO grade Ⅱ
Age/sex Location Treatment Adjuvant therapy Pathology Recurrence Zorludemir, et al.,
199517)
17 yrs/F L4‒L5 Total resection ― Clear cell None 9 yrs/F L3‒L5 1st. Total resection2nd. Total resection ― Clear cell 6 mos rec. Cancès, et al., 199818) 9 yrs/F L1‒L4 1st. Total resection
2nd. Total resection+RT RT Clear cell 5 mos rec. Dubois, et al., 199819) 10 yrs/F L1‒L4 1st. Total resection
2nd. Total resection+RT RT Clear cell 6 mos rec. Matsui, et al., 199820) 9 yrs/F T12, L2,
L5
Total resection
in 2 operations ― Clear cell None Park, et al., 200021) 14 mos/F T12‒L2 1st. Total resection
2nd. Total resection ― Clear cell 8 mos rec. Heth, et al., 200022) 7 yrs/F L4‒L5 Total resection ― Clear cell None
Carrà, et al.,
2001, 200323,24) 22 mos/M T11‒L4 1st. Total resection2nd. Total resection ― Clear cell 5 yrs rec.
Jallo, et al., 200125)
8 yrs/F L3‒L5 1st. Total resection2nd. Total resection;RT RT Clear cell 6 mos rec.
22 mos/F C3‒C5 1st. Parcial resection 2nd. Parcial resection 3rd. Total resection 4th. Resection brain metastasis+RT/CT RT+CT Clear cell 1st. 10 weeks rec. 2nd. 3 mos rec. 2nd. 24 mos rec. Yu, et al., 200226) 14 mos/F T12‒L2 1st. Total resection2nd. Total resection
3rd. Total resection+RT
RT Clear cell 1st. 8 mos rec.2nd. 7 mos rec.
Liu, et al., 200527) 2 yrs/M T10‒L1
1st. Total resection
2nd. Unknown ― Clear cell 4 yrs rec. 2 mos/M T10‒L1 1st. Total resection2nd. Unknown ― Clear cell 5 yrs rec. Oviedo, et al., 200528) 7 yrs/M L2‒L3 Total resection ― Clear cell None
Vural, et al., 200729) 4 yrs/F C1‒C2 Total resection ― Clear cell None
Colen, et al., 200930) 13 yrs/F L4‒L5 Total resection RT Clear cell None
Hafiz, et al., 20134) 4 mos/F C2‒C4 (detail was not available)Resection
+RT+CT RT+CT Atypical None Balogun, et al., 20139) 3 yrs/M L2‒L5 1st. Total resection
2nd. Parcial resection+RT RT Clear cell 9 mos rec. Evans, et al., 201515) 3 yrs/M L1‒L2 Total resection ― Clear cell None
Wu, et al.,
2015, 20172,31) 12 yrs/F C2‒C3 1st. Parcial resection2nd. Parcial resection+RT RT Chordoid
5 yrs rec. Died at 5 mos after 2nd surgery Wu, et al., 20172)
14 yrs/M C1‒C2 Total resection ― Clear cell None 7 yrs/F L2‒L4 Total resection ― Clear cell None 8 yrs/M T11‒T12 Total resection ― Atypical None 16 yrs/F T6‒T7 Total resection ― Clear cell None Present case 16 yrs/M C1‒C3 Total resection ― Atypical None mos:months, RT:radiation therapy, rec.:recanalization, yrs:years, CT:chemotherapy
外傷性脊髄損傷を契機に診断にいたった小児脊髄異型
性髄膜腫の 1 例について報告した.小児脊髄異型性髄膜
腫は過去に 2 例の報告を認めるのみであり,非常にまれ
である.病理学的に悪性であることを念頭に置き,再発
や組織浸潤の可能性を考慮し,入念な経過観察が必要で
ある.
* 本論文の発表・写真の使用などにつき,患者から承諾を得 て掲載しています. 利益相反開示 著者は日本脳神経外科学会への COI 申告を完了していま す.本論文の発表に関して開示すべき COI はありません. 文 献1) Helseth A, Mork SJ:Primary intraspinal neoplasms in Norway, 1955 to 1986. A population‒based survey of 467 patients. J Neu-rosurg 71:842‒845, 1989
2) Wu L, Yang C, Liu T, et al:Clinical features and long‒term outcomes of pediatric spinal meningiomas. J Neurooncol
133:347‒355, 2017
3) Kleihues P, Cavenee WK:Pathology and Genetics of Tumors of the Nervous System. Lyon, IARC Press, 2000
4) Hafiz MG, Rahman MR, Yeamin MB:Intradural intramedullary spinal cord meningioma in a seven years old female child. Mymensingh Med J 22:180‒185, 2013
5) The Committee of Brain Tumor Registry of Japan:Report of brain tumor registry of Japan(1984‒2000)12th edition. Neurol Med Chir(Tokyo)49(Suppl):1‒25, 2009
6) Ben Nsir A, Boubaker A, Jemel H:Cervico‒occipital meningi-oma in a 5‒year‒old child:a case report. Turk Neurosurg
24:131‒134, 2014
7) Caroli E, Russillo M, Ferrante L:Intracranial Meningiomas in Children:Report of 27 New Cases and Critical Analysis of 440 Cases Reported in the Literature. J Child Neurol 21:31‒44, 2006
8) Gerkes EH, Fock JM, den Dunnen WF, et al:A heritable form of SMARCE1‒related meningiomas with important
implica-tions for follow‒up and family screening. Neurogenetics 17: 83‒89, 2016
9) Balogun JA, Halliday W, Bouffet E, et al:Spinal clear cell meningioma in a 3‒year‒old:a case report. Pediatr Neurosurg
49:311‒315, 2013
10) Galgano MA, Beutler T, Brooking A, et al:Spinal Meningio-mas:A Review. J Spine doi:10.4172/2165-7939.1000157, 2014 11) Noh SH, Kim KH, Shin DA, et al:Treatment outcomes of 17
patients with atypical spinal meningioma, including 4 with metastases:A retrospective observational study. Spine J 19: 276‒284, 2019
12) Gottfried ON, Gluf W, Quinones‒Hinojosa A, et al:Spinal meningiomas:surgical management and outcome. Neurosurg Focus 14:e2, 2003
13) Louis DN, Perry A, Reifenberger G, et al:The 2016 World Health Organization Classification of Tumors of the Central Nervous System:a summary. Acta Neuropathol 131:803‒ 820, 2016
14) Kotecha RS, Junckerstor RC, Lee S, et al:Pediatric meningi-oma:current approaches and future direction. J Neurooncol
104:1‒10, 2011
15) Evans LT, Van Hoff J, Hickey WF, et al:SMARCE1 mutations in pediatric clear cell meningioma:case report. J Neurosurg Pediatr 16:296‒300, 2015
16) 日本脳腫瘍病理学会:脳腫瘍臨床病理カラーアトラス 第 3 版.東京,医学書院,2012
17) Zorludemir S, Scheithauer BW, Hirose T, et al:Clear cell meningioma. A clinicopathologic study of a potentially aggres-sive variant of meningioma. Am J Surg Pathol 19:493‒505, 1995
18) Cancès C, Chaix Y, Karsenty C, et al:Clear cell meningioma: recurrent intraspinal tumor in a child. Arch Pediatr 5:758‒ 762, 1998
19) Dubois A, Sévely A, Boetto S, et al:Clear‒cell meningioma of the cauda equina. Neuroradiology 40:743‒747, 1998 20) Matsui H, Kanamori M, Abe Y, et al:Multifocal clear cell
meningioma in the spine:a case report. Neurosurg Rev 21: 171‒173, 1998
21) Park HC, Sohn MJ, Kim EY, et al:Spinal clear cell meningioma presented with progressive paraparesis in infancy. Childs Nerv Syst 16:607‒610, 2000
22) Heth JA, Kirby P, Menezes AH:Intraspinal familial clear cell meningioma in a mother and child. Case report. J Neurosurg
93(2 Suppl):317‒321, 2000
23) Carrà S, Drigo P, Gardiman M, et al:Clear‒cell meningioma in
おわりに
Table 2 Summary of the case reports of pediatric spinal atypical meningioma
Age/sex diagnosisTime to Location Presentations Treatment Pathology FU Recurrence Hafiz, et al.,
20134) 7 yrs/F 4 mos C2‒C4IDIM Four limbs numbness and Neck pain
weakness
Surgical resection (detail is unknown)
Chemotherapy+ Radiation
Atypical 3 mos None
Wu, et al.,
20172) 8 yrs/M 24 mos T11‒T12IDEM Bilateral legs numbness and weakness
Bladder and rectal disturbance
GTR Atypical 36 mos None Present
case 16 yrs/M
72 mos C1‒C3 IDEM
Four limbs numbness and weakness
Bladder and rectal disturbance
GTR Atypical 18 mos None
a 22‒month‒old male:a case report and literature review. Pediatr Neurosurg 34:264‒267, 2001
24) Carrà S, Drigo P, Gardiman M, et al:Clear cell meningioma in a 22‒month‒old male:update after five years. Pediatr Neuro-surg 38:162‒163, 2003
25) Jallo GI, Kothbauer KF, Silvera VM, et al:Intraspinal clear cell meningioma:diagnosis and management:report of two cases. Neurosurgery 48:218‒221, 2001
26) Yu KB, Lim MK, Kim HJ, et al:Clear‒cell meningioma:CT and MR imaging findings in two cases involving the spinal canal and cerebellopontine angle. Korean J Radiol 3:125‒129, 2002 27) Liu PI, Liu GC, Tsai KB, et al:Intraspinal clear‒cell meningi-oma:case report and review of literature. Surg Neurol 63:
285‒288, 2005
28) Oviedo A, Pang D, Zovickian J, et al:Clear cell meningioma: case report and review of the literature. Pediatr Dev Pathol
8:386‒390, 2005
29) Vural M, Arslantas¸ A, Ciftçi E, et al:An unusual case of cervical clear‒cell meningioma in pediatric age. Childs Nerv Syst 23: 225‒229, 2007
30) Colen CB, Rayes M, McClendon J Jr, et al:Pediatric spinal clear cell meningioma. Case report. J Neurosurg Pediatr 3:57‒60, 2009
31) Wu L, Yang T, Fang J, et al:Spinal chordoid meningioma in a child:A case report and review of the literature. Oncol Lett