mp#asik7
ag34tsth8e
316-327R
(2007ff)
Nwereigasva
The
Effects
of
an
Eight
Week
Fallproof!TM
CIass
Comparing
High
and
Low
Functioning
Participants
*
Peggy
R,
TRUEBLOOD,
PT,
PhD"",
Toni
TYNER,
PT,
MSL,
Nancy
WUBENHORST,
MPT,
Jody
BRADLEY,
MPT,
Ulia
CUMMINGS,
MPT,
Jenneryn
de
MESA,
MPT,
Taylor
LE,
MPT,
Danny
NORRDIN,
MPT,
Natasha
PIPER,
MPT,
Kim
RIGGS,
MPT
and
Kathy
SILVA,
MPT
tntroduction
Adults
everthe
age ef65
representthe
fastest
growing
population
in
the
United
States.
Of
increasing
concernfor
this
segment ofthe
pepulation
is
the
risingincidence
offalls.
More
than
one-third of adults ages65
years
and olderfall
eachyeari).
Falls
pose
a significantprobEem
for
elder adults and resultin
considerablehuman
and economical costs.Among
older adults,falls
arethe
leading
cause ofinjury
deaths
andthe
most common cause of non-fatalinjuries
andhospital
admissionsfor
trauma2)3),
Of
those
whofaLl,
20-30
%
suffer moderateto
severeinjuries
such aship
fractures
orhead
traumas
that reduce mobility andindependence,
andincrease
the
risk of prematuredeath4).
Besides
the
pain,injury,
anddisability
associated wtthfalls,
older adults whohave
fallen
one er moretimes
often experience a height-enedfear
offalling
and aloss
of self-confidencein
their
abil-ity
to
perform
routine activities encounteredin
daily
life2)
Costs
asseciated withfalls
amongthe
eLderly are estimatedto
rangefrom
75-100
billion
dellars
per
yeai}.
In
orderto
minimizethe
negative econemic and socialimpact
that
resultsfrom
falls,
clevelopment
of specific ancl effective bal-ance and mobilityintervention
programs
designed
to
reducethe
number offalls
amollg older adults are a publichealth
pnonty.
Preserving
balance
is
acriticalpart
of maintainingmobil-ity
andfunction.
Clark
et ai.defines
balance
as ''theinte-gration
and organization of sensoryinputs
used to maintain uprightbalance
and volitional and reactivebaEance
controlin
dynarnic
environments"4).The
sensoryinputs
from
three
sensory systems
(visual,
somatosensory, and vestibular)help
'
".ig6fitsrc#Ea)tutuntvagv:tsJ't6sxamaa)
rFallproofll
7'u
f7AOstM
"
h
i)7 t;le=7{・[・[iJ
"le\1itift7pt
(Xva)
Correspondence/
Peggy
R.
Trueblood,
PhD,
PT.
'
Professor,
Physical
Therapy,
CaLifornia
State
University,
Fresno
2345
East
San
Ramon
Ave;
MfS
MH29
Fresno,
CA
93740-8031,
USA
maintam and regain
balance
during
vanous activities3)5'S}.It
is
the
connbination ofinputs
from
allthree
systemsthat
com-prise
balance.
The
redundancy allows oneto
two
systemsto
compensatefor
anether when one systemis
compro-mised4).The
abilityto
maintainbalance
deteriorates
during
the
agingprocess3)9}.
Examples
of age related changesinclude:
an
increased
threshold
for
excitabilityfor
proprioception,
decreased
visuat acuity, orthe
reduction ofthe
hair
celisin
the
vestibuiar system9)iO).According
to
Woollacott
et al.iO),these
alteredinputs
can resultin
a sensory conftict and ulti-mately affectbalance
andput
the
older adult athigh
riskfor
falls,
Identifying
riskfactors,
therefore,
is
important
for
rnaintaining
baLance
in
the
older adult3}9)ii'i6}.Risk
factors
canbe
extrinsie orintrinsic.
Extrinsic
factors
(situational
risks) are environmental
in
nature andinclude:
the
time
ofday,
lighting,
stairs, uneven surfaces,tripping
hazards,
andthe
type
of surfacethat
waslanded
uponi]).IntrTnsic
factors
are `within'the
individuaL
and can rangefrem
decreasecl
muscular strength andjoint
fiexibility
to
medication inter-actien, orimpairment
ofthe
three
sensory systemsi4'i6}.Fortunately,
comprehensively addressingthe
multiple riskfactors
assoeiated withfalls
canpotentially
help
prevent
fatls
from
eccurring3)4)9'i6).Numerous
studieshave
investigated
otherpredisposing
risk
factors
that
appearedto
convey a rTsk offalling
andinclude
factors
such as age,gender,
low
bedy
massindex,
cognitive
impairments,
previous
falis,
demographic
data,
chronicdiseases,
and medicationii'i3) i6'2i),The
risk offalling
increases
linearly
with the number of riskfactors
anddeclines
11%
with adecrease
of one riskfactori2)
i3).Tinetti
et al.ii) suggestedthat
preventative
programs
addressingboth
predisposing
and situational riskfactors
may resultin
the
greatest
injury
reduction.Previous
studies suggest varied resultsfor
interventions
such as exercise
in
a community-basedprogram
or an indi-vldualhome
program
to
improve
balance
and reduce risksJapanese Physical Therapy Association
NII-Electronic Library Service
JapanesePhysical Therapy AssociationThe
Effects
of anEight
Week
FallproqfYTM
CIass
for
falls22'24}.
one
study23) suggeststhat
exercise as antnter-ventTon can significantly
improve
balance
and reducefalls
in
elders, whereasin
another study24), a community-based physical activitylntervention
did
not sTgnificantly reducefall
riskfactors.
One
limitation
ofthese
studiesis
that
aone-dlmensional
measure ofbalance
to
predict
falls
is
unreliabledue
to
underlyingpathologies
that
arepresented
by
the
sub-jecti9).
The
majority oipreceding
studies emphasize strengthening and stretching exercisesto
improve
balance
and coerdination, and neglectedto
addressthe
three
senso-ry systemsfor
balance
(visual,
somatosensory,vestibu-lar)14}22)24'2s).
Recent
studieshave
shownthat
amulti-dimensionalinter-vention
targeting
balance
and mobility may reducefall
riskin
COMmuntty-dwelling elder adults2)]3']6)22)25)29'33).Furthermore,
group-based
programs
with multi-dimensionalinterventions
have
been
shownto
be
effectivein
thereduc-tion
in
falls
andimprovement
in
balance
with the elderlypopulation25).
Province
et al.3i) used a meta-analysis ofthe
Frailty
andInjuries:
Cooperative
Studies
ofIntervention
Techniques
studiesa4) andfound
that treatmentsincluding
exercise withbalance
training
could reducethe
risk offa11s
by
ten
percent
However,
researchis
tacking
regardingthe
integration
ofthe
three
sensory systems whichplay
impor-tant
relesin
maintaining static anddynamic
postural
con-tro12)29)'
The
key
cornponents neededto
improve
an indi-vidual'sbodily
orientation areintegration
ofthree
etements:the
environment,the
goals
ofthe
task,
andthe
abilities ofthe
individua12)9),
Dr.
Debra
Rese
frem
the
Center
for
Successful
Aging
atCalifornia
State
University,
Fullerton
has
recenulydesigned
a community
based
multi-dimensional programfor
persons
at medium tehigh
riskfor
falling:
FallprooftTM,
She
has
multipleyears
of experience working with olcler adults withbalance-related
impairments
andhas
successfully startedthese
comrnunity-basedprograms
in
variousfacilities
throughout
Orange
County,
CA.
The
thgiproqffTM
program
integrates
thethree
balance
systemsby
manipulating thetask
and environment, along with educatingthe
participants
regardingintrinsic
and extrinsicfactors.
The
level
of inten-sity efthe
program
specifically addressesthe
balance-relat-ed
impairments
identified
during
the
initial
screening.Thus,
persons
withboth
high
andlow
physical
function
canpar-ticipate,
Peer
mentors aretrained
to
assistthe
lower
func-tionTng
participants
andthus
ensure safetyin
agreup
class.However,
no studyhas
specifically comparedlower
func-tioning
andhigher
functioning
participants.
Participants
engagein
activitiesthat
aredesigned
by
certifiedbalance
and mobllityinstructors
to
progressively
challengethe
bal-ance systern,
The
ebjective of our research wasto
substantiate asim-Comparing
High
andLow
Functioning
Participants
317
ilar
program
in
the
Fresno,
CA
area andto
answer the
lowing
three
questions/
1)
will oLder adults(over
the
age of50}
at mediumto
high
riskfor
falling
improve
their
balance
after
taking
an eight-weekFZiliprooffTM
class:2}
arethere
any
diiferences
in
outcome measuresbetween
individuals
who are
functioning
at alower
physical
tevel
andthose
tioning
at ahigher
physical
level;
and3)
whatis
the
mal number of sessions, out of a
total
of16
sessions,that
is
requiredto
showimprovement?
To
answerthese
tions,
wehypothesized:
1)
an eight-weekbalance
tion
program
following
the
FaleproofS'i'M
model wou]d
duce
significantimprQvement
in
persons
who are atum
to
high
riskfor
falls:
2)
the
older adults who aretioning
at alewer
physicaHevel
would make comparableimprovements
to
the
older adults who arefunctioning
at ahigher
physical
level:
and3)
individuals
whoparticipated
in
75-100%
ofthe
Fkxliproof,rTM
classes(at
least
12116
sessions)weuld
demonstrate
significantlybetter
resultsthan
those
who
participated
in
56-74%
ofthe
classes(9-11
sessions).
Therefore,
the
purpose
ofthis
study wasto
assessthe
tiveness of
the
eight-weekFallproof!TM
Balance
and
Mobility
classes on comrnunity-dwelling older adults
tioning
atdifferent
physical
activitylevels
through
lheir
formance
on selectedbalance
activities andtests.
Selected
balance
activitiesincluded
an exercise-based rehabilitation
program
withthe
fellewing
components:bone
loading,
gait,
dynamic
posture,
balance,
reaction, and co-ordination
ing
intended
to
improve
balance
and mobility and reduceor
prevent
falls,
The
tests
included
impairment
and mance-basedbalance
assessnnents.By
answeringthe
three
questions
posed,
we canmine
if
the
Fallproof!TM
classis
effectivefor
reducingthe
risk of
falls
in
both
1iigh
andlow
functioning
older adutts.Falls
continuete
be
a slgnificant source of morbidity andmortality among older adults,
despite
the
medicalnity's extensive
preventative
efforts32)35)3S).According
to
the
California
Department
ofHealth
Services,
`unintentional
fall'
was
the
number oneleading
cause ofhospitalized
nonfatalinjuries
in
older adults ages55
and abevein
200135).
Falls
often
lead
to
seriousinjuries
such aship
fractures,
talizatien,
anddeath,
andthe
average cost of atotal
hip
replacement
is
$21,ooo32)35'3B).
Our
goal
is
to
determine
if
acemmunity-based
fall
prevention
class, at a cost ef$75
per
persoll,
can significantlyimprove
an older adult's sense of
balance
and]evel
of cenfidence,if
se, we canhelp
avoidthe
significant sociar and economic ramifications
by
providing
older adults a cost-effective, accessible method
to
address318
-eutifte
Methods
Subjects
The
studypopulation
consisted of older adultsliving
in
the
communTty and retirement centers within theFresno,
CA
region,Recruiting
consisted ofposting
flyers
at seniorcenters,
placing
an adin
the
local
newspaper, solicitingprior
participants
from
the
Gait,
Balanee
andMobility
Center
at
California
State
University,
Fresno
and contactingals
from
thegelleral
communityin
theCentral
Valley
of
California,
Over
a period of one year,203
panicipants
were contactecl, of whom132
were scheduledto
be
tested.
The
71
participants
that were notscheduled
for
testing
either
did
not meetthe
criteriafor
the
class, were unableto
pay
the
$75
fee,
or were notinterested
in
taking the class.Of
the
132
scheduled, only97
weretested
andthe
remaining
35
participants
were nottested
because
ofillness,
conflictin
schedule,
personal
reasons, orlocatien.
Of
the
97
tested,
15
subjects
did
not enrollin
a classbecause
ef confiictin
time,
locatien,
health
status, andpersonal
reasonsleaving
82
jects
who enrolledin
rhe class,Thirty
did
not attend nineor more classes or were not
post-tested
and were noted
in
the
study.Reasons
for
not completingthe
studyed:
death
(1
participanO,
relocation(1
participanO,
drop
out
due
to
illness
ordriving
distance
(10
participants),
andpoor
attendance
(13
parzicipants),
A
total
of52
participants
eclnine or mere classes, completed
pre
andpost-testing,
andwere used
for
data
analysis.This
information
is
presented
in
Fig.
1.
Baseline
characteristics of the socio-demographic and
health
statusdata
for
the52
participants
are shownin
Table
1,
The
age range ofthe
subjects was53
to
91
years
{mean
=78.6).
Seventy-zhree
percent
ofthe
participants
werecategorized as
having
ahigh
physical
aetivitylevel,
with a
physical
compesite score ef11
or abeve, whereas27%
were
grouped
ashaving
alow
physical
activitylevel.
Females
resented
79%
ofthe
participants,
andthe
majority ofthe
participants
in
this
study were olderthan
70
years of age,
The
mosz common medical conditions reported amongticipants
were numbnessin
theieet
(25%),
heart
problems
(24%},
and arthritis(18%),
The
majority of older adultsdid
not use an ambulatory
device
(54%).
In
the yearbefore
the
intervention,
63.5%
ofthe
participants
reportedfalls
and
53.85%
were using morethan
five
prescription
drugs.
Prior
toparticipating
in
the
study, allsubjects metthe
following
inctusion
criteria:1)
age50
or older,2)
ableto
move
from
sittingin
a chairto
standingindependently,
3)
walk at
least
50-feet
without an assistivedevice,
4)
have
aed
balance
deficit
that
limits
functional
actlvities, orhave
a
history
and/orfear
offalls,
5)
pay
a non-refundabtefee
of
$75
for
the
eight-week e]ass and6)
obtain aphysician's
med-ca34tsrg8e
FAI12001toFalLID03 TotntContEctedN=203t
t
-w tptt b'otSeheduled<Reasons/time Sehod-tedforPre-Testing.N.-ISI
'
iconficts,personat,notinterested
Endhealth)X"1 thttam.
DidNotAttendPrc-Test aseaso]ls/imeconfiiets, persoflnl,n]dhealth)N4i,AtteodedPre-Tcst
/N;97lC5P=fat120DlrspringlO03
//SS=fmlt2003)' NotEnrolted(Reasens/ttmeconMets, vaeatlen,lttnessillN!IS]ocAtion,femily)personal,heAtth,tt
'
tt1
E"roued 1 N=Sl l{i3=fAIL!O021sptingleO]1"=rEUIO03} DidNotCempteteStudyMeaso]s/didnotattepd netmeetinclvs;oncriteriu,IPost-Test,didstudy]
liL-30 repeated C"mpletedStudyN=S2C3L-fslnOO!lspringlOO] 11=ffi1110D3)F-g.
1
Study
design
-
Flow
ofparticipants
through
the
study.ical
clearance.Subjects
were excludeclif
they were:1)
diag-nosed withdementia
orAlzheimer's
disease,
2}
diagnesed
with a cardiepulmonary cendition thatlimited
their
ability to exercise, or3)
were receivingformat
physical therapy concurrent tothe
class.After
meetingthe
inclusion
criteria, the subjects werethen
ellrolledin
one of eightcemmunity-based
FkellproofYTM
balance
and mobilitygroup
classesoffered
in
theFresnofClovis
areaduring
September
2002
toNovember
2003.
Each
subject wastested
one weekprior
to
and one week
fellowing
the
eight-weekFallprooftTM
class,Subject's
demographic
information
is
included
in
Table
1.
Design:
This
study was a repeated measure,quasi-experimental
studythat
analyzedthe
effect of an eight-week rmulti-dimen-sionalGreup-Structured
Balance
andMobility
Class
<GBMC)
on selectedbalance
ancl mebility measures oyertime.
We
examined eight classes that were
held
in
the
falt
alld spring of2002
through2003.
In
all examined'classes, eachpartici-pant
underwentpre-teszing,
GBMC
intervention,
andpost-testing.
Instrumentation
Each
participant
completedtwo
subjectivetests
andfive
objectivetests
to
determine
balance
innpairments,
Subjective
Tests:
Balance
Etficacl,
Scale
The
Balance
Ei7icacy
Scale
{BES)
wasdeveloped
by
Rose
Japanese Physical Therapy Association
NII-Electronic Library Service
JapanesePhysical Therapy AssociationThe
Effects
of anEight
Week
thllproofvTM
Table
1
Demographic
Characteristics
Class
Comparing
of
Subjects
atthe
High
andLow
Functioning
Participants
Beginning
efIntervention
(n=52)
319
Baseline
characteristicsHigh-level n=38%
ofHigh-levelLow-Level n=14%
ofLow-tevel# ofpatients
total
%
oftotal
Age:
51-60
61-70
71!80
81-90
91-100
3415151
7.910,539,539,5
2.6
1o373
7,1o2L455021,45
4318224
7.7
7.734.642.3
7,7
Gender:
Male
Female
1127
28.97Ll
o14
o100
1141
21,278,8
Diabetes
8
21,05
1
7,1
9
173
Heart
problems
22
57.9
7
50
29
55.8
Osteoporosis
8
21.05
4
28.6
12
23,1
Arthritis
16
42,1
6
42,9
22
42.3
Stroke
2
5.3
3
21,4
5
9.6
Parkinson's
5
132
1
7,1
6
IL5
Numbness
in
feet
22
57,9
9
64.3
31
59,6
Jeint
replacerment6
15,8
3
21,4
9
17,3
Use
of assistivedevice
10
26.3
14
100
24
46.15
Falls
in
the
previous
year
23
60,5
10
71,4
33
63,5
Prescription
medications/
O-5
6.15
1622
42.157.9
86
57.142.9
2428
46.1553,85
Pathelogies
areper
self report.the
individual
whileperferming
activities ofdaily
living
that
requirebalance.
Subjects
answered18
questions, rating on a scale ofO
to
100%,
theirlevel
of confidencein
performing
agiven
task
(e.g.
risefrom
a chair).The
totalscore eblainedwas
divided
by
1800
and multipliedby
100
to
get
aper-centage.
The
percentage
determined
the
individual's
confi-dence
in
maintainingtheir
balanee
during
activities ofdaTly
living,
Subjects
who scoredless.
than or equalto
50%
wereconsidered
to
have
low
self-confidence whileperforming
var-ious
activities requiringbalance3).
Composite
Pdysical
Furection
Scale
The
Conrposite
Physical
Funetion
(CPF)
Scale3)39)
consistsof
12
questions
addressing aperson's
abilityto
cempletedaily
activities, such asheusehold
chores and shopping, withor without
difficulty.
The
maxirnum scoreis
24,
Objective
Tests:
Berg
Balance
Scale
analFullerton
Advanced
Balance
71ests
Functional
balance
was assessed using one oftwe
tests:
the
Berg
Balance
Scale
(BBS)4e)
of14
items
orthe
Fullerton
Advanced
Balance
(F)IB)3)
Scale
of10
items.
Both
the
BBS
and
FAB
Scales
have
demonstrated
good
test-re-testrelia-bility
andinter
andintra-rater
reliability5}40),The
BBS
has
an excellent
inter-rater
reliabiUty ofO.96i4).
The
FAB
Scale
was
developed
as an alternative measure offunctional
limi-tations,
due
tothe
tendency
of theBBS
toproduee
ceilingeffects3).
Higher
functioning
adults withbalance
impairments
wM scorehigher
onthe
BBS,
which maybe
interpreted
ashaving
normalbalance.
An
individual
who scored14
orbelow
on the
CPF
wasdefined
as alower
functioning
individual
and
the
BBS
was administered.A
score aboye14
onthe
CPF
xvasdefined
as ahigher
functioning
individual
andthe
FAB
was administered.Both
tests
were scored using aO-4
ordinal scalefor
eachitem,
The
BBS
has
a maximurn score of56.
A
score of45
orbelow
is
associated with ahigh
riskfor
falls3).
The
items
onthe
test
progressively
challengethe
individual:s
balance
while
performing
narrewbage
of support activities begin-ningin
the
siltingpositien
and ending with a one-legged stanceposition,
The
test
additionally measured weightshift-ing.
turning,
and reaching,Materials
usedto
administerthe
BBS
include
the
following:
a stopwatch:two
straight-backed chairs:(one
with armrests and one without armrests); a yard-stick; a slipper: and a6-inch
bench.
The
FAB
is
also afunctienal
test
with a maximum scoreof
40.
Unlike
the
BBS,
it
challenges sensoryintegration
withtasks
such as standing onfoam
with eyes closed andwaik-ing
withhead
turns,
Other
items
include
stepping up andover an ebstacle,
jumping
for
distance,
andtandem
walkTng.Scores
onthe
FAB
Scale
also correlate with scores obtained usingthe
BBS3).
According
toDr.
Debra
Rose
atCalifornia
320
re\rkta\
State
University,
Fullerton,
aF)IB
score ef30!40
places
the
individual
at riskfor
falls
{personal
communicatien),Materials
used
to
administerthe
FAB
include
a stopwatch, astick, a
12-inch
ruler, apen
orpenciL
a6-inch
bench,
ametronome, masking
tape,
two
stackedAirExe
balance
foam
pads,
and one or more12-inch
lengths
of non-slip material.
Modified
Clinical
71est
of
Sensory
Jnteraction
in
Balance
CrsIBJ
The
purpose
ofthe
M-C71SIB7)
Ts
to
identify
whetherthe
use of sensory
information
in
different
sensory environmentsare normal or abnormal,
Subjects
were requiredte
stand
quietly
for
30
seconds. withfeet
shoulder width apart andarms
folded
acrosstheir
chestduring
each ofthe
following
four
conditions:1}
eyes open,firm
surface,2)
eyes c}osed,firm
surface,3}
eyes open,foam
surface(two
stackedAirExO
balance
foam
pads}
and4)
eyes closed,foam
surface.The
individual
was scoredby
the
sum of thefour
collditions,with
the
maximum scorebeing
l20
seeonds,
50-Fbot
Wdlk
71est
The
50-}7bot
IVdlh
flest
is
used toidentify
functional
itations
ofgait
by
measuring variability of velocity3).Each
subject was askedto
walk atotal
distance
of70
feet,
first
at a
preferred
speed andthen
at afast
speed.The
distance
between
the10-foot
and60-feot
markers was timed.The
purpose
ofthis
test
is
to
determine
if
the
subjectis
ableto
adapt
hisfher
gait
speedto
the
changeln
task
demands3),
It
has
been
welldocumented
that
low
or slowgait
speedsare associated with an
increased
riskfor
falls3)4i),
"Wttlleie-71ilhie"712st
The
"Wtxlkie-Talhie''
Test
is
usedto
measurethe
subject'sability
to
divide
hisfher
attentionbetween
tasks3).
This
test
was
perforined
asthe
investigator
walked withthe
subjectto
thelocation
of the50-17bot
Wdlk
flest.
The
subject wasasked an epen-ended
question
that required more than a"yes''
or `'no" answer.
A
positive
score was recordedif
the
subject
stopped walkingto
answerthe
question.
Conversely,
a negative score was recerded
if
the
subject couidue walking while
he/she
answeredthe
question.
Senior
Fitness
7lest
The
Senior
Fitness
Test,
developed
by
Rikli
andJones42),
consisted of a six-test
battery
that
incLudes
testing
upperand
lewer
bedy
strength,flexibillty,
aerobic endurance, and
dynamic
balance
and agility.Materials
usedduring
testing
include
a stopwatch, maskingtape,
a standard straight-backchair without arms,
five
or eightpound
dumbbells,
a36-inch
measuring
tape,
and a eone,This
assessmenthas
strated reliability and validity42) and was
developed
to
test
underlying
physical
impairments
associated withfunctional
mobility.
The
resultsfrom
thesetests
were comparedto
norm-referenced standards
based
on a sample ef7,l83
munity-dwelling elder adults ranging
from
60-94
years
ofage3)42),
Proeedures
Subjeets
were scheduledfer
pre-testing
one weekprior
te
the
start of theirFagiproof7TM
class,Testing
toek
place
at3
different
sitesin
the
Fresno
community wherethe
Fallproof!TM
classes wereheld.
Subjecis
were scheduled accordingto
time
and convenience oflocation.
Prior
to
testing,
allsubjects signed aninformed
consentdocument
that
was approvedby
the
University
Committee
on
the
Protection
for
Human
Subjects.
Next,
each subjectfilled
out aHealth
Activity
Questionnaire
that
consisted ofgeneral
health
questions,
anydiagnosed
medical conditions,a
histery
offalls,
the
CPF
Scale,
as well as activityleveL
In
additionto
completingthe
Health
Activity
Questionnaire,
each subject completed
the
BffS.
Then,
aninvestigator
whowas a
Certified
Balance
andMobility
Instructor
(CBMI}
per-formed
a comprehensive assessment ofbalance
andmobili-ty
skills,The
CBMI
used theFAB
orBBS,
50-Foot
Walk
7lest,
''Wdlhie-7lrlhie"flest,
Senior
Fitness
Test,
andM-C71SiB
to
completethe
balance
assessmentfor
each indi-viduaLEach
CBMI
underwent130
hours
oftheoretical
coursework and examinations, along with50
heurs
eftotal
contact timethrough
distance
learning
atCalifornia
State
University,
Fresno
and was sponsoredby
California
State
University,
Fullerton
in
orderto
become
aCertified
Balance
and
Mobility
Instructor.
The
pregram
collsisted ofthe
the-oretical
basis
for
balance
and mobility,the
rationalefor
develeping
a multidimensionalfall
risk reductionprogram,
analyzing
the
role ofintrinsic
and extrinsicfactors
that
are associated withfalls,
and assessment ofbalance
andmobili-ty,
During
the
certificationprocess,
eachinvestigator
wasevaluated and
tested
by
the
course'sinstructors
to
ensureproper
administration andinterpretation
of assessmenttests,
The
orderfor
testing
subjects was unsystematic andbased
onthe
availability
of
equipment.Data
was recorded on a score sheet as each test was administered.Ifa
subject scored14
orbelow
on theCPF
Scale,
theBBS
was conductecl,During
theBBS
the
subject was askedto
perform
the
fol-lowing
fourteen
items:
standingfrom
a seatedposition,
stand-ing
unsupported, sitting unsupported, standingto
sit,trans-fers,
standing with eyes ciosed: standing withfeet
together;
reaching
forward
with outstretched arm;picking
up aslip-per
from
the
floor;
turning
to
look
behind
everleft
and rightshoulders;
turning
360
degrees:
toe
tapping
on a sixinch
step-stool:tanclem
stance; and standing on oneleg.
Conversely,
if
the
subject scored above14
enthe
CPF
Seale,
the
FAB
was administeredin
pLace
ofthe
BBS,
During
theFAB
the subject was askedto
perform
the
fol-lowing
10
items:
standing withfeet
together, eyes cLosed: reachingferward
to retrieve all objectheld
at shoulderJapanese Physical Therapy Association
NII-Electronic Library Service
Japanese Physical Therapy AssociationThe
Effects
of anEight
Week
FaliproofrTM
CIass
height
with outstretched arm; a turn360
degrees
in
a rightand
left
direction;
stepping up and over a sixinch
bench:
tandem
walking; standingon
one
leg:
standing on4-inch
foam
with eyes closed; a
two-foQted
jump;
walking withhead
turns; and reactive postural controL
The
M-CTSIB
wasperformed
by
having
the
subject standquietly
for
30
seconds withfeet
shoulder width apart and arms crossed overtheir
chestduring
each ofthe
follewing
four
conditions/1)
eyes open,firm
surface,2}
eyes closed,firm
surface,3)
eyes open,foam
surface, and4)
eyes closed,foam
surface,Each
condition consisted ofthree
trials.
If
the
subject was ableto
maintainhislher
balanee
for
the
full
30
secondsin
the
first
triaL
theinvestigator
proceeded
to
the
next sensory cendition.If
the
subjectlost
hisfher
balance,
lifted
the
arms or openedthe
eyes, then an average of allthree
trials
was recorded.The
individual
was scoredby
the
sum ofthe
four
conditions. withthe
maximum scorebeing
120
seconds.
The
50-Fbot
Wdlk
11est
andthe
"Wdlhie-fkelkie"11est
wereperformed
aspreviously
described.
All
sixitems
included
in
the
Senior
Fitness
Test
wereadministered
in
accordanceto
the
protocols
outiinedin
the
Senior
Fitness
Manua142}.
Upper
extrernity strength wasassessed
by
performing
the
Arm
Curt
7lest.
The
subject was allowedto
practice
oneto
two
bicep
curlsto
checkfor
cor-rectform
prior
to
performing
the
test.
A
score wasgiven
by
countingthe
number ofbicep
curls cempletedin
thirty
seconds withfemales
using afive-pound
durnbbe]1
and males using an eight-pounddumbbell.
Lower
extremity strength was measuredby
performing
the
Chair
Stand
flest.
A
score wasgiven
by
countingthe
number oftimes
the
subject steodfrom
an armless chair withhands
crossed overhisfher
chestin
30
seconds.The
subject was allowedto
practice
standing up onetime
before
the
test
triaL
Upper
extremi-ty
flexibility
was evaluatedby
performing
the
Back
Scratch
Test.
The
subject was askedto
reach onehand
overthe
ipsilateral
shoulder anddown
the
back;
the
otherhand
reached around
the
back
and uptowards
the
otherhand
in
an attemptto
touch
or overlapthe
extendedthird
digits
ofboth
hands.
The
subjectpracticed
with eaeh armto
deter-mine
hislher
preferred
arm.After
praeticing
zwo times usingthe
preferred
arm,two
test
trials
wereperformed.
The
score wasthen
recordedto
the
nearest ihinch
measuringthe
dis-tance
of overlap erdistance
between
the
tips
efthe
3rd
dig-its.
A
minusO
score was recerdedif
the
3id
digits
did
notteuch
ancl aplus
<+)
seere recordedif
they
everlapped.The
better
score ofthe
two
trials
was circled.Lower
extremityftexibility
was assessedby
performingthe
Chair
Sit
andReach
Test,
Seated
in
a chair,the
subject reachedfor
onefoot
keeping
the
knee
fully
extended while the oppositeleg
was
kept
in
afiexed
position.The
subjectpracticed
the
testComparing
High
andLow
Functiening
Participants
321
on
both
legs
todeterrnine
which wasthe
preferred
leg,
Once
determined,
the subjectpracticed
two
times
to
warm-up,then,
two
test
trials
wereperformed,
The
distance
(inches)
between
the
tip
ofthe
toe
andtips
ofthe
3'd
digits
weremeasured and recorded,
The
midpoint atthe
toe
representedthe zero
point.
If
their
reach was short ofthis
point,
the
distallee
was recorded as a minus(-)
score;if
the
middle
gers
touched
their
toe,
a score a zero was recorded; andif
the
subject reachedpast
the
midpoint oftheir
toe,
the
tance
was recorded as aplus
(+)
score.Aerobic
endurancewas ascertained
by
administeringthe
2-minute
Stqp
11est,
The
stephelghz
was establishedfor
eachindividual
by
ing
the
subjects stand sideways nextto
the wall with armsresting
by
their sides.The
wall was marked with apiece
of
tape
atthe
height
ofthe
tip of the middiefinger.
The
tape
representedthe
minimumknee-stepping
height
for
the
subject.
The
subject was askedto
marchin
place
liftTng
the
knees
abovethe
tape
for
two
minutes.The
score wasthe
number of
full
steps completedby
onelower
extremTtyin
two
minutes.Dynamic
balance
and agility wasdetermined
by
the
subject'sperformance
onthe
8-Fbot
VP
andGo
Tlest.
Subjects
weretimed
to
seehow
quickly
they could standfrom
an armless chair, walk around a coneplaced
8
feet
away, and return
to
the
originatposition.
The
subject wasallowed one
practice
trial
fo11owed
by
two
test
trials,
The
better
score ofthe
two
test
trials
wascircled.
The
nents of
the
Senior
Fitness
Test
were modified anded
if
the
subject wasincapable
ofperforming
the teszper
protocol
(i.e.,
usinghands
to
push
upfrom
the chairfor
the
Chair
Stand
7kest,
orholding
ontethe
wall!chairfor
the
minute
Step
7lest).
After
pre-testing,
the
results ofthe
seniorfirness
tesr
zverediscussed
with each subject, comparinghislher
scoresto
normative
data.
In
addition,the
EAB
orBBS,
50
17bot
Wdlle
Test,
'tWttlkie-7kelfeie"
Test
andM-CTSIB
were analyzedby
each
CBMI
to
determine
anybalance-related
impairments
and
the
results were recorded on anindividualized
Fal(proof.tTM
report card.Prior
tethe
intervention,
cian's clearance was obtained
for
each subjectthat
gave
mission
for
participation
in
the
Fal(proof!TM
class.
Following
the
eight-weekinzervention,
subjects were
tested
adhering zothe
sameprocedures
deserlbed
above.
Intervention
Subjecls
who metthe
inclusion
crlteria wereplaced
in
one of eight
FtzllprooffTM
classesthat
wereheld
from
spring2002
through
fall
2003.
The
primary
instructor
for
the
week
group
class was aCBMI.
In
additionto
the
CBMI,
graduaze
physical
therapy students, aspart
ofthe
graduate
curriculum, underwent
12
hours
oftraining
to
assistin
ance re-training techniques
taught
by
afaculty
member of
322
ve#fith7
California
Sate
University,
Fresno,
whois
also aCBMI,
Based
on
the
impairments
identMed
through
the
pre-testing
sions,
the
primary
instructor
for
the
classdeveloped
priate
lesson
plans
for
each class sessien,The
lesson
plans
were
based
onthe
theory
and applicationstaught
in
the
Balance
andMobility
Certification
course.The
CBMI's
ated a struetured and
progressive
program
of activitiesspecifically
designed
to addressthe
multipledimensions
that
contribute
to
balance
and mobility.The
Fallproof!TM
cere
program
components consTsted of center ofgravity
control
training,
mulitsensorytraining,
proactTve
and reactive
tural
strategytraining,
gait
pattern
enhancementtraTning,
and strength and
flexibility
training,
These
elements weresystematically
introduced
andprogressed
from
alow
to
high
level
ofbalance
challengeby
manipulatien ofthe
ment and
task
demands.
Environmental
changesincluded
decreased
availability of vision and altered support surfaces.Task
demand
changesinclude
decreasing
the
base
of
port,
varying armpositions,
and adding cognitivetasks.
Each
subject
in
the
classperformed
the
activity at anate
level,
based
ontheir
individual
impairments
asmined
by
the
CBMI,
The
class mettwo
times
a weekfor
eight weeks witheach sessioll
lasting
for
onehour.
For
the
first
10-15
utes,
the
instructor
Ied
the
classin
a warm-upthat
porated
gait,
range of motion, strength and coordination,
Throughout
the
intervention,
the
subjectsperfermed
ties
as agroup
andthen
divided
upin
to
sub-groupsto
ticipate
in
specificbalance
activities.Each
balance-related
activity was
demonstrated
along withthe
rationale ofhow
it
can maximize anindividual's
sensoryTntegration
ness within
the
home
and community.The
classes endedwith a
10-minute
coel-downthat
consisted ofstretching,cleep
breathing
and a review of activities.Throughout
the
vention,
both
the
CBMI
andphysical
therapy
graduate
dent
helpers
provided
assistance andguarding
to
ensurethe
safety of
the
subjects at alltimes.
The
ratios ofhelpers
to
subjects ranged
from
1:1
to
1/3
amongthe
eightFZillproofYTM
classes.
In
this
multi-dimensional approachto
balance,
extrinsic and
intrinsic
factors
were addressed with each subjectally,
During
the
secondto
third
week, the subjects were
given
ahome
safety check effsheetin
orderto
assesstheir
heme
conditiensfor
extrinsicfacters,
which could contribute
to
falling.
The
home
safety check offlist
provided
ness of
potential
hazards
throughout thehome
that
eouldcreaze a
fall,
Suggestions
weregiven
for
modificationto
ate a safer environment,
At
the
fourth
anclfifth
week,the
subjects were
given
anindividuaEized
home
exercise
gram
(HEP)
that
consisted of upper andlower
extremitystretching and strengthening with a
theraband,
head-eye
eg34#eg8e
ceordmalion exercises, and aczivities
that
challenged multi-sensory systems.Data
analysis
The
scores ofthe
fifty-two
subjects who metthe
inclu-sion criteria were usedfor
data
analysis,Repeated
measurestwo-way
analysis of variance(ANOVA}
wasperformed
onten
outcome variables(BES,
M-CTSIB,
50-Foot
Wdlk
lpre・
ferred},
Chair
Stand
7lest,
Arm
Curl
71est,
2
Minute
Step
71!st,
Chair
Sit
andReach
7lest,
Baefe
Scratch
flest,
8-Foot
UP
andGo
11?st,
andFAB
orBBS.)
usingStatistical
Package
for
the
Secial
Sciences
{SPSS,
Microsoft
Windows
version11.0a}.
The
"Wdlfeie-lhlkie"71?st
was not used
for
data
analy-sisbecause
51
ofthe
52
subjects received a negative scoreleaving
no roomto
demonstrate
change.Descriptive
data
are reportedfor
variables ofinterest
{mean,
standard devi-ation, and95%
confidenceinterval)
usingMicroseft
Excel
2000e.
The
twe
independent
variablesin
this study weretime
(pre-post)
andgroup
(high
orlow).
The
between-groups
variance explainsthe
independent
variable effects, andthe
error variance accountsfor
all sources ef variationunex-plainecl
by
treatment.
Because
this
design
incorperates
twoindepelldent
variables, we were ableto
askthree
questions
of
this
data:
1,
Factor
A
(time):
What
is
the
effect ofTnter-vention on subjects regardless of
their
status?2.
Factor
B
{group):
Was
there
adifference
in
perfermance
between
low
level
andhigh
level
subjects?3.
Interaction:
Did
the
inter-vention effect
depend
on status of subjects?
Results
Table
2
presents
two-factor
repeated measureANOVA
fer
two
independent
variables:time
(prepost)
andgroup
(high
level-low
leveb.
There
was a significantimprevement
overtime
in
alleutcome measures exceptChair
Sit
andReaeh
712st.
There
was a significant effect ongroup
statusfor
BES
(Fig.2),
M-C71glB
(Fig.3),
BBSfFAB
(Fig,4),
Chair
Stanel
Tlest
(Fig.
5),
2-minute
Stqi)
71est
(Fig.
6),
and8
Fbot
tlp
andGo
71est
{Fig.7).
There
was aninteraction
oftime
by
group
for
the
M-C7SIB
and8-Fbot
Clp
andGo
71est
withthe
low
level
group
demonstrating
greater
improvements
(Fig.
3
and7).
Results
frem
the
FAB
andBBS
tests
arepresented
in
Table
2,
which shows significant main effectfrom
the
inter-ventien;
however
there
was neTnteractien
between
groups
(Fig.4}.
The
majority ofthe
partTcipants
(88%)
participated
in
75%
or more of the classes(Table3).
Statistical
analysis,two-factor
repeated measureANOVA,
indicates
no signifi-cantdifference
in
the
outcome measuresbased
onthe
num-ber
of classesin
whichthe
subjectsparticipated
<p>O.05).
Discu$sion
Japanese Physical Therapy Association
NII-Electronic Library Service
JapanesePhysicalTherapy AssociationThe
Effects
of anEightWeekFZillproofVTM
CIass
ComparingHigh
andLowFunctToningParticipants323
Table
2Two-wayRepeated
MeasureANOVA
forTen
OutcomeMeasures
OutcomeMeasures
Mean
Pre-Test
n=38Highlevel
(
±SD}
MeanPost-Test
n=38High-level{
±SD)
MeanPre-Test
n=14Lowlevel
(
±SD)
MeanPest-Test
n=14Lowlevel
(
±SD)
MInain
Effect
M
terventlonain
EffectStatusMain
Effect
Stalus
X
Intervention
p
valueBES
66,91
±18.472.53
±16.6
43,29
±14.653.38
±23.1O.O02
S
o.ooo
s
O.349
NS
M.CTSIB
I04,23
±16.1103,91
±15.6
82.42
±13.193,28
±12,4O,O14
S
o.ooo
s
O,O09
S
50-Foot
Walk
PreferredTest
3.17
±3.142,30
±L94
5,54
±8.263,42
±3.05O,O19
S
O.I03
NSO.321
NS
ChaTrStand
Test
8.84
±3,229,47
±3.76
5,71
±3.05Z32
±3.04O,O13
S
O,O09
S
O.269
NS
ArmCurl
Test
11,50
±4.7813.08
±4.94
10.64
±3.1811.57
±1.51O.024
S
O.350
NSO.550
NS
2-pt(inuteStep
Test
62.61
±2L273.89
±21,O
46,50
±17.951.79
±14.4O,OOI
S
O.O02
S
O.208
NS
Chair
Sit
Testand
Reach
-4.13
±
5.58-3.85
±5.18
-5.54
±4.57-5.14
±5.69O.509
NSO.400
NSO.909
NS
BackScratch
Test
.6.53
±5.68-6,331
±5,77
-6,64
±5.44-4,157
±6.41O,048
S
O,545
NSO.090
NS
8-FootUp
andGo
Test8.81
±2.308.65
±2.88
12.93
±3.01IL21
±2.34O.O02
S
o,ooo
s
O,O07
S
#BBSbinedand
FAB
com-52.7
±
16259.87
±17,5
59,74
±16.572.14
±l3.7o.ooo
s
O,047
S
O.190
NS
p<O.05"%ofstatistically
significant. maximuln,1OO
90
80ge
70U
6o]fi
50>E
40g
3o
20
10
o
Fig
High
level
Low
level
Total
.2
Mean
percentage
value efBES
between
low
level
groups,
*Indicates
a significantment of confidence
level
(p<O.05)
in
the
and overall tetal
post-test
scores.140120100m
80v88
6oco4020
Fig
o
high
andimprove-low-levetHigh-level
Low-level
Tetal
.
3
Mean
M-CTSIB
scores comparinghigh-level
and
low-level
subjects.Error
bars
representsubjects standard
deviation,
'Indicates
a
significant
difference
(p<O.05)
in
thelow-Ievel
and overalltotal
post-test
scores.100
90
80gE
70'G'
6oE6
50ge
40
30
20
"o
o
Fig.
4
14
12
dOv=es
8se6--.co
4
2
o
BBS
FAB
Total
BBS
andFAB.
Low
level
group
took
BBS
andhigh
level
group
took
FAB.
*'Indicates
a significantimprovement
{p<O,05)
in
the
BBS
andFAB
post-test.
Error
bars
representbetween-subjects
stan-dard
deviation.
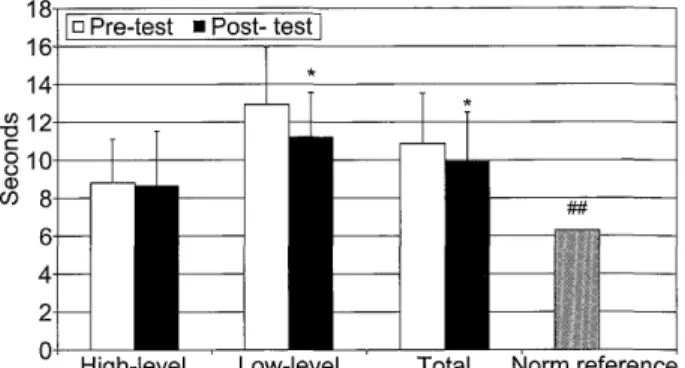
Fig.
5High-levelLow-levelTotalNormreference
Comparison
ofChair
Stand
Test
between
high
andlow
level
groups.
"Indicates
a significantimprove-ment