博士論文
平成 28 年度
臨床と創薬における
副作用マネジメントとその評価
田坂祐一
Multidirectal approaches to manage advers drug reactions and evaluation of the outcomes.
Yuichi Tasaka
Avoiding of adverse drug reactions (ADRs) is substantially important to provide safety medications. In this study, I examined the ways and means that are able to avoid/decrease ADRs in clinical site and drug development, respectively.
Pharmacists have increased the provision of pharmaceutical care services to patients. However, the financial benefit of various pharmaceutical interventions has not been well described. In chapter 2, I estimated the original economic impact associated with pharmaceutical interventions by an evidenced-based approach. I classified pharmaceutical interventions into 12 items, which included preventions of serious ADRs, and avoidance of drug interaction. The cost saving associated with preventions of serious ADRs was calculated as ¥2,140,000 per case based on the amount of costs that were paid by the Pharmaceuticals and Medical Devices Agency. Interventions to transvenous antimicrobial therapy were estimated to have a cost saving of ¥190,000 per case based on the literature in Japan. The rates of preventing serious ADRs related to chemotherapy orders, high-risk drugs and others were 5.21%, 3.91% and 2.6%, respectively, based on the literature in the United States. Using this rate, the values of intervention related to chemotherapy orders, high-risk drugs and others were ¥112,000, ¥84,000 and ¥56,000, respectively. The number of interventions was 209 per year, including 3 avoidances of serious ADRs. According to the number of interventions, I calculated that the total cost saving associated with pharmaceutical interventions was ¥22,816,000. This is the first study to estimate the economic impact associated with various pharmaceutical interventions of pharmacists in Japan. Evaluating the economic impact in relation to the pharmaceutical interventions is an important method for assessing the role of pharmacists.
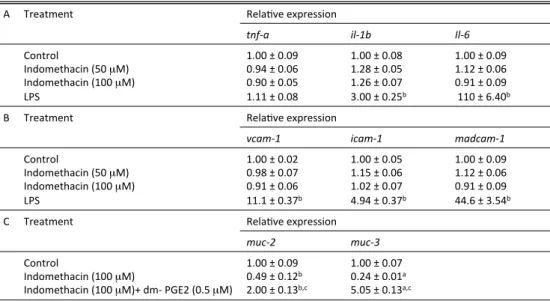
A number of clinical studies have shown that non-steroidal anti-inflammatory drugs (NSAIDs) exacerbate inflammatory bowel disease; however the molecular mechanism whereby this occurs remains unclear. NSAIDs inhibit cyclooxygenase (COX), which has subtypes COX-1 and COX-2. In chapter 3, I have examined the effect of various types of NSAIDs on the development of dextran sulfate sodium (DSS)-induced colitis, an animal model of inflammatory bowel disease. The DSS-induced colitis was worsened by administration of nonselective NSAIDs but not by COX-1 or COX-2 selective inhibitors. However, administration of a combination of both COX-1- and COX-2-selective inhibitors exacerbated the colitis. The intestinal level of PGE2 dramatically decreased in response to administration of COX-1- and COX-2-selective inhibitors, and exogenously administered PGE2 suppressed the exacerbation of colitis by NSAIDs. The expression of mucin proteins, which protect the intestinal mucosa, was suppressed by non-selective NSAIDs and this expression was restored by PGE2, both in vivo and in vitro. Intestinal mucosal cell growth was inhibited by non-selective NSAIDs and this cell growth was restored by PGE2, both in vivo and in vitro. This study provides evidence that inhibition of both COX-1 and COX-2 and the resulting dramatic decrease in the intestinal level of PGE2 is responsible for NSAID dependent
growth seems to be involved in this exacerbation and its suppression by PGE2.
Ulcerative colitis (UC) involves chronic inflammation of the large intestine. Several agents are used to treat UC, but adverse side effects are remaining problems. In chapter 4, I examined the effect of tropisetron as a new type of drug for UC using DSS-induced model of colitis in mice. I developed a DSS-induced colitis and calculated the Disease Activity Index and colon length. I measured myeloperoxidase activity and determined the protein level and mRNA level of cytokines in the colon. DSS-induced colitis was ameliorated by administration of tropisetron and PNU282987. Pre-administration of methyllycaconitine diminished the suppressive effect of tropisetron upon DSS-induced colitis. These findings suggested that α7 nicotinic acetylcholine receptors (α7 nAChRs) were related to the suppressive effect of tropisetron on DSS-induced colitis. Additionally, stimulation of α7 nAChRs decreased the colon level of interleukin-6 and interferon-γ upon DSS administration. Furthermore, stimulation of α7
nAChRs decreased macrophage infiltration, with expression of α7 nAChRs increased by DSS administration.
These results suggest that the underlying mechanism of this suppressive effect on DSS-induced colitis is via stimulation of α7 nAChRs and involves suppression of expression of pro-inflammatory cytokines. Tropisetron could be a new type of therapeutic agent for UC.
Idiopathic pulmonary fibrosis (IPF) is thought to involve inflammatory infiltration of leukocytes, lung injury induced by reactive oxygen species (ROS), in particular superoxide anion, and fibrosis (collagen deposition). No treatment has been shown to improve definitively the prognosis for IPF patients. Superoxide dismutase (SOD) catalyzes the dismutation of superoxide anion to hydrogen peroxide, which is subsequently detoxified by catalase.
Lecithinized SOD (PC-SOD) has overcome clinical limitations of SOD, including low tissue affinity and low stability in plasma. In chapter 5, I examined the effect of PC-SOD on bleomycin-induced pulmonary fibrosis.
Severity of the bleomycin-induced fibrosis in mice was assessed by various methods, including determination of hydroxyproline levels in lung tissue. Intravenous administration of PC-SOD suppressed the bleomycin-induced increase in the number of leukocytes in bronchoalveolar lavage fluid. Bleomycin-induced collagen deposition and increased hydroxyproline levels in the lung were also suppressed in animals treated with PC-SOD, suggesting that PC-SOD suppresses bleomycin-induced pulmonary fibrosis. The dose-response profile of PC-SOD was bell-shaped, but concurrent administration of catalase restored the ameliorative effect at high doses of PC-SOD.
Intratracheal administration or inhalation of PC-SOD also attenuated the bleomycin-induced inflammatory response and fibrosis. The bell-shaped dose-response profile of PC-SOD was not observed for these routes of administration. I consider that, compared with intravenous administration, inhalation of PC-SOD may be a more therapeutically beneficial route of administration due to the higher safety and quality of life of the patient treated with this drug.
Through these studies, I propose the importance of providing the safe medication by the multiple approaches; to avoid the avoidable ADRs and detect ADRs in an early phase not to make that serious; to clarify the cause of ADRs and establish the safety use of the medicine; to make the safety and effective medicine with lower risks of ADRs; to provide safety and effective medication by devising of route of administration. I hope that outcomes of these studies would improve quality of life of the patients.
目 次
頁
Summary. 1
目次 3
略語 5
第1章 序論 7
第2章 薬剤師による薬学的介入から得られる医療経済効果の推算 第1節 緒言 10
第2節 薬学的介入の定義とプレボイド報告 11
第3節 薬学的介入の分類 12
第4節 医療経済効果の推算 13
第5節 年間の医療経済効果の推算結果 15
第6節 薬学的介入の内訳 16
第7節 考察 19
第3章 非ステロイド性抗炎症薬の潰瘍性大腸炎に対する効果の解明 第1節 緒言 21
第2節 DSS腸炎に対する種々のNSAIDsの効果 23
第3節 NSAIDsによるDSS腸炎悪化に対するPGE2の効果 26
第4節 NSAIDsによるDSS腸炎悪化における炎症性サイトカイン,細胞接着分子,および ムチンタンパクの関与 27
第5節 NSAIDsによるDSS腸炎悪化における腸粘膜細胞死および細胞増殖の関与 31
第6節 考察 34
第7節 実験材料および実験方法 38
第1節 緒言 43
第2節 DSS腸炎に対するトロピセトロンの効果 45
第3節 トロピセトロンによるDSS腸炎抑制作用におけるα7 nAChRsの関与 47
第4節 α7 nAChRs刺激によるDSS腸炎抑制効果における炎症性サイトカインの関与 50
第5節 大腸におけるα7 nAChRsの発現とマクロファージの局在に関する検討 52
第6節 考察 54
第7節 実験材料および実験方法 58
第5章 レシチン化SODの特発性肺線維症に対する効果の検討 第1節 緒言 62
第2節 BLM肺線維症に対するPC-SODの効果 65
第3節 BLM肺線維症に対するPC-SODの改善効果のメカニズムの解明 69
第4節 BLM肺線維症に対するPC-SODの改善効果に対するカタラーゼ同時投与の効果 71
第5節 BLM肺線維症に対するPC-SODの新しい投与法の効果 74
第6節 考察 79
第7節 実験材料および実験方法 82
第6章 総括と展望 87
謝辞 89
参考文献 91
略 語
ADRs adverse drug reactions
Akt v-Akt Murine Thymoma Viral Oncogene
α7 nAChRs α7 nicotinic acetylcholine receptors BALF bronchoalveolar lavage fluid
BLM bleomycin
BrdU bromodeoxyuridine
COX cyclooxygenase
DAB 3, 3′-diaminobenzidine
EMT epithelial-mesenchymal transition ERK extracellular signal-regulated kinase DMBA 4-(dimethylamino)-benzaldehyde DSS dextran sulfate sodium
GAPDH glyceraldehyde-3-phosphate dehydrogenase 5-HT3R 5-hydroxytryptamine-3 receptor
HPLC high-performance liquid chromatography IBD inflammatory bowel disease
ICAM intercellular adhesion molecule
IFN Interferon
IL Interleukin
IPF idiopathic pulmonary fibrosis
LPS lipopolysaccharide
MAPK mitogenactivated protein kinase
MRSA methicillin-resistant staphylococcus aureus
NAC N-acetylcysteine
NSAIDs non-steroid anti-inflammatory drugs
PMDA Pharmaceuticals and Medical Devices Agency
PC-SOD lecithinized superoxide dismutase(lecithin; i.e. phosphatidylcholine)
PGE2 prostaglandin E2
PGs prostaglandins
PI3K phosphatidylinositol 3-kinase
QOL quality of life
ROS reactive oxygen spaces
TNBS 2,4,6-trinitrobenezene sulfonic acid TUNEL TdT-mediated dUTP nick end labeling TNF Tumor Necrosis Factor
UC ulcerative colitis
VCAM vascular cell adhesion molecule
第 1章 序 論
医薬品による副作用 (adverse drug reactions: ADRs) の回避あるいは早期発見による重篤化の回避は,
安全な薬物療法を行ううえで最も重要なことの1つである.米国におけるメタ解析1では,副作用が重 篤または致命的なものに至る割合はそれぞれ6.7%,0.32%であり,入院患者の15.1%に医薬品による何 らかの副作用が生じていることが報告されており,近年の報告2においても同様の数値が示されている.
また,米国において医薬品の副作用を経験した患者はそうでない患者に比べ死亡率の上昇,入院期間の
延長が報告されており3,生じるコストは年間1.56億~4億ドルにのぼると報告されている4, 5.本邦に おいても医薬品医療機器総合機構 (Pharmaceuticals and Medical Devices Agency: PMDA) による平成23 年度の医薬品副作用被害救済給付支給件数は959件であり,その費用は20億5,838万9千円である(独 立行政法人 医薬品医療機器総合機構ホームページ (www.pmda.go.jp)).これらのことから,医薬品によ る副作用を回避または軽減すること,すなわち医薬品による副作用のマネジメントは安全な薬物療法を 提供することに加えて医療経済的にも重要であると考えられる.
医薬品による副作用のマネジメントは臨床現場における副作用マネジメントと創薬に活かすべき副 作用マネジメントの2つに大別することができる.臨床現場における副作用マネジメントは回避可能な 副作用の予防,あるいは早期発見による重篤化の回避である.薬物相互作用による二次性の重篤な副作 用は高齢者,多剤併用,精神科領域,不適切な処方および複数の処方医の条件下で高頻度に発生するこ とが報告されている 6.また,腎機能が低下した患者に対する常用量の腎排泄型薬剤の使用は,代謝の 遅延に伴う副作用の増強を引き起こすことが考えられるが,実際の臨床現場では腎機能に応じた適切な 投与量となっていないケースも散見される 7.薬剤師は疑義照会および処方提案を介して薬物相互作用 の軽減や,薬物治療モニタリング (therapeutic drug monitoring : TDM) を含めた患者の腎機能に応じた薬 剤投与量の推奨を行う.これらの薬物療法の最適化は,より安全かつ有効な薬物療法を提案するもので ある.さらに,薬剤師は医薬品投与後のモニタリングを介して,副作用の早期発見および重篤化防止を
QOL) を向上させることに加えて,医療費を削減させることができることが期待される.しかしながら,
本邦において薬剤師による個々の薬学的介入を医療経済的に評価した報告はない.そこで本研究では,
副作用のマネジメント(回避・軽減)による医療費の削減効果という観点から,臨床現場における薬剤
師による薬学的介入から得られる効果を医療経済的に評価することを試みた(第2章).
一方,創薬における医薬品による副作用のマネジメントは,医薬品による副作用の原因解明や副作用
の少ない医薬品の開発であり,患者のQOLを大きく向上させることが期待される.本研究では,① 非 ステロイド性抗炎症薬 (non-steroid anti-inflammatory drugs: NSAIDs) の炎症性腸疾患 (inflammatory bowel disease: IBD) に 対 す る 効 果 の 解 明 , ② ニ コ チ ン 性α7 ア セ チ ル コ リ ン 受 容 体 (α7 nicotinic acetylcholine receptors: α7 nAChRs) を標的とした新規潰瘍性大腸炎治療薬の検討,③ 肺線維症に対する レシチン化スーパーオキシドジスムターゼ (lecithinized superoxide dismutase: PC-SOD) の効果と安全な
投与方法の検討の3つのテーマに基づき,創薬における医薬品による副作用のマネジメントの観点から 検討を行った.
潰瘍性大腸炎 (ulcerative colitis: UC) は大腸に慢性の炎症を繰り返す難治性の疾患であり,本邦におい ては特定疾患に指定されている(厚生労働省ホームページ (http://www.mhlw.go.jp)).UC 発症の根本的 な原因は明らかにはなっていないが,UC は遺伝的要因や腸内細菌叢などの環境的要因に起因する免疫
の 異 常 亢 進 に よ り 発 症 , 悪 化 す る と 考 え ら れ て い る 8-10.NSAIDs は シ ク ロ オ キ シ ゲ ナ ー ゼ
(cyclooxygenase: COX) を阻害することにより優れた解熱・鎮痛作用を有する抗炎症薬であり,医療現場
では広く使用されている薬剤である.COX は炎症を惹起する生理活性物質であるプロスタグランジン
(prostaglandins: PGs) の生合成に必須の酵素であるため,NSAIDsはUCを改善すると考えられた.しか
しながら,実際にはUCを悪化させるという報告があり11-13,本邦では多くのNSAIDsの添付文書に慎 重投与としてUCが記載されている.一方で,COXにはCOX-1,COX-2のアイソザイムが存在し,COX-2 に関してはUCを悪化させるという報告と改善するという報告がともに存在し14-17,またCOX-1のUC に対する関与は不明であった.そこで本研究では, IBD の代表的な実験動物モデルであるデキストラ ン硫酸ナトリウム (dextran sulfate sodium: DSS) 腸炎モデルを用いて,種々のNSAIDsのIBDに対する効
果を検討した(第 3章).一方で,疫学的な研究から,喫煙者では非喫煙者に比べ UC の発症率が低い ことが分かっていた18, 19.タバコの主成分であるニコチンはUCの有効な治療薬になると考えられ,様々 な臨床試験が行われ,その有効性が示された.しかしながら,ニコチンには嘔気や頭痛といった副作用
のため,臨床応用されることはなかった20-22.近年,マクロファージに存在するα7 nAChRsの刺激作用 が抗炎症作用を発揮することが報告された23.このことはα7 nAChRs刺激薬がUCの有効な治療薬とな る可能性を示唆している.また,現在のUCの治療薬としてステロイド薬や免疫抑制剤,インフリキシ マブなどが使用されているが,その副作用が多いことなどが問題となっている8, 9, 24-26.そこで本研究で
は,既存の医薬品のなかで,副作用が少なく,かつα7 nAChRs刺激作用を有する薬剤であるトロピセト ロンに着目し,DSS腸炎モデルを用いて,その腸炎抑制効果とメカニズムについて検討を行った(第4 章).
特発性肺線維症 (idiopathic pulmonary fibrosis: IPF) は原因不明の間質性肺炎の総称であり,本邦にお
いて特定疾患に指定されている.IPF は間質性肺炎のうち 60%を占め,診断確定後の平均生存年数が
2.5–5年と予後が不良であること,および有効な治療薬がほとんどないことが問題であり27-29,新規治療
薬の開発が強く望まれている. これまでに,間質性肺炎患者の肺組織,血液,および気管支肺胞洗浄
液 (bronchoalveolar lavage fluid: BALF) 内 で ス ー パ ー オ キ シ ド ア ニ オ ン (O2-) な ど の 活 性 酸 素 種
(reactive oxygen spaces: ROS) の産生が亢進していることが報告されており,間質性肺炎の病態において
ROSが重要な役割を果たしていることが考えられる30-32.また,O2-の消去剤であるSODにレシチンを 結合した製剤である PC-SODは SODの欠点である半減期の短さと細胞親和性の低さを克服した製剤で
あり33, 34,有効なIPFの治療薬となりうることが期待される.そこで本研究では,肺線維症モデルであ
るブレオマイシン (bleomycin: BLM) 肺線維症モデルを用いてPC-SODの効果とそのメカニズム,およ び副作用の起こりにくい安全な投与法について検討を行った.(第5章).
第 2章 薬 剤 師 に よ る 薬 学 的 介 入 か ら 得 ら れ る 医 療 経 済 効 果 の 推 算
第1節 緒言
近年の医療現場において,特に病棟における薬剤師の役割は多様化し,さまざまな薬学的介入が行わ れている.持参薬の確認による処方提案,薬歴管理を行うことによる医薬品の投与量・流速等の確認や 薬物相互作用の回避,医療スタッフへの医薬品情報提供等を行うことにより,病棟における医薬品によ る安全性の向上が求められる.また,医薬品投与後の服薬指導を通じて,副作用モニタリングや患者の 状態に応じた処方提案などを行う.さらに,抗メチシリン耐性黄色ブドウ球菌 (methicillin-resistant
staphylococcus aureus: MRSA) 薬のTDMや外来がん化学療法における介入など,薬剤師の役割は医療現
場での医薬品による安全性を担保するうえで重要さを増してきている.
Hamblin らは米国の救急医療において,PharmD による継続的な薬学的介入により,副作用の回避や
その重篤化の回避等を通じて年間565,664ドルの医療経済効果があることを報告している 35.また,本 邦においては丹羽らが抗菌薬適正使用推奨プログラムを確立することにより,患者1人につき,1日あ
たり27,237円の医療経済効果があることを報告している36.しかしながら,本邦において薬剤師による
個々の薬学的介入を医療経済的に評価した報告はない.そこで本章では,副作用の回避・軽減による医 療費の削減効果という観点から,臨床現場における薬剤師による薬学的介入から得られる効果を医療経 済的に評価することを試みたので,その結果について述べる.なお,本章での結果は既に参考文献 37 で発表している.37
第2節 薬学的介入の定義とプレアボイド報告
第1節で述べたように,現在の医療現場においては様々な薬学的介入が行われており,そのアウトカ ムを一定の規律に基づき抽出し,評価することは非常に困難である.そこで本研究では,平成 24 年度 に愛媛大学医学部附属病院(以下,当院)が日本病院薬剤師会の定めるプレアボイド報告(日本病院薬
剤師会ホームページ (http://www.jshp.or.jp/))を行った計 209 件を薬学的介入と定義し,解析を行った.
プレアボイド報告は日本病院薬剤師会の定める副作用回避事例報告システム (Be PREpared to AVOID
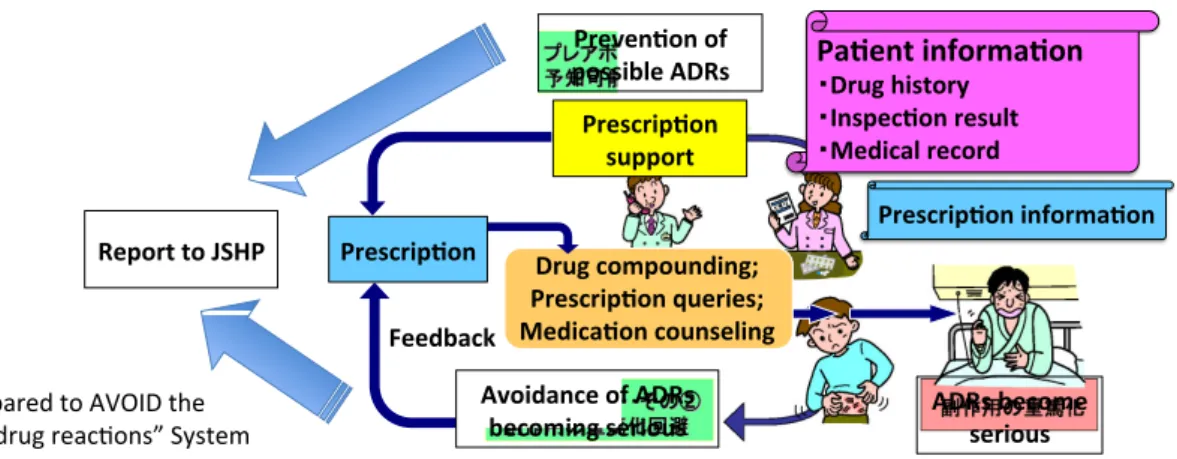
the adverse drug reactions system) (Fig. 1) の称呼であり, 薬剤師が薬物療法に直接関与し, 薬学的介入に より患者の不利益(副作用,相互作用,治療効果不十分など)を回避あるいは軽減した事例を集積する システムである.
Fig. 1. Outline of the “Be PREpared to AVOID the adverse drug reactions” system.
Hospital pharmacists report cases that have prevented the disadvantage of patients by pharmaceutical interventions to the Japanese Society of Hospital Pharmacists through “Be PREpared to AVOID the adverse drug reactions” system in Japan. This figure has been created partially modified what has shown by the Pharmaceutical Society of Japan(http://www.pharm.or.jp/).
“Be$PREpared$to$AVOID$the$
adverse$drug$reac9ons”$System ADRs%become%
serious Report%to%JSHP
Preven6on%of%
possible%ADRs% Pa6ent%informa6on%
Drug%history%
Inspec6on%result%
Medical%record
Prescrip6on%informa6on
Feedback
Prescrip6on%
support
Avoidance%of%ADRs%
becoming%serious Drug%compounding;%
Prescrip6on%queries;%
Medica6on%counseling Prescrip6on
JSHP Japanese$Society$of$Hospital$Pharmacists
第3節 薬学的介入の分類
Hamblinらは米国における薬学的介入を重大な副作用の回避,抗菌薬療法への介入および薬物相互作 用回避などの41の一次介入に分類している35.本研究では薬学的介入として定義した計209件の介入を
Hamblinらの報告を参考に,本邦における薬学的介入の評価に適すると考えられる以下の12種類に分類 した.
1)重大な副作用の回避または重篤化の回避
2)経静脈的な抗菌薬療法への介入
3)がん化学療法への介入
4)薬物相互作用回避
5)腎機能に応じた投与量推奨
6)注射薬配合変化防止
7)薬歴の聴取(抗血小板薬等の術前中止薬の確認などを含む)
8)その他の薬剤処方提案
9)モニタリング(検査)推奨
10)スタッフへの医薬品情報提供
11)他職種とのラウンド
12)副作用報告
第4節 医療経済効果の推算
前述した通り,平成23年度のPMDAによる医薬品副作用被害救済給付支給件数は959件であり,そ
の費用は20億5,838万9千円である.このことから,本邦においては医薬品による重大な副作用の回避
または重篤化の回避に対して平均2,140,000円の医療経済効果があると推算した(2,058,389,000円 ÷ 959 件 = 2,146,391円).また,本検討における重大な副作用とは添付文書上の重大な副作用あるいは警告,
重要な基本的注意等に記載のあるものとした.抗MRSA薬のTDMなどを介した経静脈的抗菌薬療法に 対する介入に関しては丹羽らの報告36を参考に定めた.すなわち,抗菌薬療法に適切に介入することに
より,1患者あたり1日27,237円の医療経済効果があることが報告されており,これに当院の抗MRSA 薬の平均投与日数である7日を考慮し,1件(患者1人)あたりの薬学的介入に対して190,000円の医 療経済効果があると定めた(27,237円 × 7日 = 190,659円). Hamblinらは薬物相互作用回避や腎機能
に応じた投与量推奨など個々の薬学的介入の 2.6%~5.21%が重大な副作用の回避または重篤化の回避 につながると報告している35.このことから本研究においても,個々の薬学的介入による医療経済効果
は重大な副作用の回避または重篤化の回避の2.6%~5.21%の医療経済効果があると考え,上記3~8の 薬学的介入を副作用発現リスクに応じてがん化学療法への介入,ハイリスク薬への介入,その他の薬物
療法への介入の3段階に分類し,それぞれの薬学的介入に対する医療経済効果を定めた(がん化学療法 への介入:112,000円;2,140,000円 × 5.21% = 111,827円,ハイリスク薬への介入:84,000円; 2,140,000
円 × 3.91%(2.6%と5.21%の中間値)= 83,924円,その他の薬物療法への介入 : 56,000円 ; 2,140,000
円 × 2.6% = 55,806円).なお,本検討におけるハイリスク薬は日本病院薬剤師会の定めるハイリスク
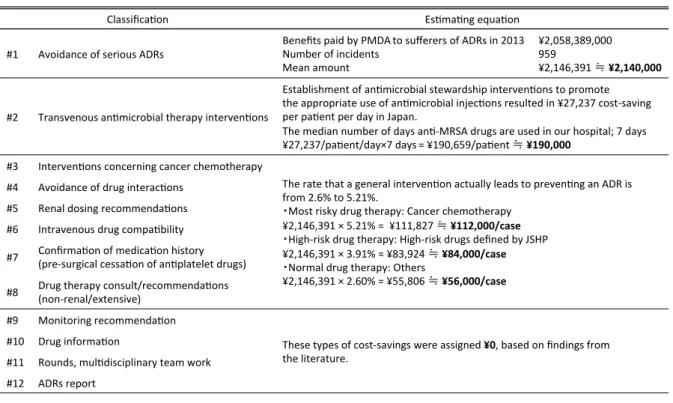
薬に関する業務ガイドライン(日本病院薬剤師会ホームページ (http://www.jshp.or.jp/))で記載のあるも のとした.また,今回の検討では Hamblin らの報告 35をもとに,処方変更に直接反映されない 9~12 の薬学的介入による医療経済効果は0円と定めた (Table 1).
Table 1. Classification of pharmaceutical interventions and estimation of economic impact.
Classifica(on Es(ma(ng.equa(on
#1 Avoidance.of.serious.ADRs Benefits.paid.by.PMDA.to.sufferers.of.ADRs.in.2013 Number.of.incidents.
Mean.amount.
¥2,058,389,000 959¥2,146,391. .¥2,140,000
#2 Transvenous.an(microbial.therapy.interven(ons.
Establishment.of.an(microbial.stewardship.interven(ons.to.promote.
the.appropriate.use.of.an(microbial.injec(ons.resulted.in.¥27,237.costSsaving.
per.pa(ent.per.day.in.Japan..
The.median.number.of.days.an(SMRSA.drugs.are.used.in.our.hospital;.7.days.
¥27,237/pa(ent/day×7.days.=.¥190,659/pa(ent. .¥190,000
#3 Interven(ons.concerning.cancer.chemotherapy.
The.rate.that.a.general.interven(on.actually.leads.to.preven(ng.an.ADR.is..
from.2.6%.to.5.21%...
Most.risky.drug.therapy:.Cancer.chemotherapy
¥2,146,391.×.5.21%.=..¥111,827. .¥112,000/case HighSrisk.drug.therapy:.HighSrisk.drugs.defined.by.JSHP
¥2,146,391.×.3.91%.=.¥83,924. .¥84,000/case Normal.drug.therapy:.Others
¥2,146,391.×.2.60%.=.¥55,806. .¥56,000/case
#4 Avoidance.of.drug.interac(ons.
#5 Renal.dosing.recommenda(ons.
#6 Intravenous.drug.compa(bility.
#7 Confirma(on.of.medica(on.history..
(preSsurgical.cessa(on.of.an(platelet.drugs).
#8 Drug.therapy.consult/recommenda(ons..
(nonSrenal/extensive)
#9 Monitoring.recommenda(on.
These.types.of.costSsavings.were.assigned.¥0,.based.on.findings.from..
the.literature..
#10 Drug.informa(on.
#11 Rounds,.mul(disciplinary.team.work.
#12 ADRs.report.
第5節 年間の医療経済効果の推算結果
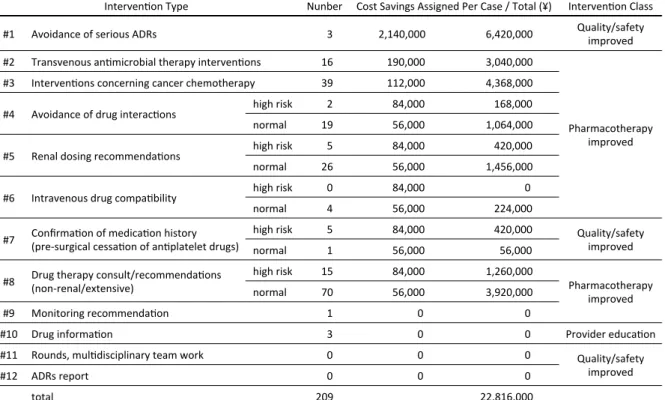
当院における平成24年度の薬学的介入計209件を上記12種類に分類した結果をTable 2に示す. 209 件の内訳は,重大な副作用の回避または重篤化の回避3件,経静脈的な抗菌薬療法への介入 16件,が ん化学療法への介入39件,薬物相互作用回避 21件(うちハイリスク薬 2件),腎機能に応じた投与量 推 31件(うちハイリスク薬 5件),注射薬配合変化防止4件(うちハイリスク薬0件),薬歴の聴取6 件(うちハイリスク薬5件),その他の処方提案85件(うちハイリスク薬15件),モニタリング(検査)
推奨1件,スタッフへの医薬品情報提供3件,多職種とのラウンド0件,副作用報告0件であった.ま た,これらの薬学的介入により得られる医療経済効果は合計22,816,000円と推算された.
Table 2. Estimation of annual economic impact.
Interven'on)Type) Nunber Cost)Savings)Assigned)Per)Case)/)Total)(¥)) Interven'on)Class)
#1 Avoidance)of)serious)ADRs ))))3 2,140,000 ))6,420,000 Quality/safety)
improved)
#2 Transvenous)an'microbial)therapy)interven'ons) ))16 )))190,000 ))3,040,000
Pharmacotherapy) improved
#3 Interven'ons)concerning)cancer)chemotherapy) ))39 )))112,000 ))4,368,000
#4 Avoidance)of)drug)interac'ons) high)risk ))))2 )))))84,000 )))))168,000
normal ))19 )))))56,000 ))1,064,000
#5 Renal)dosing)recommenda'ons) high)risk ))))5 )))))84,000 )))))420,000
normal ))26 )))))56,000 ))1,456,000
#6 Intravenous)drug)compa'bility) high)risk ))))0 )))))84,000 ))))))))))))))))0
normal ))))4 )))))56,000 )))))224,000
#7 Confirma'on)of)medica'on)history)) (preSsurgical)cessa'on)of)an'platelet)drugs))
high)risk ))))5 )))))84,000 )))))420,000 Quality/safety)) improved
normal ))))1 )))))56,000 )))))))56,000
#8 Drug)therapy)consult/recommenda'ons)) (nonSrenal/extensive)
high)risk ))15 )))))84,000 ))1,260,000
Pharmacotherapy) improved
normal ))70 )))))56,000 ))3,920,000
#9 Monitoring)recommenda'on) ))))1 ))))))))))))))0 ))))))))))))))))0
#10 Drug)informa'on) ))))3 ))))))))))))))0 ))))))))))))))))0 Provider)educa'on
#11 Rounds,)mul'disciplinary)team)work) ))))0 ))))))))))))))0 ))))))))))))))))0 Quality/safety) improved
#12 ADRs)report) ))))0 ))))))))))))))0 ))))))))))))))))0
total 209 22,816,000
第6節 薬学的介入の内訳
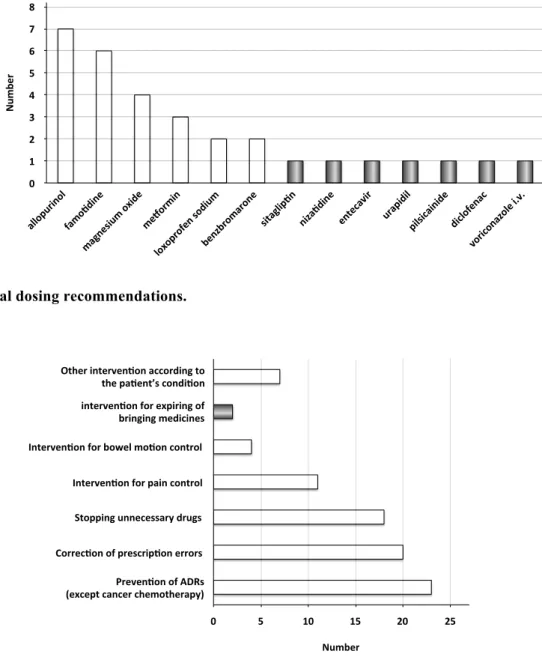
209件の薬学的介入のうち,重大な副作用の回避または重篤化の回避に該当する薬学的介入は3件で あり,HBs 抗原陽性患者に対するHBV感染未治療での化学療法開始に伴うB型肝炎急性増悪の回避1 件,grade 4 (Common Terminology Criteria for Adverse Events (CTCAE) v 4.0) の貧血患者に対する化学療法 開始による貧血の増悪の回避1件,絶食下でのステロイド内服患者におけるステロイド胃潰瘍の未治療 に伴う重篤な貧血の回避1件であった (Table 3).経静脈的な抗菌薬療法への介入は16件であり,対象 薬剤はバンコマイシン10件,テイコプラニン5件,メロペネム1件であった (Fig. 2).がん化学療法へ の介入は39件であり,抗がん剤投与量に関する介入 2件,支持療法等の処方もれの確認に関する介入 14件,支持療法の提案に関する介入21件,その他2件であった (Fig. 3).薬物相互作用回避に関しては 併用禁忌に該当するものがシクロスポリンとピタバスタチン1 件,併用注意に該当するものが 20件で あり, 代謝阻害に関するものが3件,吸収阻害に関するものが18件であった (Table 4).腎機能に応じ た投与量推奨(抗がん剤を除く)は31件であり,対象薬剤はアロプリノール 7 件,次いでファモチジ ン6件,酸化マグネシウム4件であった (Fig. 4).その他の処方提案に関しては副作用対策23件, 誤 処方・誤転記・処方もれに関する介入 20件, 同種同効果薬の重複を含む不要薬の中止 18件,疼痛コ ントロールに対する介入11 件,排便コントロールに対する介入4件,期限切れ医薬品の持参に対する 介入2件,ほかの諸症状に対する処方提案7件であった (Fig. 5).また,これらの薬学的介入の介入方 法のべ 237 件を分類分けした結果, 薬剤追加 67件 (28.3%),薬剤中止 45 件 (19.0%), 薬剤変更28 件 (11.8%) ,薬剤減量28件 (11.8%) が上位を占めた (Fig. 6).
Table 3. Avoidance of serious ADRs.
Case %Pharmaseu+cal%interven+on
Avoidance%of%re6ac+va+on%of%hepa++s%B%virus%(HBV)%from%under6treatment%in%
a%hepa++s%B%to%hepa++s%B%surface%(HBs)%an+gen6posi+ve%cancer%
chemotherapy%pa+ent
Defer%cancer%chemotherapy%and%start%oral%administra+on%
of%entecavir%
Avoidance%of%severe%anemia%in%a%cancer%chemotherapy%pa+ent%with%a%grade%4%
anemia Defer%cancer%chemotherapy%and%undertake%further%
inves+ga+ons%of%anemia%
Avoidance%of%severe%anemia%caused%by%administra+on%of%oral%steroids%in%a%
fas+ng%gastric%ulcer%pa+ent Start%oral%administra+on%of%proton%pump%inhibitor%
Fig. 2. Transvenous antimicrobial therapy interventions.
Fig. 3. Interventions concerning cancer chemotherapy.
Table 4. Avoidance of drug interactions.
10 8 6 4 2
0 12
Number meropenem
teicoplanin
vancomycin
25 20 15 10 5 0
Number Suppor.ve0therapy0recommenda.on0
Check0of0prepared0medicines Dosing0recommenda.on Others
subject(drug(1 subject(drug(2 Number cause(of(drug(interac5ons Contraindica5on(for(coadministra5on cyclosporine pitavasta5n 1 metabolic(inhibi5on
Combina5on(issue
levofloxacin magnesium(oxide 7
absorp5on(inhibi5on
cefdinir magnesium(oxide 4
minocycline magnesium(oxide 1
calcium(polystyrene(sulphonate magnesium(oxide 2
cefdinir ferrous(citrate 2
itraconazole lansoprazole 2
esomeprazole cilostazol 1
metabolic(inhibi5on
telaprevir nifedipine 1
Fig. 4. Renal dosing recommendations.
Fig. 5. Drug therapy consult/recommendations (non-renal/extensive).
Fig. 6. Method of intervention.
0 8
6
4
2 1 3 5 7
Number
allopur inol
famo 7dine
magnesium;o xide
me=
ormi n
benzbromarone sitaglip7
n niza7dine
entecavir
loxoprofen;sodium urapidil
pilsic ainide
diclofenac voriconazo
le;i.v.
interven'on)for)expiring)of)) bringing)medicines
0 Interven'on)for)bowel)mo'on)control
Interven'on)for)pain)control
Correc'on)of)prescrip'on)errors Stopping)unnecessary)drugs
Preven'on)of)ADRs)) (except)cancer)chemotherapy))
25 20 15 10 5 Other)interven'on)according)to)
the)pa'ent’s)condi'on
Number
Others
dispe nsing
,method, chang
e
Drug,informa4on, Dosage,met
hod,change,
Medica4on,counseling, Dosage,fo
rm,ch ange,
Add,monitoring, Increase
,dosag e,
Change,dose,regi men
,
Decrea sed,dosage, Change,drug, Drug,discon4nua4on, Add,drug, 0 60
40
20 10 30 50 70
Number
第7節 考察
本研究では,本邦において初めて薬剤師による個々の薬学的介入により得られる効果の医療経済的な 評価を試みた.一般的に医薬品の副作用により生じるコストを算出するためには個々の事例を解析する 必要があり,多種多様な薬剤と副作用に関して予めそのコストを算出しておくことは非常に困難である と考えられる.実際に,今回の検討では重大な副作用の回避または重篤化の回避に該当する薬学的介入 は3件であったが,介入を行わなかった場合の個々の転機は不明であり,それにより医療費も大きく異 なることから,実際に発生したと予想される経済効果を試算することはできない.そこで本研究では,
PMDAによる医薬品副作用被害救済制度に着目した.医薬品副作用被害救済制度は,医薬品が適正に使 用された条件下で発生した副作用に対して支払われる給付金である.従って,この平均額は本邦におけ る副作用により発生するコストを最も適切に表しているものの1つであると考え,重大な副作用の回避 または重篤化の回避に対して2,140,000円の医療経済効果を割り当てた.この金額はHamblinらの報告す る6,000ドル35に比べ高い金額となっているが,これはPMDAによる給付金には遺族年金等も含まれてい るためである. PMDAが厚生労働省管轄の独立行政法人であることを考慮すると,本副作用被害救済 給制度が現在の我が国の最も副作用回避を評価するのに適した制度であると考える.このことから,本 邦においては遺族年金を含めた医療経済効果を算出することが妥当であると考えた.
209件の薬学的介入を分析した結果,TDMを介した経静脈的な抗菌薬療法への介入はテイコプラニン5
件,バンコマイシン10件であり年間のTDM 回数に比べ非常に少ない結果であった.これは解析対象で あるプレアボイド報告として報告されたものが実際に介入を行い処方が変更されたものの一部であっ たこと,当院ではプレアボイド報告は1回のTDMごとではなく介入を行った患者ごとに行っていること によると考えられた.がん化学療法に対する介入では支持療法の提案や処方もれの確認が主であった.
これらの介入は重大な副作用発現頻度の高い抗がん剤の副作用を予防または軽減するものであり,ほか の薬学的介入に比べ高い医療経済効果を割り当てた妥当性は高いと考える.薬物相互作用回避は全介入
禁忌を抽出し,処方せんに印字するシステムを採用しており,調剤の段階で察知し疑義照会を行うこと によって未然に回避されているため,プレアボイド報告として報告されてこなかったためであると考え る.腎機能に応じた投与量推奨はアロプリノールおよびファモチジンが上位を占めたが,腎機能の低下 した患者に対するロキソプロフェンや酸化マグネシウムの他剤への変更も含まれており,腎機能悪化や 高マグネシウム血症といった副作用の未然回避に貢献していると思われる.その他の薬剤処方提案には がん化学療法以外の副作用対策,同種同効薬の重複に対する介入や処方もれに対する介入が上位を占め た一方で,疼痛コントロールや排便コントロールへの介入をはじめとする患者の状態に応じた積極的な 薬学的介入も含まれており,Hamblinらの報告35に基づき56,000円の医療経済効果を割り当てた.また,
今回の薬学的介入を介入方法別に分析した結果,最も多いものは薬剤追加であり,次いで薬剤中止であ った.薬剤を追加または中止することにより直接的に薬剤費の増減が発生するが,今回の検討では副作 用の予防につながる頻度に応じて医療経済効果を定めており,これらの薬剤費については検討から除外 している.
Lazarou らは医薬品による副作用のうち,50%は予防可能なものであることを報告している 1.また,
BondらはこのLazarouらの報告を加味すると,米国において副作用収集システムに登録している全米の
病院うちの約50%だけにおいても,予防可能な副作用を回避することにより年間300億ドルの医療経済 効果があると推算している 3.本邦においては医薬品の副作用によりどれだけの医療費が発生している かは不明であるが,米国と同様の頻度で副作用が発生し,回避できるものがあると仮定すると,薬学的 介入を行うことによる医療費の削減効果は多大なものであることが推察される.
このように本研究において,薬剤師による副作用回避に着目し,その効果について医療経済的に検討 を行った.近年の医療技術の進展や多様化に伴い,医薬品の安全使用と適正使用,最適な薬物療法の支 援等医療現場におけるリスクマネージャーとしての薬剤師の役割と責任は高まりつつある.これらの背 景からも薬剤師による薬学的介入を医療経済的に数値で示すことは,薬剤師の役割を新たな側面から評 価することのできる有効な手段であると思われる.
第 3章 非 ス テ ロ イ ド 性 抗 炎 症 薬 の 炎 症 性 腸 疾 患 に 対 す る 効 果 の 解 明
第1節 緒言
IBDは現代社会において大きな健康問題となっている.近年の研究からIBDは,活性化した好中球が 腸組織へと浸潤し,活性酸素種を産生することにより腸粘膜が傷害され,その結果,腸内細菌が腸粘膜 を通過して腸組織へと浸潤することにより引き起こされる腸における慢性の炎症性疾患であることが 示唆されている38.また,臨床におけるIBDの治療プロトコールを確立するため,および使用する薬剤 による偶発的なIBDの悪化を避けるためには,どのような種類の薬剤がIBDを改善または悪化させるか を知ること,そしてその基本的な分子メカニズムを理解することが重要である.そのため,実験動物モ
デル,特にDSS腸炎モデルを用いた検討は非常に有用であると考えられる39.
NSAIDsは,炎症を誘発する強い能力を有するPGsの合成に必須の酵素であるCOXの活性の阻害を介し
て抗炎症効果を発揮する.そのため,NSAIDsはIBDの治療に有効ではないかと考えられていた.しかし ながら,いくつかの臨床研究や実験動物モデルによる研究は,NSAIDsがIBDや実験腸炎モデルの症状を 悪化させることを示している40-43.これはPGsが腸粘膜においてムチンの産生促進作用,粘膜細胞の増殖 促進作用,粘膜細胞死阻害作用,および炎症性サイトカインの産生阻害作用などの種々のメカニズムを
通じた保護効果を持つことによるものであると考えられる42.また,PGsの前投与により実験腸炎モデル の発症が軽減すること44はこの考えを支持するものである.しかしながら,我々はこれまでに,胃粘膜 においてNSAIDsが直接,すなわちCOX阻害作用に依存しない方法で胃粘膜傷害を引き起こし,これが
NSAIDs胃潰瘍の形成に重要な役割を果たしていること示してきた45.さらに,いくつかの研究はNSAIDs
がIBDや実験腸炎モデルに対して安全であるという我々の見解と矛盾した結果を示している46, 47.
COXにはCOX-1とCOX-2という2つのサブタイプが存在する.COX-1は様々な組織において恒常的に 発現しており,ホメオスタシスの維持に重要な役割を果たしている.一方で,COX-2はIBD患者や実験
44, 48, 49
て安全なNSAIDsとしてCOX-2選択的な阻害薬が開発された.また,臨床や実験動物モデルにおいても
COX-2選択的な阻害薬は安全であることが示され, IBD患者や実験腸炎モデルに対して有効であるとい
う報告も示された14-17が,そのメカニズムは不明であった.さらに,いくつかの研究ではCOX-2選択的 な阻害薬はIBDや実験腸炎モデルを悪化させるという正反対の結果が示された11-13.一方で,IBDにおけ るCOX-1の関与は不明である.臨床現場ではNSAIDsがIBD患者に投与されることはしばしば起こること であり40,どのようなタイプのNSAIDs(例えばCOX-1やCOX-2選択的な阻害薬)がIBD患者に対して安 全であるのかを知ることは重要である.そこで,本研究では,種々のNSAIDsのCOX選択性に着目し,
DSS腸炎の形成に対する効果および,そのメカニズムについて検討を行った.なお,本章での結果は既 に参考文献50で発表している.50
第2節 DSS腸炎に対する種々のNSAIDsの効果
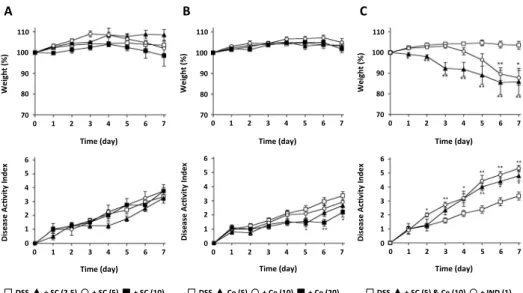
本検討において,DSS腸炎の程度は体重,下痢と血便をスコア化し合計したものであるdisease activity
indexや大腸の長さなど様々な指標を用いて測定を行った.まず,3% DSSを投与することによる腸炎の 形成に対するCOX-1選択的な阻害薬であるSC-560の影響を体重とdisease activity indexを用いて経時的に 測定した.その結果,3%DSSの投与はFig. 7に示す通り軽度の腸炎を惹起し,これは過去の報告と一致 するものであった51.SC-560の投与は最も高用量 (10 mg/kg) においてもDSS投与によるdisease activity
indexの上昇や体重の変化に影響を与えなかった (Fig. 7A).また,COX-2選択的な阻害薬であるセレコ キシブにおいても同様の検討を行ったところ,セレコキシブにDSS腸炎を悪化させる作用はなかった.
また,disease activity indexにおいてはセレコキシブ投与により軽度のDSS腸炎の改善が認められた (Fig.
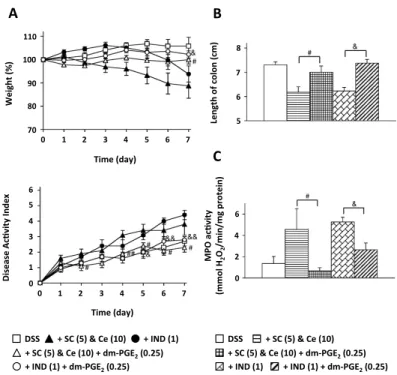
7B).次に,COX-1とCOX-2を同時に阻害した時のDSS腸炎に与える影響を検討するために,SC-560とセ
レコキシブ併用投与の検討を行った.その結果,DSS非処置群はSC-560とセレコキシブ併用投与は体重 に影響を与えなかった (data not shown) が, DSS処置群では体重減少に加えてdisease activity indexの上 昇を引き起こした (Fig. 7C).これまでの報告52によると,Fig. 7CにおけるSC-560またはセレコキシブの 濃度は,それぞれCOX-1またはCOX-2を阻害するために十分な濃度である.さらに,COX非選択的
NSAIDs(インドメタシン)を単独でDSS処理群に投与したところ,SC-560とセレコキシブ併用投与と同
程度の体重減少とdisease activity indexの上昇が認められた (Fig. 7C).また,SC-560とセレコキシブ併用 投与,あるいはインドメタシン投与によるDSS腸炎の悪化は,腸炎の程度の形態学的な指標として使用
される腸の長さの短縮においても確認された (Table 5).これら全ての結果から,COX-1とCOX-2を同時 に阻害することはDSS腸炎を悪化させることが示唆された.
この考えを確認するために,大腸のプロスタグランジンE2 (prostaglandin E2: PGE2) 量の測定を行っ た.まず始めに,real time RT-PCR法を用いて,COX-1とCOX-2のmRNAが大腸において発現してい
ることを確認した.その結果,DSSの投与によりCOX-2のmRNAの発現が上昇したが,COX-1のmRNA
変化しているのかを確認した.その結果,大腸のPGE2量はDSS投与開始後5日間かけて徐々に上昇し,
その後はDSS投与前と同程度まで低下した (Fig. 8B).また,DSS処理群における種々のNSAIDsが大 腸の PGE2量に与える影響を検討した結果,SC-560の投与により大腸の PGE2量の軽度の減少が認めら れた一方で,セレコキシブの投与による有意な影響はみられなかった (Fig. 8C).さらに,SC-560 とセ
レコキシブ併用投与は大腸の PGE2量を著しく低下させ,この低下はインドメタシンを投与した際と同 程度のものであった (Fig. 8C).一方で,Fig. 8Aおよび8Bで得られた結果は過去の報告48, 49と同様の結
果であったが,詳細な経時的変化のプロファイルはこれまでの報告12とは一致していない.これは実験
動物の種差とDSSの用量の違いによるものである可能性が考えられた.これらTable 5,Fig. 7,Fig. 8 で得られた結果をまとめると,NSAIDsによるDSS腸炎の悪化にはこの著しい大腸の PGE2量の減少が 重要であると考えられる.
Fig. 7. Effect of various NSAIDs on DSS-induced colitis.
ICR mice were treated with or without 3% DSS for 7 days. The indicated dose of each NSAID was administered daily. The indicated dose (mg/kg) of SC-560 (SC) (A, C), celecoxib (Ce) (B, C) or indomethacin (IND) (C) was administered daily. Body weight and disease activity index were measured daily. Values are mean ± S.E.M. (n=4–18). ⁎⁎P<0.01; ⁎P<0.05.
Weight'(%)
70 80 90 100 110
Weight'(%)
70 80 90 100 110
Weight'(%)
70 80 90 100 110
Time'(day)
0 1 2 3 4 5 6 7
Time'(day)
0 1 2 3 4 5 6 7
Time'(day)
0 1 2 3 4 5 6 7
Disease'Ac>vity'Index
0 1 2 3 4 5 6
Time'(day)
0 1 2 3 4 5 6 7
Time'(day)
0 1 2 3 4 5 6 7
Time'(day)
0 1 2 3 4 5 6 7
Disease'Ac>vity'Index
0 1 2 3 4 5 6
Disease'Ac>vity'Index
0 1 2 3 4 5 6
DSS +'SC'(2.5) +'SC'(5) +'SC'(10) DSS Ce'(5) +'Ce'(10) +'Ce'(20) DSS +'SC'(5)'&'Ce'(10) +'IND'(1)
A B C