は じ め に
脳動脈瘤が血栓化をきたすと急速に増大して mass
ef-fect を呈したり,破裂の誘因となるなど急激な変化を認め
ることがある.大型および巨大動脈瘤の 40-50%に血栓化
を伴い
5)15),動脈瘤が血栓化をきたすと破裂のリスクが上
昇し,さらに血栓の飛散による脳梗塞を発症することもあ
る
5)21).中大脳動脈瘤に対する治療は一般的には直達手術
が主流であるが,血栓化を伴った大型動脈瘤では広頚で
あったり,穿通枝や術中の中大脳動脈血栓化などの問題も
香川大学医学部 脳神経外科(受稿日 2016. 11. 4)(脱稿日 2017. 4. 10)〔連絡先:〒 761-0793 香川県木田郡三木町池戸 1750-1 香川大学医 学部 脳神経外科 岡内正信〕[Address correspondence: Masanobu OKAUCHI, M.D., Ph.D., Department of Neurological Surgery, Kagawa University Faculty of Medicine, 1750-1 Ikenobe, Miki-cho, Kita-gun, Kagawa 761-0701, Japan]脳卒中の外科 45: 403 〜 408,2017
症 例
あり
6),直達手術のリスクは決して低くなく治療方針の決
定には慎重な検討を要する.近年では,血管内手術の有効
性も報告されている
3)14).今回,われわれは症候性の中大
脳動脈部分血栓化動脈瘤に対して外科治療を行った 2 症例
を経験したので,文献的考察を加えて報告する.
症
例
〈症例 1〉 20 歳,男性.
突然の頭痛,嘔吐を自覚し,近医脳神経外科を受診し
た.頭部 CT および MRI にて右中大脳動脈瘤を認めた
中大脳動脈部分血栓化動脈瘤の 2 症例
岡内 正信,新堂 敦,川西 正彦,田宮 隆
Partially Thrombosed Aneurysm in the Middle Cerebral Artery:
Two Case Reports
Masanobu O
KAUCHI, M.D., Ph.D., Atsushi S
HINDO, M.D., Ph.D.,
Masahiko K
AWANISHI, M.D., Ph.D., and Takashi T
AMIYA, M.D., Ph.D.
Department of Neurological Surgery, Kagawa University Faculty of Medicine, Kagawa, Japan
Summary: Thrombosis of cerebral aneurysms increases the risk of rupture and may even lead to ce-rebral infarction due to the dispersion of thrombus. We describe two case reports for patients who underwent surgical treatment for a symptomatic partially thrombosed aneurysm of the middle cere-bral artery (MCA).
Case 1 was a 20-year-old man who presented with a headache. Detailed examination revealed a par-tially thrombosed large cerebral aneurysm along the right MCA, which was enlarged owing to ad-vanced thrombosis. The patient experienced subarachnoid hemorrhage while awaiting planned sur-gery and underwent emergency neck clipping of the aneurysm.
Case 2 was a 63-year-old woman who developed cerebral infarction following a right MCA aneurysm growth with thrombosis and underwent emergency coil embolization. She presented with a recurrent aneurysm 3 months later, and underwent a second coil embolization. Both cases showed acute trans-formation secondary to thrombosis. Urgent treatment is warranted when symptoms related to throm-bosis are observed. The treatment strategy should be designed carefully to suit individual cases based on varying anatomy/geometrical patterns of aneurysms and varying progression of thrombosis.
Key words:
・ thrombosed aneurysm ・ middle cerebral artery ・ subarachnoid hemorrhage ・ cerebral infarction Surg Cereb Stroke (Jpn) 45: 403-408, 2017
が,画像上および腰椎穿刺による髄液検査にても,くも膜
下出血は否定された(Fig. 1A-C).その 5 日後に再度頭痛
発作があったため,当院を受診した.頭部 CT および
MRI ではこのときもくも膜下出血は認めなかったが,動
脈瘤の血栓化に伴って軽度増大し,周囲に脳浮腫が出現し
ていた(Fig. 1D-F).緊急入院とし,引き続き精査を行っ
た.頭部 MRI における動脈瘤の大きさは 20×16 mm で,
頚部には血栓化が及んでいない所見であった.脳血管撮影
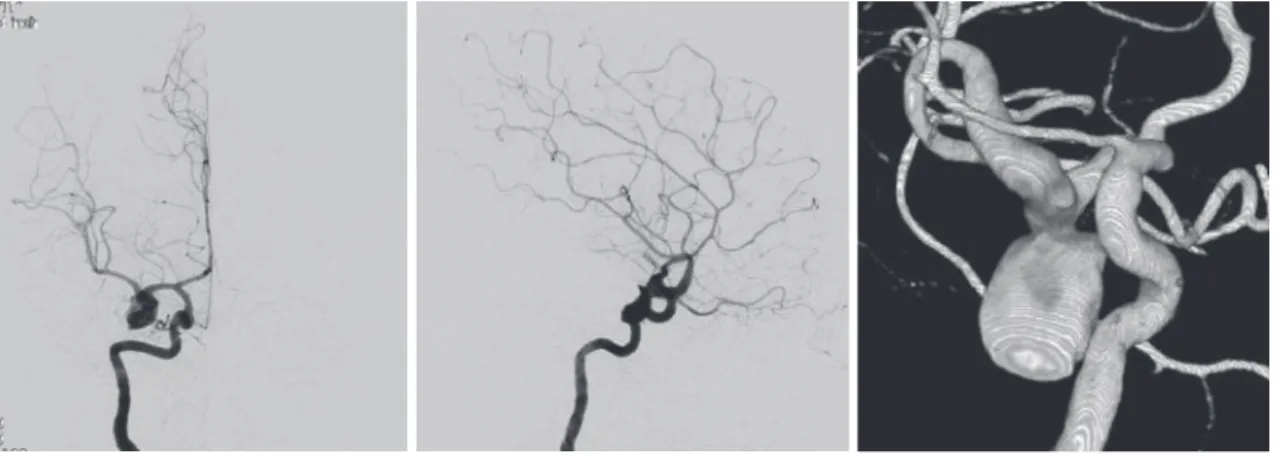
では,動脈瘤は右中大脳動脈 M1 に下向きに存在していた
(Fig. 2).準緊急でクリッピング術の予定としていたが,
手術予定日直前(2 回目の頭痛発作から 5 日後)にくも膜下
出血を発症した.Hunt & Kosnik grade V で頭部 CT にて
脳室穿破を伴うくも膜下出血を認め(Fig. 3A),両側脳室
ドレナージに続いてネッククリッピング術および右内・外
減圧術を施行した(Fig. 3B, C).症候性の脳血管攣縮は認
めず,day 14 に気管切開術,day 34 に頭蓋形成術を施行
した.4 カ月後に modified Rankin Scale(mRS)5 で転院さ
れた(Fig. 3D).
〈症例 2〉 63 歳,女性.
ふらつきの精査で施行した頭部 MRI・MRA にて,右中
大脳動脈瘤が偶然発見された.右中大脳動脈 M1 に上向き
に突出する長径 2 mm の不整形動脈瘤で(Fig. 4A),まず
は保存的に経過観察の方針とした.3 カ月後の MRI では
変化はなかったが,その半年後の MRI にて動脈瘤の血栓
化に伴う増大(15 mm)および脳浮腫の出現を認めた(Fig.
4B, C
).早急に入院精査を行った後,治療方針検討中に突
然の左上下肢麻痺が出現し,緊急頭部 MRI にて右内包後
脚に急性期脳梗塞を認めた(Fig. 4D).脳血管撮影では,
動脈瘤頚部左背側より基底核部へ向かう穿通枝が分岐して
Fig. 1 Computed tomography (CT) image (A), magnetic resonance imaging-T2-weighted
image (MRI-T2WI) (B), and fluid attenuation inversion recovery (FLAIR) image (C) performed at the presentation of first headache attack showing a right middle ce-rebral artery aneurysm. CT (D), MRI-T2WI (E) and FLAIR (F) performed at the pre-sentation of second headache attack showing progression of intra-aneurysmal thrombosis and perifocal brain edema.
A B C D E F
おり(Fig. 4E),動脈瘤内血栓の飛散による穿通枝梗塞と
診断し,同日に脳動脈瘤コイル塞栓術を施行した.動脈瘤
の頚部より中大脳動脈の分枝および穿通枝が分岐してお
り,これらを温存するようにシンプルテクニックでコイル
塞栓術を行った(Fig. 4F, G).術後の経過は良好で,左上
下肢麻痺も改善し,mRS 0 で退院した.しかし,3 カ月後
の MRI にて coil compaction に伴う動脈瘤の再発を認め
(Fig. 5A),追加のコイル塞栓術を初回治療と同様の方法
で施行した(Fig. 5B, C).3 カ月後の MRI では動脈瘤の再
発は認めず,脳浮腫も著明に減弱していた(Fig. 5D, E).
その後,約 1 年経過観察しているが,動脈瘤の再発はきた
していない.
考 察
脳動脈瘤の血栓化は全脳動脈瘤の 9-13%に認め
9)19),大
きなものほど血栓化の頻度は高く,20-25 mm の大型動脈
瘤では 48%,25 mm 以上の巨大動脈瘤では 76%に血栓化
を認める
18).血栓化脳動脈瘤の発症形式としては,33-Fig. 2 Right internal carotid artery angiogram (A: anterior-posterior view, B: lateral view, C:
three-dimensional view) showing a large aneurysm located in the M1 segment.
A B C
A B C D
Fig. 3 Computed tomography (CT) image (A) showing subarachnoid
hemor-rhage with ventricular rupture. Postoperative CT (B) and three-dimen-sional computed tomography (3D-CT) angiogram (C) demonstrating clipping of the neck of the aneurysm. Magnetic resonance imag-ing-T2-weighted image (MRI-T2WI) (D) performed 4 months after op-eration showing extensive brain damage.
44%がくも膜下出血,5-8%が脳虚血症状で発症すると報
告されている
7)8)21).脳動脈瘤の約 20%が中大脳動脈に発
生するが
13),Lawton ら
12)が報告した 68 例の血栓化脳動脈
瘤のうち,中大脳動脈瘤は 11 例(16%)であった.血栓化
脳動脈瘤は血栓の範囲や正常血管との関係などから分類さ
れるが,本 2 症例はいずれも頚部を有する囊状動脈瘤で,
血栓は動脈瘤頚部には及んでいない部分血栓化動脈瘤であ
り,中大脳動脈瘤の中では最も多いタイプのものであ
る
6)12).
症例 1 は,出血発症前に 2 度くも膜下出血を疑う突発性
の頭痛があったが,CT,MRI および髄液検査にてくも膜
下出血は認めなかった.脳動脈瘤の破裂以外で急激な頭痛
を示す原因として,瘤内血栓化や壁内血腫に伴う急激な動
脈瘤の増大によるものが報告されている
22)23).本症例で
は,2 度目の頭痛発作時の MRI にて 1 回目の発作時と比
べて瘤内の血栓化に伴う動脈瘤の増大および脳浮腫の出現
を認めており,急激な血栓化の進行が頭痛の原因であった
と考えられた.手術手技に関しては,動脈瘤の頚部には血
栓化が及んでいなかったことから,まずはネッククリッピ
ングを目指し,不可能であった場合に備えて,浅側頭動
脈-中大脳動脈吻合術ができるように準備をして手術に臨
む方針であった.文献的にも,このタイプの部分血栓化動
脈瘤に対してはネッククリッピングで治療されることがほ
とんどで,術中の血栓化合併症も少なかったと報告されて
いる
6)12).本症例では,不幸にも手術待機中にくも膜下出
血を発症してしまい,緊急手術を行った.術前検査の通り
動脈瘤頚部には血栓を認めず,ネッククリッピングが可能
であった.
症例 2 は,頭痛などの症状をきたさずに血栓化を伴う増
大を認めた中大脳動脈瘤で,瘤内血栓の飛散によると思わ
れる脳梗塞を発症した症例である.脳虚血症状で発症した
未破裂脳動脈瘤の大きさは平均 12.5 mm と報告されてお
り
16),本症例は 15 mm であった.本症例も症例 1 と同様
に動脈瘤頚部には血栓化が及んでおらず,根治的にはネッ
ククリッピング術が最善と考えられたが,動脈瘤は M1 に
位置する上向きであり直達手術による穿通枝の損傷が懸念
Fig. 4 Magnetic resonance angiography (MRA) (A) showing a small aneurysm located along the
right middle cerebral artery. Follow-up MRA (B) showing enlargement of the aneurysm with development of thrombosis, and magnetic resonance-fluid attenuation inversion re-covery (MRI-FLAIR) image (C) showing brain edema around the aneurysm. Fresh cerebral infarction was detected in the posterior internal capsule on MRI-diffusion-weighted imag-ing (DWI) (D). Three-dimensional digital subtraction angiography (3D-DSA) (E) showimag-ing a perforator that originated at the neck of the aneurysm (arrowheads). Coil embolization of the aneurysm was performed (F: preoperative angiogram, G: postoperative angiogram).
A B C D E F G
された.脳梗塞による麻痺症状は軽微であったため,穿通
枝閉塞による合併症の出現はよりためらわれる状況であっ
た.血管撮影上,マイクロカテーテルの誘導は容易に可能
と思われ,まずはコイル塞栓術にて治療を行う方針とし
た.動脈瘤頚部より穿通枝および中大脳動脈分枝が分岐し
ており,これらを温存するようにシンプルテクニックでコ
イル塞栓術を行った.再発した場合に追加治療が困難とな
ることを考慮して,ステントは使用しなかった.中大脳動
脈瘤はしばしば広頚であったり,中大脳動脈分枝が頚部に
巻き込まれていたりするなどの解剖学的特徴や手術アプ
ローチの容易さから,直達手術で治療されることが多
い
1)17).しかし,中大脳動脈瘤に対する血管内手術の有用
性の報告も散見され
2)20),Mortimer ら
14)はコイル塞栓術で
治療した 300 例の中大脳動脈瘤〔うち 244 例(80.7%)が破
裂動脈瘤〕において完全閉塞率は 91.4%,morbidity and
mortality は 7.8%,再治療例は 4.3%,79.4%が予後良好で
あったと報告しており,直達手術と遜色ない結果であっ
た.部分血栓化動脈瘤に対するコイル塞栓術で問題となる
のは再発率の高さで,70-80%と報告されている
4)11).再発
率は血栓化の程度と関連があるとされており,Cho ら
3)は
血栓化の範囲が広い動脈瘤 10 例のコイル塞栓術において
再発率は 30%であったと報告している.頚部を有する囊
状動脈瘤で血栓化の範囲が広いものはコイル塞栓術も選択
肢となり得ると考察されているが,本症例もそれに該当す
ると考えられた.しかし,本症例では,動脈瘤頚部より分
岐する穿通枝および中大脳動脈分枝を温存するために,あ
えて頚部を残したこともあり,再発をきたして再治療を要
した.麻痺などの合併症を呈することなく治療を行えた
が,動脈瘤が再発したことを考慮すると,やはり開頭術を
第一選択とすべきであったと考えられた.今後,再発を繰
り返した場合に,どのように治療するかが課題である.血
管内手術の新しいデバイスとして,Woven Endovascular
Bridge(WEB)が部分血栓化動脈瘤にも有効であったと報
告されており
10),新たな治療選択肢として期待される.
結 語
中大脳動脈血栓化動脈瘤の破裂瘤に対し,ネッククリッ
ピング術を施行した 1 例と,脳梗塞にて発症した未破裂瘤
に対し,コイル塞栓術を施行した 1 例を報告した.いずれ
も血栓化を契機に急激な変化をきたしており,血栓化によ
Fig. 5 Magnetic resonance angiography (MRA) (A) obtained 3 months after the first operation demonstrates
recanalization of the aneurysm. A second coil embolization was performed (B: preoperative angiogram,
C: postoperative angiogram). MRA (D) and magnetic resonance-fluid attenuation inversion recovery
(MRI-FLAIR) image (E) performed 3 months after the second operation showing no recurrence of aneu-rysm and significant attenuation of brain edema.
A B C D E
る症状を認めた場合は,早急な治療が必要である.動脈瘤
の形状や血栓化の進展状況により治療方針は異なるた
め,個々の症例に応じて慎重に検討する必要がある.
本論文の要旨は,第 45 回日本脳卒中の外科学会(2016
年 4 月,札幌)で発表した.著者全員は日本脳神経外科学
会への COI 自己申告を完了しています.本論文の発表に
関して開示すべき COI はありません.
文
献
1) Ausman JI: The future of neurovascular surgery. Part I: In-tracranial aneurysms. Surg Neurol 48: 98-100, 1997
2) Bracard S, Abdel-Kerim A, Thuillier L, et al: Endovascular coil occlusion of 152 middle cerebral artery aneurysms: initial and midterm angiographic and clinical results. J Neurosurg 112: 703-708, 2010
3) Cho YD, Park JC, Kwon BJ, et al: Endovascular treatment of largely thrombosed saccular aneurysms: follow-up results in ten patients. Neuroradiology 52: 751-758, 2010
4) Choi IS, David C: Giant intracranial aneurysms: development, clinical presentation and treatment. Eur J Radiol 46: 178-194, 2003
5) Drake CG: Giant intracranial aneurysms: experience with surgical treatment in 174 patients. Clin Neurosurg 26: 12-95, 1979
6) Eliava S, Pilipenko Y, Shekhtman O, et al: Reversal of intraop-erative arterial thrombosis with a fibrinolytic agent when treating large and giant partially thrombosed aneurysms of the middle cerebral artery. J Neurosurg 124: 1114-1122, 2016 7) 藤田勝三,山下晴央,増村道雄,ほか:巨大脳動脈瘤症例の
Natural history ─特に脳血管写,CT 所見より.No Shinkei Geka 16: 225-231, 1988
8) Hosobuchi Y: Direct surgical treatment of giant intracranial aneurysms. J Neurosurg 51: 743-756, 1979
9) Housepian EM, Pool JL: A systemic analysis of intracranial aneurysms from the autopsy file of the Presbyterian Hospi-tal. J Neuropathol Exp Neurol 17: 409-423, 1958
10) Kabbasch C, Mpotsaris A, Reiner M, et al: WEB as part of a multimodality treatment in complex, large, and partially thrombosed intracranial aneurysms: a single-center observa-tional study of technical success, safety, and recurrence. J
Neurointerv Surg 22: 2016, doi: 10.1136/neurintsurg-2015- 012126
11) Kim SJ, Choi IS: Midterm outcome of partially thrombosed intracranial aneurysms treated with Guglielmi detachable coils. Interv Neuroradiol 6: 13-25, 2000
12) Lawton MT, Quiñones-Hinojosa A, Chang EF, et al: Throm-botic intracranial aneurysms: classification scheme and man-agement strategies in 68 patients. Neurosurgery 56: 441-454, 2005
13) Locksley HB, Sahs AL, Knowler L: Report on the cooperative study of intracranial aneurysms and subarachnoid hemor-rhage. Section II. General survey of cases in the central regidtry and characteristics of the sample population. J
Neu-rosurg 24: 922-932, 1966
14) Mortimer AM, Bradley MD, Mews P, et al: Endovascular treatment of 300 consective middle cerebral artery aneu-rysms: clinical and radiological outcomes. AJNR Am J
Neuro-radiol 35: 706-714, 2014
15) O’Neill M, Hope T, Thomsom G: Giant intracranial aneurysms: diagnosis with special reference to computerized tomogra-phy. Clin Radiol 31: 27-39, 1980
16) Qureshi AI, Mohammad Y, Yahia A, et al: Ischemic events associated with unruptured intracranial aneurysms: multi-center clinical study and review of the literature.
Neurosur-gery 46: 282-289, 2000
17) Regli L, Uske A, de Tribolet N: Endovascular coil placement compared with surgical clipping for the treatment of unrup-tured middle cerebral artery aneurysms: a consective series.
J Neurosurg 90: 1025-1030, 1999
18) Rosta L, Battaglia R, Pasqualin A, et al: Italian cooperative study on giant intracranial aneurysm: 2. Radiological data.
Acta Neurochir Suppl(Wien) 42: 53-59, 1988
19) Spallone A, Cantore G: The role of extracranial carotid abnor-malities in the genesis of the cerebral aneurysms. J
Neuro-surg 55: 693-700, 1981
20) Suzuki S, Tateshima S, Jahan R, et al: Endovascular treatment of middle cerebral artery aneurysms with detachable coils: angiographic and clinical outcomes in 115 consective pa-tients. Neurosurgery 64: 876-888, 2009
21) Whittle IR, Dorsch NW, Besser M: Spontaneous thrombosis in giant intracranial aneurysms. J Neurol Neurosurg Psychiatry 45: 1040-1047, 1982 22) 矢野昭正,三好康之,西本 健,ほか:動脈瘤内血栓化ある いは壁内出血による突然の頭痛によって発症した後大脳動脈 large aneurysm の 1 例.脳卒中の外科 28: 222-225, 2000 23) 安井敏裕,矢倉久嗣,小宮山雅樹:巨大脳動脈瘤において破 裂以外の機序で急激な症状の増悪を来すメカニズム─壁内血 腫ならびに瘤内血栓化.No Shinkei Geka 21: 897-901, 1993