【症例】感染性腹部大動脈瘤術後遠隔期に腋窩大腿動脈バイパスグラフト閉塞をきたした 1 例:下行大動脈inflowによる血行再建
3
0
0
全文
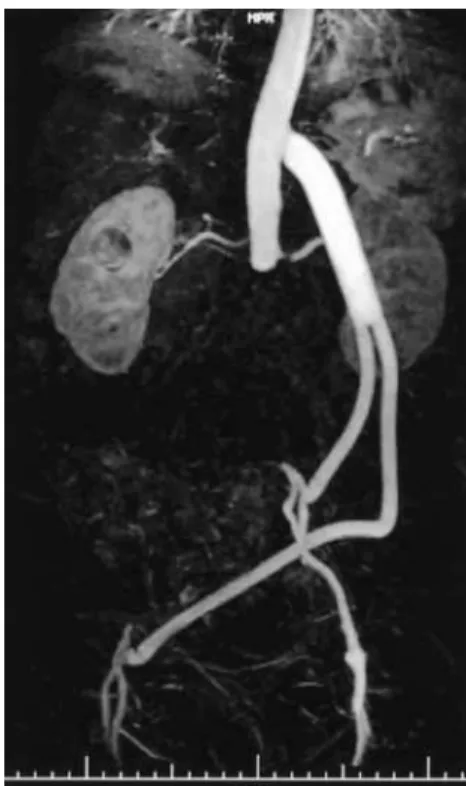
(2) 48. 日血外会誌 15巻 1 号. バイパスグラフトの血栓摘除のみでは再閉塞の危険が 高いことから緊急の処置は行わず,待機的にあらたな 血行再建を行うこととした.. SMA. 手 術:右下ひねり側臥位,第 7 肋間開胸,後腹膜 経路でアプローチした.強固な癒着が予想される腎動 脈下の大動脈断端部は露出せず,下行大動脈を露出. 末梢で左外腸骨動脈を露出し,右鼠径部で前回手術吻 合部を含めた右大腿動脈を露出した.ヘパリン投与 後,部分遮断を用いY字型人工血管(HemashieldTM 14 × 8mm, Boston Scientific, USA)を下行大動脈に端側で吻 合,左脚は左外腸骨動脈に端側で吻合,右脚は前回人 工血管末梢吻合部に狭窄をみとめなかったため右大腿 人工血管に端端で吻合した. 術後経過は良好であった.術後MRA (magnetic resonance angiography) (Fig. 1) でグラフトは良好に開存していた. 術後ABPIは右0.97,左1.00と改善した.術後13日目に自 宅退院となった.現在,再血行再建術後 9 カ月を経過 したが,下肢虚血症状なく経過観察中である.. 考 察. Fig. 1. Postoperative magnetic resonance angiography. The bypass graft was patent without stenosis.. 感染性腹部大動脈瘤の手術では,非解剖学的バイパ ス術は重要な治療選択肢の一つであり,われわれは明 らかに膿瘍形成のみられる症例では本術式を選択して. McCarthyら6)は,腹部感染人工血管や大動脈十二指腸瘻. いる.非解剖学的バイパス術は人工血管感染の危険は. の術後12例を含む21例に対する下行大動脈をinflowとし. 低下するものの,多くの場合用いられる腋窩−大腿動. た血行再建術を報告しているが,在院死亡はなく,4 年. 脈バイパス術は開存率が 5 年で60∼70%程度 2∼4)であ. の一次開存率は100%としている.Criadoらの32例の報. り,遠隔期グラフト閉塞を常に念頭に置かねばならな. 告 7)では,在院死亡6.25%,2 年の一次グラフト開存率. い.感染瘤術後の腋窩−大腿動脈バイパスグラフト閉. は86%であった.この報告のなかで,Criadoらはさらに. 塞の再手術の方法として,血栓摘除や再腋窩−大腿動. 他の報告例を集計して146例で検討した結果,対象には. 脈バイパス術も考えられたが,これらは遠隔成績に不. 感染人工血管抜去術後が18%存在し,その在院死亡率. 安が残る.一方,腎動脈下の腹部大動脈に吻合する解. は5.5%,5 年生存率67.5%,5 年一次グラフト開存率は. 剖学的再建では,癒着剥離に関して技術的な問題があ. 72.7%,二次開存率は82.7%であった.これらのなかに. る.また,大網充填,抗生剤治療で感染が落ち着いて. は遠位吻合を大腿動脈以下に吻合したものも含まれて. いるようであっても,かつて感染があった部位に人工. おり,われわれの症例のように遠位のrun-offが良好な. 血管をおくことはグラフト感染の問題からも決して有. 症例では開存率はよりよいものとなることが考えられ. 利な方法とはいえない.下行大動脈−両大腿動脈バイ. る.一方で,本術式選択にあたっては,強い動脈硬化. パス術は中枢吻合に際し癒着剥離の必要性がなく,ま. 性変化のためinflowとして不適当な下行大動脈,その部. た,径も十分に太く,バイパスのinflowとしては妥当な. 分遮断に伴う危険,開胸,後腹膜アプローチに伴う術. 血管と考える.グラフトルートも左側腹部後腹膜経路. 後の創部痛などのいくつかの問題もある.したがっ. におくことで,前回手術野とは十分に隔絶しえた.. て,全ての症例に適応となるわけではないが,自験例. 5). 本法はStevensonらによる1961年の報告 が最初であ. のように,比較的若年で,術前合併症の少ない症例に. り,以後,いくつかのまとまった報告 6∼8)がみられる.. は有効と考える.. 48.
(3) 2006年 2 月. 松崎ほか:下行大動脈inflowによる血行再建. 49. in axillofemoral bypass with externally supported knitted. 結 語. Dacron prosthesis in a Japanese hospital. J. Am. Coll. Surg., 186: 581-588, 1998.. 感染性腹部大動脈瘤に対して,瘤切除,腋窩−大腿. 5) Stevenson, J. K., Sauvage, L. R. and Harkins, H. N.: A. 動脈バイパスを施行した症例の遠隔期バイパスグラフ. bypass homograft from thoracic aorta to femoral arteries. ト閉塞に対し,下行大動脈をinflowとする血行再建術を. for occlusive vascular disease: Case report. Ann. Surg.,. 行い良好な結果を得た.. 27: 632-637, 1961. 6) McCarthy, W. J., Mesh, C. L., McMillan, W. D., et al.:. 文 献. Descending thoracic aorta-to-femoral artery bypass: Ten. 1) Moneta, G. L., Taylor, L. M. Jr., Yeager, R. A., et al.: Surgical. years’ experience with a durable procedure. J. Vasc. Surg.,. treatment of infected aortic aneurysm. Am. J. Surg., 175:. 17: 336-348, 1993.. 396-369, 1998.. 7) Criado, E. and Keagy, B. A.: Use of descending thoracic. 2) Onohara, T., Komori, K., Kume, M., et al.: Multivariate. aorta as an inflow source in aortoiliac reconstruction: Indi-. analysis of long-term results after an axillobifemoral and. cations and long-term results. Ann. Vasc. Surg., 8: 38-47,. aortobifemoral bypass in patients with aortoiliac occlusive. 1994.. disease. J. Cardiovasc. Surg., 41: 905-910, 2000.. 8) Barrett, S. G., Bergamini, T. M. and Richardson, J. D.:. 3) Martin, D. and Katz, S. G.: Axillofemoral bypass for aortoiliac. Descending thoracic aortobifemoral bypass: An alternative. occlusive disease. Am. J. Surg., 180: 100-103, 2000.. approach for difficult aortic revascularization. Am. Surg.,. 4) Mii, S., Mori, A., Sakata, H., et al.: Fifteen-year experience. 65: 232-235, 1999.. Late Graft Occlusion of Axillofemoral Bypass after the Repair of an Infected Aortic Aneurysm: Revascularization Using the Descending Aorta As an Inflow Source Kenji Matsuzaki, Norihiko Shiiya, Tomoyoshi Yamashita, Takashi Kunihara, Toshifumi Murashita and Keishu Yasuda Department of Cardiovascular Surgery, Hokkaido University Hospital Key words: Infected aneurysm, Extra-anatomical bypass, Descending aorta bifemoral bypass. We report an operative case of axillobifemoral bypass graft occlusion after repair of an infected aortic aneurysm. Successful revascularization was achieved by descending aorta bifemoral bypass grafting. A 58-year-old man was admitted to our hospital. He had acute limb ischemia induced by extraanatomical bypass graft occlusion, which had been conducted in a previous operation for an infected aortic aneurysm caused by Sallmonella. Surgical revascularization was performed with 7th intercostal thoracotomy and a retroperitoneal approach. Instead of the infrarenal aortic stump where the omentum was previously transferred, the descending aorta was chosen as an inflow source. A y-shaped Dacron prosthesis was anastomosed to the descending aorta, left external iliac artery, and right femoral graft. The postoperative course was uneventful. The descending aorta can be an alternative inflow source if the axillofemoral bypass graft was occluded in a patient who previously underwent operation for an infected infrarenal abdominal aortic (Jpn. J. Vasc. Surg., 15: 47-49, 2006). aneurysm.. 49.
(4)
図
関連したドキュメント
Tu be Saf et y & P ro du ct fe atu re s 静脈採血関連製品 特殊採血関連製品 静 脈 採 血 関 連 製 品 針 ・ア ク セ サ リ ー 動脈採血関連製品
私たちの行動には 5W1H
信心辮口無窄症一〇例・心筋磁性一〇例・血管疾患︵狡心症ノ有無二關セズ︶四例︒動脈瘤︵胸部動脈︶一例︒腎臓疾患
仙骨の右側,ほぼ岬角の高さの所で右内外腸骨静脈
10例中2例(症例7,8)に内胸動脈のstringsignを 認めた.症例7は47歳男性,LMTの75%狭窄に対し
右側縄腸骨動脈 仏9 5.3 4.3 4.7 4.8 左側線腸骨動脈 5.3 乱9 3.8 40
Keywords: homology representation, permutation module, Andre permutations, simsun permutation, tangent and Genocchi
49)Erlebach M, Wottke M, Deutsch MA, et al: Redo aortic valve surgery versus transcatheter valve-in- valve implantation for failing surgical bioprosthetic valves: Consecutive
