頚部頚動脈狭窄からのartery-to-artery embolismの病態 ―自験頚動脈内膜剝離術からの考察―
全文
図

関連したドキュメント
To induce cerebral hypoperfusion, chronic stenosis was produced by placing a 3 mm long polyethylene cuff around the bilateral carotid arteries of
Yamagishi M, Ozaki Y, Kimura K, Saito S, Yamaguchi T, Daida H, Matsuzaki M: Effect of intensive statin therapy on regression of coronary atherosclerosis in patients with
antihypertensive treatment:a meta-analysis of randomized controlled trials. Statins in stroke prevention and carotid atherosclerosis:systematic review and up-to-date
6) Gasecki AP, Ferguson GG, Eliasziw M, Clagett GP, Fox AJ, Hachinski V, Barnett HJ: Early endarterectomy for severe carotid artery stenosis after a nondisabling stroke: results
Sohda M, Sakai M, Honjyo H, Hara K, Ozawa D, Suzuki S, Tanaka N, Yokobori T, Miyazaki T, Fukuchi M, Higuchi T, Tsushima Y, Kuwano H. L-[3-18F]- α -methyltyrosine accumulation
(先天性巨大血小板性血小板減少症を引き起こす第一zinc finger domain上の新規GFI1B 変異 ) Uchiyama Y, Ogawa Y, Kunishima S, Shiina M, Nakashima M, Yanagisawa K,
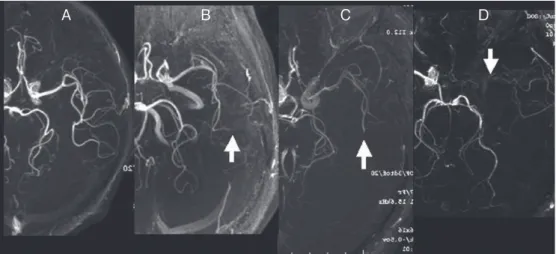
Image B demonstrating that pyoktanin staining has visualized previously unrecognized minute plaque debris captured on the same
Objective: To report a case of symptomatic internal carotid artery stenosis with a persistent proatlantal artery (PPA), which was treated by carotid artery stenting (CAS) with
