直腸癌における神経周囲浸潤の臨床病理学的意義
岩本 一亜
1)斎藤 俊博
2)手島 伸
2)武田 和憲
2)鈴木 博義
2)野明 俊裕
1)荒木 靖三
1) 1) 大腸肛門病センター高野会くるめ病院 2) 仙台医療センター 目的:直腸癌に対する神経周囲浸潤(perineural invasion;以下,PNI と略記)の予後規定因子としての 意義を解析した.方法:直腸切除を行った直腸癌 412 例を検討し,1996~2005 年は後ろ向きに 2006~2010 年は前向きに検討した.結果:144 例(35.4%)で PNI が陽性であり,上部直腸癌の陽性率は 43.7%,下部 直腸癌は 24.7%であった.PNI 陽性症例の病理組織学的因子の多変量解析では PNI と上部直腸癌,リンパ 管侵襲,脈管侵襲および低分化胞巣間に相関がみられた.PNI 陽性の 3 年生存率と 5 年生存率はそれぞれ 56.2%と 37.3%であり,PNI 陰性はそれぞれ 79.6%と 72.6%であった.PNI のみられた症例は予後が不良で あった(P<0.001).Stage II 症例において,PNI 陰性の 5 年生存率が 82.7%に対して PNI 陽性は 44.0% (P=0.008)であり,PNI は N0 でも予後因子であることが示された.予後因子では,リンパ節転移,壁深 達度,PNI に有意差を認め,リンパ管浸潤や脈管浸潤に有意差は認めなかった.局所再発規定因子として, 壁深達度 T3/T4 と PNI に有意差を認めた.結語:直腸癌の PNI は予後および局所再発の危険因子であり, TNM分類の T 因子,N 因子を補填する因子としてリンパ管侵襲および脈管侵襲以上に臨床病理学的意義 は大きい. キーワード:直腸癌,神経周囲浸潤,再発予後因子,生存率はじめに
大腸癌の病期分類には AJCC(American Joint Committee on Cancer)1),Dukes,Astler-Coller classification
および JCCC(Japanese Classification Colorectal Carcinoma)などがあり,遠隔転移,壁深達度(T 因子)と リンパ節転移(N 因子)で分類された病期に基づく治療法を提示している.一方,National Comprehensive Cancer Network(以下,NCCN と略記)ガイドラインは組織形態である節外非連続胞巣を組み入れ,リン
パ節転移の亜分類 N1c と分類している2).2011 年改訂版(Rectum and Colon Version 3 2011)では神経周囲
浸潤(perineural invasion;以下,PNI と略記)を病理組織学的因子として記載することを推奨している. NCCNガイドラインはこのような新しい病理組織学的因子を用いて細分化することで効率的な治療法を提 言し,治療成績の向上を図っている.PNI に関して本邦では,1990 年代に直腸癌に対する自律神経温存側 方郭清の妥当性に関する報告が盛んに行われていた.その後,進行直腸癌の予後因子として検討されてい るが,臨床的意義は確立されていない.今回,NCCN ガイドラインに取り上げられた PNI の意義を自験直 腸癌にて検証したので報告する. 〈2013 年 4 月 24 日受理〉別刷請求先:岩本 一亜 〒 839-0865 久留米市新合川 2 丁目 2-18 大腸肛門病センター高野会くるめ病院
対象と方法
1996年 2 月から 2010 年 3 月の間に仙台医療センターにて切除され,病理組織学的診断の明確な直腸腺
癌 412 例を検討対象とした.臨床病理学的特徴および先進部組織形態:PNI,Budding と低分化癌胞巣の評 価を行った.切除標本を 10%ホルマリン液に固定後,腫瘍中心部を通る腸管縦軸方向の切片を作成し,HE 染色し光学顕微鏡にて組織検討を行った.
PNIの定義は Batsakis3)および Liebig ら4)が提唱するように endoneurium,perineurium そして epineurium
いずれかの層に癌浸潤がみられたものとし,Auerbach’s plexus,外輪筋の longitudinal intramuscular plexus あ るいは外縦筋と漿膜間 subserous plexus のいずれかにみられる癌浸潤を神経浸潤と判定した.PNI の確定診 断には腫瘍辺縁部の所見を重視し,神経周囲間隙,神経線維束内に癌細胞がみられる所見を PNI とし,4 段階に評価した.PNI を認めないを pn0,極めて軽度(全標本中に 1~2 個)の PNI を pn1(Fig. 1),pn1 と pn3 の中間程度の PNI を pn2(Fig. 2),極めて高度(多くの切片に病変)の PNI を pn3(Fig. 3)とし, pn1~3 を PNI 陽性とし,pn0 を陰性として判定した.また,S100 染色で神経を染色し,腫瘍細胞に占居さ れた神経を確認した(Fig. 4).Budding および低分化癌胞巣は大腸癌研究会の定義にしたがって,Budding は 5 個未満の癌細胞あるいは小腺管による浸潤病変を確認し,浸潤先進部において接眼レンズ 10 倍,対物
レンズ 20 倍(実視野面積 0.785 mm2)で最も多く Budding が含まれる 1 視野内に Budding が 0~4 個を grade
1,Budding が 5~9 個を grade 2,Budding が 10 個以上を grade 3 と分類した.grade 2 ないし grade 3 を
Budding陽性とし,grade 1 を Budding 陰性と判定した5).そのうちリンパ管侵襲ありのもの,癌と判定が不
能なもの,膿瘍などの炎症所見に付随しての組織形態をとった病変は除外した.低分化癌胞巣の評価は間 質浸潤を呈する癌胞巣の中で 5 個以上の細胞からなる腺腔形成の乏しい癌胞巣を検索し,接眼レンズ 10 倍,対物レンズ 4 倍にて 0~9 個の癌胞巣を grade A と判定し,10 個以上の癌胞巣を認めるものを grade B,
接眼レンズ 10 倍,対物レンズ 40 倍にて低分化癌胞巣が視野全体を占めるものを grade C と分類した6).
grade Bないし grade C を低分化癌胞巣陽性とし,grade A を陰性と判定した.壊死変性や炎症細胞浸潤など
により断片化した癌組織および“粘液湖”に浮遊する癌細胞は除外した. 病理組織学的評価は仙台医療センター病理診断科に依頼し,1996~2005 年の 191 例は retrospective に再 評価し,2006~2010 年の 221 例は切除標本の臨床組織診断時に追記し解析した.症例の観察期間は 30~ 3,900日で平均 2,112 日,中央期間は 1,940 日であった.また,3 年経過した症例は 282 例(68.4%),5 年 経過した症例は 196 例(47.6%)であった. 側方郭清の適応は腫瘍下縁が下部直腸に達する進行癌とし,両側自律神経を温存し大腸癌治療ガイドラ イン7)に従いリンパ節 263,273 および 283 は郭清し,293 は術前・術中に必要と判断した症例のみ郭清し た.本検討では下部直腸癌,肛門管癌 190 例中 119 例(62.6%),下部直腸癌,肛門管癌 stage II および IIIa, IIIbの 149 例中 99 例(66.4%)に側方郭清を施行した.また,stage IV 症例を除いた 345 例中,R0 手術を 319例(92.5%)に,R1 手術を 20 例(5.8%)に行い,R2 手術は 6 例(1.7%)であった. 統計学検定は,因子間の解析には χ2乗検定を用い,累積生存率に関しては Kaplan-Meier 法にて解析し
log lank検定を行った.また,多変量解析はロジスティック回帰分析を行った.統計ソフトは SPSS II for
Windowsを使用した.
結
果
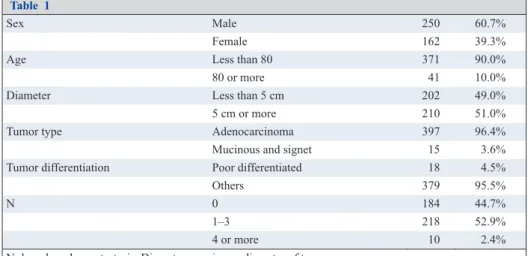
1.背景因子 男女比は 250:162 で男性が 60.7%と多く,80 歳以上の高齢患者は 41 例(10%)であった.占居部位は 上部直腸癌 222 例,下部直腸癌 186 例,肛門管癌 4 例であった.腫瘍径が 5 cm 以上の症例が 210 例(51%) を占め,397 例(96.4%)が腺癌でそのうち低分化腺癌は 18 例(4.5%)であった.リンパ節転移は 184 例(44.7%)が N0 であり,218 例(52.9%)が N1,N2 および N3 であった(Table 1). 2.PNI と病理組織学的因子の関連 PNI陽性は 144 例(35.4%)で,その内 pn1 は 114 例(27.7%),pn2 は 21 例(5.1%),pn3 は 9 例(2.2%) であった(Table 2).PNI の有無に性差はなかったが,占居部位では上部直腸癌の陽性率は 43.7%で,下部 直腸癌陽性率の 24.7%に比べ PNI は高率にみられた(P<0.001).進行度別にみると,壁深達度においては T3,T4 で有意に多く(P<0.001),リンパ節転移でも N3,N4 に高率で(P<0.001),病期別では進行例ほど 陽性率が高かった(P<0.001).リンパ管侵襲および静脈侵襲が高度な症例ほど神経浸潤の頻度が高く (P<0.001,P<0.001),主組織型では低分化腺癌が他の組織型に比べ PNI の頻度が高かった(P<0.005)(Table 3).
PNIと同様に評価した Budding は,grade 1 が 262 例(63.6%),grade 2 が 92 例(22.3%),grade 3 が 58
例(14.1%)であり,Budding 陽性率は 36.4%であった.また,低分化癌胞巣は grade A が 282 例(68.4%),
Fig. 1 Perineural invasion can be seen in human rectal cancer specimens that were stained with HE counterstain. Section of human rectal cancers was stained with hematoxylin and eosin. Cancer cell located and invaded slightly at the perineurium (pn1).
Fig. 2 Perineural invasion can be seen in human rectal cancer specimens that were stained with HE counterstain. Section of human rectal cancers was stained with hematoxylin and eosin. Cancer cell located and invaded moderately at the perineurium and within the epineurium (pn2).
Fig. 3 Perineural invasion can be seen in human rectal cancer specimens that were stained with HE counterstain. Section of human rectal cancers was stained with hematoxylin and eosin. Cancer cell located and invaded extremely at the perineurium and within the epineurium (pn3).
Fig. 4 This photomicrograph depicts perineural invasion in rectal cancer specimens. Section of human rectal cancers was stained with S-100 proteins. Tumor is located within the perineurium and has invaded the endoneurium. Nerve cells are stained and cancer cells occupy Auerbach’s plexus.
grade Bが 79 例(19.2%),grade C が 51 例(12.4%)と判定され,低分化癌胞巣陽性率は 31.6%であった (Table 2).
ロジスティクス回帰検定による単変量解析で,Budding,低分化癌胞巣と PNI に相関を認めた(P<0.001,
P<0.001).同様に PNI 陽性と他因子の相関を単変量解析すると,リンパ節転移 N2,N3 および N4,壁深達
度 s2/a2,si/ai,腫瘍占居部位 Ra,リンパ管侵襲 ly2/ly3,脈管侵襲 v2/v3 で有意差を認めた.PNI の出現と 各因子の関連をステップワイズ法で多変量解析すると,占居部位,リンパ管侵襲,脈管侵襲および低分化 癌胞巣が有意水準 5%以下で有意差を認めた.また,odd’s ratio はリンパ管侵襲 3.79,占居部位 2.60,脈管 侵襲 2.26,先進部低分化胞巣 2.04 で PNI の出現との関連が示された(Table 4).
3.PNI と予後
PNIを予後因子として Kaplan-Meier 法にて解析した結果,PNI 陰性では 3 年および 5 年生存率は 79.6%,
72.6%に対し,PNI 陽性はそれぞれ 56.2%,37.3%と予後不良であった(P<0.001)(Fig. 5).また,Stage II 症例において PNI 陰性は 5 年生存率 82.7%であり,PNI 陽性は 44.0%(P=0.008)であった(Fig. 6).同様 に,Stage III 症例では PNI 陰性の 5 年生存率は 69.1%であり,PNI 陽性は 47.6%(P=0.048)で有意差がみ られた.PNI はリンパ節転移にかかわらず予後規定因子であることが示唆された. N,T 因子を補填する因子としてリンパ管侵襲,脈管侵襲と PNI を比較するために,ステップワイズ法 で変数を選択して Cox 比例ハザードモデルを用いて多変量解析した.予後に関わる因子ではリンパ節転移 (P<0.001),壁深達度(P<0.001),PNI(P=0.001)に有意差を認めた(Table 5).観察期間中の再発は 31.1% にみられ,初回の再発部位は局所再発 8.0%,肝転移 8.3%および肺転移 6.1%であった.再発形式に関わる Table 1 Sex Male 250 60.7% Female 162 39.3%
Age Less than 80 371 90.0%
80 or more 41 10.0%
Diameter Less than 5 cm 202 49.0%
5 cm or more 210 51.0%
Tumor type Adenocarcinoma 397 96.4%
Mucinous and signet 15 3.6% Tumor differentiation Poor differentiated 18 4.5%
Others 379 95.5%
N 0 184 44.7%
1–3 218 52.9%
4 or more 10 2.4%
N: lymph nodes metastasis, Diameter: maximum diameter of tumor
Table 2 PNI pn 0 266 (64.6%) pn 1 114 (27.7%) pn 2 21 (5.1%) pn 3 9 (2.2%) Budding grade 1 262 (63.6%) grade 2 92 (22.3%) grade 3 58 (14.1%) Poorly component grade A 282 (68.4%) grade B 79 (19.2%) grade C 51 (12.4%) Poorly component: Poorly differentiated component at tumor front
因子を多変量解析し,局所再発に関わる因子として壁深達度(P<0.001,odd’s ratio 3.028)と PNI(P=0.003, odd’s ratio 2.602)に,肝転移に関わる因子ではリンパ節転移(P=0.001,odd’s ratio 3.920)に有意差を認 め,同様に肺転移では壁深達度(P=0.041,odd’s ratio 2.522)に有意差を認めた(Table 6).
考
察
癌統計では大腸癌罹患者数は近年横ばいもしくは減少傾向となっているが,2010 年度の部位別にみた癌 Table 3 PNI (–) PNI (+) P χ2 Sex Male 167 83 0.354 0.858 Female 101 61 Location Ra 125 97 <0.001 16.18 Rb 140 46 P 3 1 T T1 19 1 <0.001 24.3 T2 44 8 T3 185 116 T4 19 19Stage (JACC) I/II 145 28 <0.001 62.7
IIIa 68 41 IIIb 29 34 IV 26 41 N 0 151 33 <0.001 50.34 1, 2 106 87 3 9 16 4 or more 2 8
Lymphatic invasion None, mild 193 37 <0.001 81.50 Moderate, marked 75 107
Venous invasion None, mild 71 43 <0.001 43.24 Moderate, marked 97 101
Histological type Well 20 2 0.005 14.93 Moderately 230 127
Poorly 7 11
Mutinous 11 3
Others 0 1
JACC: Japanese classification of colorectal carcinoma, T: depth of tumor invasion, N: Lymph node metastasis
Table 4
Factor Univariate analysis Multivariate analysis Odd’s ratio P 95%CI Odd’s ratio P 95%CI N 4.069 <0.001 2.546–6.503 2.066 0.013 1.166–3.661 T 2.009 <0.001 1.322–3.053 1.10 0.739 0.530–1.570 Location (Ra) 2.437 <0.001 1.594–3.727 2.60 <0.001 0.232–0.634 Ly 7.440 <0.001 4.701–11.776 3.79 <0.001 2.142–6.560 V 0.242 <0.001 0.156–0.373 2.26 0.003 1.331–3.854 Budding 2.930 <0.001 1.920–4.472 1.513 0.228 0.771–2.966 Poorly component 2.911 <0.001 1.890–4.485 2.036 0.046 1.013–4.092 N: lymph node metastasis, T: depth of tumor invasion, Ra: upper rectum, Ly: lymphatic invasion, V: venous invasion, Poorly component: poorly differentiated component at tumor front
Fig. 5 Survival rates of patients who underwent rectal resection according to perineural invasion status: Prognosis of the PNI-positive group is significantly poorer than that of the PNI-negative group (P<0.001).
Fig. 6 Survival rates of patients who underwent curative surgery for rectal cancer penetrating muscularis propria and without lymph node metastasis according to perineural invasion status: Prognosis of the PNI-positive group is significantly worse than that of the PNI-negative group (P<0.001).
死亡率において女性では 1 位,男性では 3 位であり,外科治療を行う疾患のなかで最も多い悪性疾患であ る.しかし,本邦では 2005 年以降 furuolouracil の持続投与と oxaliplatin(L-OHP)や irinotecan を組み合わ せた FOLFOX,FOLFIRI の普及,また抗 VEGF(vascular endotherial growth factor)や抗 EGFR(epidermal
growth factor receptor)の恩恵により,切除不能,再発症例の生存期間が改善している8)9).
大腸癌は早期癌に対する手術適応と Stage III に対する補助化学療法の適応および Stage IV に対する化学 療法の選択は現在ガイドラインで示されている.しかし,Stage II 大腸癌に対する補助化学療法の効果は実 証されておらず10),適応症例を絞り込むことが課題となっている.また,Stage III に対する補助化学療法 の適応を明確にする必要がある11).さらに,直腸癌治療では側方郭清12)13),術前化学放射線療法14)や術後 補助化学療法の意義が欧米と本邦では一致せず,再発ハイリスク症例を判定し側方郭清,術前放射線化学 療法や術後補助化学療法の適応を明確にすることが必要である15).悪性度の高い Stage II,III 大腸癌の症 例を判定するには,主軸となる深達度とリンパ節転移での病期分類に新しい指標を加え細分化することが 必要である.しかし,病理組織学的形態を予後指標として加えることは,組織評価の負担が増え,予後評 価が煩雑となることも考慮すべきである. 新しい予後の指標として,従来の病期分類を補填する癌先進部や特異な組織形態の役割が注目されてき ている16).病理組織学的形態例えば Budding,低分化胞巣,PNI,節外非連続胞巣などは予後を評価する独 立した因子として報告されている17).評価因子を加える際は予後判定に独立した役割をもち,病理組織学 的評価と診断が簡便で評価者間の差が小さく,加えてその因子が一定の頻度で出現することが重要である. Table 5 P Exp 95% (CI) N <0.001 0.482 0.322 0.723 T <0.001 0.370 0.252 0.542 Ly 0.826 0.949 0.594 1.516 V 0.790 0.944 0.616 1.445 PNI 0.001 0.506 0.335 0.766
N: lymph nodes metastasis, T: depth of tumor invasion, Ly: lymphatic invasion, V: venous invasion, PNI: perineural invasion
Table 6
P Odd’s ratio 95% (CI) Local recurrence N 0.415 1.309 0.688–2.490 T <0.001 3.028 1.664–5.508 Ly 0.796 1.101 0.532–2.278 V 0.755 1.11 0.575–2.144 PNI 0.003 2.602 1.377–4.916 Liver metastasis N 0.001 3.92 1.700–9.036 T 0.519 1.293 0.592–2.824 Ly 0.39 1.56 0.563–4.319 V 0.323 1.563 0.638–3.826 PNI 0.722 1.164 0.503–2.694 Lung metastasis N 0.695 1.225 0.447–3.353 T 0.041 2.522 1.037–6.137 Ly 0.13 0.436 0.147–1.298 V 0.25 1.746 0.674–4.523 PNI 0.431 1.429 0.566–3.813 N: lymph nodes metastasis, T: depth of tumor invasion, Ly: lymphatic invasion, V: venous invasion, PNI: perineural invasion
1835年に Cruveilhier18)が神経への癌浸潤を報告し,1943 年には Seefeld ら19)が直腸癌の PNI を検討し局
所再発との関連を報告した.また,1963 年に Sheilds や Warren は前立腺癌症例で PNI の検討を行った20).
PNIはいくつかの癌種で浸潤形式の一つとして認識されている.神経鞘は三層からなり外膜,周囲膜およ び内膜で構成されている.最も高頻度にみられる PNI は周囲膜内に進展し神経鞘に浸潤したものである21). Liebigら4)は内膜,周囲膜で腫瘍が神経に接し,33%以上周囲膜を取り囲むか神経鞘に浸潤したものを PNI と定義した.しかし,周囲膜に包まれた末梢神経枝に癌細胞が浸潤するもの,あるいは周囲膜と神経線維 束の間の神経周囲間隙に癌細胞が浸潤するもの3)など定義は統一されていない.神経外膜は癌細胞の浸潤 を防御する機能を有するが,神経周囲膜は組織抵抗が脆弱な間隙であり,組織間を網羅するリンパ管様の ネットワークを有している22).腸管壁内外の神経線維は脈管に並走し,神経線維の分布する腸管壁層を進
展する.神経線維は粘膜に periglandular plexus,粘膜下層に submucosal plexus(Meissner’s plexus)を形成 し,内輪筋には circular intermuscular plexus を形成する.内輪筋と外輪筋の間には Auerbach’s plexus,外輪 筋には longitudinal intramuscular plexus が,さらに外縦筋と漿膜間には subserous plexus が形成されている.
神経叢は脈管に沿って互いに交通し,貫通枝に沿って腸管壁外へ向かい腸間膜に到達する23)24).
本邦では,直腸癌の自律神経温存手術に対して,白水ら25)は原発巣から PNI を介して温存する自律神経
に癌が遺残する可能性を指摘し,自律神経の周囲組織に浸潤する微小な癌病巣が注目された.予後因子と
して,上野ら26)は 364 例の直腸癌症例を解析し,筋層以深の extramural perineural invasion を検討し,筋層
からの距離 10 mm 以上もしくは 5 個以上/20 倍視野のものが不良な予後を規定すると報告している.また, 同様に大腸癌で筋層より 5 mm 以上離れる壁外脂肪層内に PNI を呈する病変があり,辺縁が不正な PNI 病 巣は予後と関連が深いと報告した.それらの解析から Budding や低分化癌胞巣のように T 因子,N 因子に 加えて悪性度を判定する副所見として注目されている.しかし,extramural perineural invasion と定義され る予後不良な PNI の頻度は 8.2%,壁外脂肪層内の癌進展病巣にみられる PNI の頻度は 2%以下と低率で, 定義に従った神経浸潤の検出は煩雑である.今回の検討でも PNI を pn0~3 に分類して解析を行ったが, pn0:266 例(64.6%),pn1:116 例(28.2%),pn2:21 例(5.1%),pn3:9 例(2.2%)と pn2,pn3 症例は 特に不良な予後を示したが頻度は 7.3%と低率であり,臨床的に予後に関わる因子として pn1,2,3 を PNI
陽性と定義しその頻度は 35.4%となった.膵癌における PNI について,剣持27)の神経特異抗原および神経
接着分子(neural cell adhesion molecule;NCAM)を用いた検討では,特異抗原による PNI を検出してい る.本検討では S100 染色を 10 例検証し,腫瘍細胞に占居された神経の検索を行った.PNI の判定は HE 染色で行い,通常の病理組織学的診断法で確認することが望ましい.
PNIの頻度は大腸癌では 4.8%~25.9%,直腸癌では 9.9%~34.5%と報告され,本検討でも PNI は直腸癌
の 35.4%であった.また,上部直腸癌の 43.7%,下部直腸癌の 24.7%にみられ,自律神経分布との関連が示 唆された(P<0.001 odd’s ratio 2.60).局所再発では,PNI を伴うものは 1.5~2 倍と報告され,本検討でも 局所再発は高率であった(odd’s ratio 2.25,P=0.008).T 因子では T1 で 5.0%,T2 で 15.4%,T3 で 38.5%, T4で 50%に PNI を認め,T 因子との関連が示された28),PNI は深部に癌が達しやすく転移,局所再発の因 子であることが推測される.本邦では下部直腸での側方リンパ節周囲の制御を推奨しているが,PNI を考 慮すると妥当な考え方である.神経鞘に癌が浸潤すると抵抗が小さい神経鞘の膠原繊維と基底膜の間隙を 進展し29),傍神経間隙を通じて周辺臓器に転移する機序が報告されている30). PNIは頭頸部腫瘍や膵癌,前立腺癌の予後に関連する癌進展経路として知られ,頭頸部腫瘍では生存期 間が短く局所再発が高くなると報告されている31)32).大腸癌では 1943 年に Seefeld ら19)によって初めて報 告され,本邦では 1990 年半ばに直腸癌に関する神経温存手術の feasibility を検討し,前述の剣持27)は壁外 神経叢や Auerbach’s plexus への癌侵襲を報告している.一方,欧米では 2005 年に直腸・結腸がそれぞれ検
討され,PNI は予後因子として臨床的に意義があると報告し,特に Kim ら33)は circumferential radical margin
て示されたが,Stage IV や術後 10 年経過例を含めた検討であり,背景因子が異なることを前提に解釈する 必要がある.
術前放射線化学療法を行った直腸癌でも Guillem ら34)や Kim ら33)は PNI を局所再発および予後不良因子
として報告している.本研究中では 11 例の術前放射線療法(30 Gy~50 Gy)と 7 例の術後放射線療法(50 Gy)の照射が含まれていた.前者では PNI が 4 例(36.4%)陽性で生存率は 36.4%であり,後者では PNI 陽性例が 4 例(57.1%)みられ生存率は 14.3%と低率であった.直腸癌の局所制御には病変の周囲組織を含 めて切除することが重要で,直腸固有筋膜を損傷せず剥離層を揃えた total mesorectal excision(TME)が不
可欠となる35)36).本検討で R1 手術 30 例のうち 17 例が生存し,13 例が再発死亡していた.生存例では PNI 陽性が 3 例(17.6%)であったのに対し,死亡例では 8 例(61.5%)が PNI 陽性であった.PNI 陽性では直 腸周囲の層を考慮し,神経周囲ネットワーク内の癌細胞散布を最小限にとどめる手技が要求される.CRM を 1 mm 確保するのが微妙な T3,T4 症例への NCCN や,AJCC で示される進行直腸癌への術前放射線化 学療法は,術中散布を回避させ局所再発を制御する有効な方法と解釈できる37). 一方,N 因子に対する PNI 陽性率は N0 で 17.9%,N1,2 で 45.1%,N3 で 64.0%,N4 で 80.0%とリンパ 節転移が高度なほど陽性となり,リンパ節転移例の 77.1%が PNI 陽性であった.本検討では下部直腸癌の N3の 18 例は全例が側方リンパ節転移陽性で,癌細胞は骨盤内の神経網やリンパ流を介して浸潤すること が推測された38).以上のことから,下部直腸癌の PNI 陽性例に対する根治的手術では側方郭清が必要とな る.欧米では下部直腸癌への側方郭清は予後に寄与しないと捉えられ,放射線化学療法による側方リンパ 節治療を推奨している39)が,癌局所治療を評価するために TME や郭清リンパ節個数と同様に,下部直腸 癌では側方リンパ節に対しての診断および治療内容(術前化学放射線療法や側方リンパ節郭清)を明記す べきである.
今回,腫瘍先進部の病理組織学的検査所見として PNI と Budding(P<0.001 odd’s ratio 1.51),PNI と低分 化癌胞巣(P<0.001 odd’s ratio 2.04)での相関が示された.また,PNI は病理組織学的因子ではリンパ管侵 襲と相関を示し(P<0.001,odd’s ratio 3.75),PNI をリンパ管侵襲が修飾された形態と解釈することもでき る.前述の頭頸部癌や膵癌および前立腺癌では PNI は予後因子として既に扱われており,自律神経が豊富 に分布する直腸癌でも因子として加えることは妥当である.直腸は膀胱に隣接した自律神経の豊富な臓器 であり,神経周囲のリンパ管や固有のネットワークを有し,PNI を来すとネットワークに沿って転移して いる可能性が示唆されている.また,PNI のみられる腫瘍は neurophilic factor を介して増殖,進展を加速さ せることが証明され,神経周囲に進展している腫瘍は,TME を行っても CRM が陽性となる要因を有し, 局所再発のリスクが高い.この 2 点は癌局所コントロールに極めて重要なファクターで,手術精度に直腸 癌治療成績が左右される所以と考えられる.本研究では中等度ないし高度リンパ管侵襲と脈管侵襲の頻度 は 44.2%および 48.1%で,それぞれ単変量解析では予後に関連したが,T および N 因子を含む予後因子の 多変量解析では有意差を認めなかった.他方,PNI は 35.4%とリンパ管侵襲や脈管侵襲に比較すると低率 であったが,多変量解析でも予後不良の強い因子として有意差がみられた.それらの結果から直腸癌では PNIは程度にかかわらず TNM 分類の T 因子,N 因子を補填する因子として有用であり,NCCN ガイドラ インの如くリンパ管侵襲および脈管侵襲と同様に直腸癌の病理組織学的診断に明記すべきであると結論づ けることができる. 最後に,NCCN ガイドラインは TME や摘出したリンパ節数を手術の精度を判定する治療因子としてガ イドラインに組み入れている.また,PNI に関しては深達度,リンパ節転移を補填する因子の一つとして 明記され,CRM や非連続性節外転移など新たな病理組織学的因子が加えられ予後を反映する分類が行われ ている.本邦でも直腸癌のガイドラインには側方リンパ節に対する術前評価や治療法を明記し,加えて PNI を表記することで,治療指針ことに補助化学療法選択がより明確となることが期待される. 本研究に関しては,貴重な時間を割いてご協力頂いた仙台医療センター病理診断科鈴木博義先生に心より謝意を表し ます.
利益相反:なし
文献
1) Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, editors. AJCC cancer staging manual, 7th ed. New York: Springer; 2010.
2) National Comprehensive Cancer Network. NCCN Guidelines Rectal Cancer version2. 2012. 3) Batsakis JG. Nerves and neurotropic carcinomas. Ann Otol Rhinol Laryngol. 1985;94(4 Pt 1):426–7.
4) Liebig C, Ayala G, Wilks JA, Berger DH, Albo D. Perineural invasion in cancer: a review of the literature. Cancer. 2009;115(15):3379–91.
5) Hase K, Shatney C, Johnson D, Trollope M, Vierra M. Prognostic value of tumor “budding” in patients with colorectal cancer. Dis Colon Rectum. 1993;36(7):627–35.
6) Ueno H, Murphy J, Jass JR, Mochizuki H, Talbot IC. Tumor ‘budding’ as an index to estimate the potential of aggressiveness in rectal cancer. Histopathology. 2002;40(2):127–32.
7) 大腸癌研究会編.大腸癌治療ガイドライン 2010 年版.東京:金原出版;2010. p. 13–5.
8) Giantonio BJ, Catalano PJ, Meropol NJ, O’Dwyer PJ, Mitchell EP, Alberts SR, et al. Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal cancer: results from the Eastern Cooperative Oncology Group Study. J Clin Oncol. 2007;25(12):1539–44.
9) Fuchs CS, Marshall J, Mitchell E, Wierzbicki R, Ganju V, Jeffery M, et al. Randomized, controlled trial of irinotecan plus infusional, bolus, or oral fluoropyrimidines in first-line treatment of metastatic colorectal cancer: results from the BICC-C Study. J Clin Oncol. 2007;25(30):4779–86.
10) Quah HM, Chou JF, Gonen M, Shia J, Schrag D, Landmann RG, et al. Identification of patients with high-risk stage II colon cancer for adjuvant therapy. Dis Colon Rectum. 2008;51(5):503–7.
11) André T, Boni C, Navarro M, Tabernero J, Hickish T, Topham C, et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colom cancer in the MOSAIC trial. J Clin Oncol. 2009;27(19):3109–16.
12) Sugihara K, Kobayashi H, Kato T, Mori T, Mochizuki H, Kameoka S, et al. Indication and benefit of pelvic sidewall dissection for rectal cancer. Dis Colon Rectum. 2006;49(11):1663–72.
13) Ueno H, Mochizuki H, Hashiguchi Y, Hase K. Prognostic determinants of patients with lateral nodal involvement by rectal cancer. Ann Surg. 2001;234(2):190–7.
14) Kapiteijn E, Marijnen CAM, Nagtegaal ID, Putter H, Steup WH, Wiggers T, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med. 2001;345(9):638–46.
15) Jass JR, Love SB, Northover JMA. A new prognostic classification of rectal cancer. Lancet. 1987;1(8545):1303–6.
16) Jass JR, Ajioka Y, Allen JP, Chan YF, Cohen RJ, Nixon JM, et al. Assessment of invasive growth pattern and lymphocytic infiltration in colorectal cancer. Histopathology. 1996;28(6):543–8.
17) Ueno H, Price AB, Wilkinson KH, Jass JR, Mochizuki H, Talbot IC. A new prognostic staging system for rectal cancer. Ann Surg. 2004;240(5):832–9.
18) Cruveilhier J. Maladies Des Nerfs. Anatomie Pathologique Du Corps Humain, 2nd edition. Paris: J.B. Bailliere; 1835. p. 3. 19) Seefeld PH, Bargen JA. The spread of carcinoma of the rectum: invasion of lymphatics, veins and nerves. Ann Surg.
1943;118(1):76–90.
20) Krasna MJ, Flancbaum L, Cody RP, Shneibaum S, Ben Ari G. Vascular and neural invasion in colorectal carcinoma. Incidence and prognostic significance. Cancer. 1988;61(5):1018–23.
21) Ozaki H, Hiraoka T, Mizumoto R, Matsuno S, Matsumoto Y, Nakayama T, et al. The prognostic significance of lymph node metastasis and intrapancreatic perineural invasion in pancreatic cancer after curative resection. Surg Today. 1999;29(1):16–22. 22) Ayala GE, Dai H, Ittmann M, Li R, Powell M, Frolov A, et al. Growth and survival mechanisms associated with perineural
invasion in prostate cancer. Cancer Res. 2004;64(17):6082–90.
23) Peters A, Palay SL, Webster H. Connective tissue sheaths of peripheral nerves. The fine structure of the nervous systems: Neurons and their supporting cells, 3rd edition. New York: Oxford University Press; 1991. p. 494.
24) Cawthorn SJ, Parums DV, Gibbs NM, A’Hern RP, Caffarey SM, Broughton CI, et al. Extent of mesorectal spread and involvement of lateral resection margin as prognostic factors after surgery for rectal cancer. Lancet. 1990;335(8697):1055–9. 25) 白水 和雄,磯本 浩晴,掛川 暉夫.直腸癌の神経周囲浸襲に関する臨床病理学的研究 特に予後および自律神経温 存術との関連性.日本外科学会雑誌.1991;92(4):411–8. 26) 上野 秀樹,望月 英隆,長谷 和生,横山 幸生,吉村 一克,山本 哲久,ほか.直腸癌における神経侵襲の予後規定 因子としての意義に関する検討.日本消化器外科学会雑誌.1994;27(9):2126–34. 27) 剣持 雅一.膵癌の神経浸潤と神経特異抗原および神経接着分子(NCAM)との関連.日本消化器外科学会雑誌. 1990;23(11):2580–5.
28) Fujita S, Nakanishi Y, Taniguchi H, Yamamoto S, Akasu T, Moriya Y, et al. Cancer invasion to Auerbach’s plexus is an important prognostic factor in patients with pT3-pT4 colorectal cancer. Dis Colon Rectum. 2007;50(11):1860–6.
29) Ueno H, Hase K, Mochizuki H. Criteria for extramural perineural invasion as a prognostic factor in rectal cancer. Br J Surg. 2001;88(7):994–1000.
30) Ketterer K, Rao S, Friess H, Weiss J, Buchler MW, Korc M. Reverse transcription-PCR analysis of laser-captured cells points to potential paracrine and autocrine actions of neurotrophins in pancreatic cancer. Clin Cancer Res. 2003;9(14):5127–36. 31) Ayala GE, Wheeler TM, Shine HD, Schmelz M, Frolov A, Chakraborty S, et al. In vitro dorsal root ganglia and human
prostate cell line interaction: redefining perineural invasion in prostate cancer. Prostate. 2001;49(3):213–23.
32) Ballantyne AJ, McCarten AB, Ibanez ML. The extension of cancer of the head and neck through peripheral nerves. Am J Surg. 1963;106:651–67.
33) Kim NK, Kim YW, Min BS, Lee KY, Sohn SK, Cho CH. Factors associated with local recurrence after neoadjuvant chemoradiation with total mesorectal excision for rectal cancer. World J Surg. 2009;33(8):1741–9.
34) Guillem JG, Chessin DB, Cohen AM, Shia J, Mazumdar M, Enker W, et al. Long-term oncologic outcome following preoperative combined modality therapy and total mesorectal excision of locally advanced rectal cancer. Ann Surg. 2005;241(5):829–36.
35) Enker WE, Pilipshen SJ, Heilweil ML, Stearns MW Jr, Janov AJ, Hertz RE, et al. En bloc pelvic lymphadenectomy and sphincter preservation in the surgical management of rectal cancer. Ann Surg. 1986;203(4):426–33.
36) Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986;1(8496):1479–82. 37) Quirke P, Durdey P, Dixon MF, Williams NS. Local recurrence of rectal adenocarcinoma due to inadequate surgical resection.
Histopathological study of lateral tumor spread and surgical excision. Lancet. 1986;2(8514):996–9.
38) Feil W, Wunderlich M, Kovats E, Neuhold N, Schemper M, Wenzl E, et al. Rectal cancer: factors influencing the development of local recurrence after radical anterior resection. Int J Colorectal Dis. 1988;3(4):195–200.
39) Burdy G, Panis Y, Alves A, Nemeth J, Lavergne-Slove A, Valleur P. Identifying patients with T3–T4 node-negative colon cancer at high risk of recurrence. Dis Colon Rectum. 2001;44(11):1682–8.
Evaluation of Perineural Invasion in Rectal Cancer as a Prognostic Factor
Kazutsugu Iwamoto
1), Toshihiro Saito
2), Shin Teshima
2), Kazunori Takeda
2),
Hiroyoshi Suzuki
2), Toshihiro Noake
1)and Yasumi Araki
1)1) Kurume Coloproctology Center
2) Sendai Medical Center
Purpose: The aim of this study was to evaluate perineural invasion (PNI) of rectal cancer as a prognostic factor. Method: Subjects were 412 patients undergoing intestinal resection for rectal cancer, and patients who had undergone surgery between 1996 and 2005 were investigated retrospectively, of whom patients who received surgery between 2006 and 2010 were evaluated prospectively. Results: PNI was found in 144 patients (35.4%), of which 43.7% was in upper rectal cancerand 24.7% in lower. Multivariate logistic regression analysis showed that PNI was significantly associated with upper rectal cancer (P<0.001), lymphatic invasion (P<0.001), vascular invasion (P=0.003), and poorly differentiated component at tumor front (P=0.046). The PNI-positive group had a significantly worse survival curve. 3- and 5-year overall survival rates of PNI-positive cases were 56.2% and 37.3%, respectively. The survival rates of the PNI-negative group were 79.6% and 72.6% (P<0.001). The PNI-positive group in patients without lymphatic metastasis (stage II) also had poor prognosis, and the 5-year overall survival rate was 44.0%. In contrast, the survival rate for the PNI-negative group was 82.7% (P=0.008). The overall survival rate was significantly associated with lymph node metastasis (P<0.001), T3/T4 (P<0.001), and PNI (P=0.001), however, not associated with lymphatic invasion and vascular invasion. Local recurrence was also significantly related to T3/T4 (P<0.001, odd’s ratio 3.03), and PNI (P=0.003, odd’s ratio 2.60). Conclusion: In this study, PNI in patients with rectal cancer was significantly associated with prognosis and local recurrence. It was suggested that PNI was indispensable and valuable as a prognostic factor more than lymphatic invasion and vascular invasion.
Key Words: rectal cancer, perineural invasion, risk factor, survival rate
[Jpn J Gastroenterol Surg. 2013;46(9):635-646] Reprint requests: Kazutsugu Iwamoto Kurume Coloproctology Center
2-2-18, Shin-Aikawa, Kurume, 839-0865 JAPAN Accepted: April 24, 2013
© 2013 The Japanese Society of Gastroenterological Surgery