ない用量で投与されている例が多数報告され3),リ バーロキサバンの市販後調査では減量投与(10 mg) されている患者のうち,51%が不適切な減量であるこ とが示された.現在までに不適切な減量(“off-label" under-dose)投与が心房細動患者の塞栓症や出血イ ベント発症に与える影響は分かっておらず,大規模 臨床試験で示された効果が得られているのかは疑問 である.本研究では,リバーロキサバンの “off-label" under-dose投与患者の心血管イベント発症に与える 影響を,適正使用患者群と比較検討した. 対象および方法 対象患者 2012 年 8 月から 2015 年 12 月までに関西医科大学 附属病院で,Cockcroft-Gault 式で算出したクレアチニ ンクリアランス 50 ml/min 以上かつ CHADS2スコア 1 関西医科大学内科学第二講座循環器内科 (受領:令和 2 年 5 月 18 日) 日本臨床生理学会雑誌 Vol. 50, No. 5, 2020.
原著論文
"Off-label" under-dose リバーロキサバン投与の
心房細動患者における心血管イベント発症に関する検討
諏 訪 惠 信,宮 坂 陽 子,原 田 翔 子,仲 井 え り
谷 口 直 樹,塩 島 一 朗
要 約 近年,心房細動患者の塞栓症予防に直接経口抗凝固薬が使用可能となったが,添付文書に 従っていない不適切な減量(“off-label" under-dose)投与が及ぼす影響についての報告は少な い.そこで本研究は,2012 年から 2015 年に当院で新規にリバーロキサバンが投与された非弁 膜症性心房細動患者で,腎機能が保たれた連続患者を対象とし,塞栓症と心血管死の複合イベント と出血イベントを調査した.リバーロキサバン 10 mg 投与患者を “off-label" under-dose 群(N = 65)とし,15 mg の適正使用群(N = 235)と比較検討した.対象患者 300 例の平均観察期 間 13 カ月中に,複合心血管イベント 13 例,出血イベント 22 例を認めた.Cox 比例ハザード解 析で,“off-label" under-dose 群は複合心血管イベントの有意な危険因子であったが(ハザード比= 3.86, P=0.03),出血イベントでは有意ではなかった.つまり,リバーロキサバンの “off-label" under-dose投与患者は塞栓症と心血管死のイベントが有意に増加したが,出血の抑制は認めら れなかった. 研究背景・目的 心房細動は,日常臨床でよく遭遇する不整脈である. 心房細動による脳塞栓や心不全など心血管合併症は大 きな問題とされる.脳塞栓予防には 50 年以上ワルファ リンが使用されてきたが,薬効の不安定さ,食品・薬 剤との相互作用が煩雑で,しばしば重篤な出血や脳塞 栓が認められた.2011 年から本邦で使用可能となっ た直接経口抗凝固薬 (DOAC)は,ワルファリンと比 較した欧米の大規模臨床試験1, 2)で,ワルファリンに 劣らない血栓塞栓予防効果と,出血性合併症の少ない 高い安全性が示された. しかし日常臨床においては,添付文書に従ってい点以上で,新規にリバーロキサバンが投与された非弁 膜症性心房細動の連続患者を対象とした.リバーロキ サバン 15 mg 群を standard dose 群,10 mg 群を “off-label" under-dose 群とした.対象患者の心血管イベン トを,死亡もしくは 2016 年 9 月まで前向きに追跡調 査を行った.本研究は,関西医科大学倫理審査センター の承認を得て実施している(承認番号 H1612108). データ収集 DOAC 処方時の年齢,性別,身長,体重,血圧, 心拍数,腎機能,ヘモグロビン値,心房細動の分類(発 作性・持続性),基礎疾患,既往歴,服用薬の情報を 収集した. 項目の定義 貧血は,ヘモグロビン値が男性 13 g/dl 未満,女性 12 g/dl未満と定義した4).高血圧は,異なるタイミ ングで計測した血圧が収縮期 140 mmHg 以上,拡張 期 90 mmHg 以上が 2 回以上,もしくは降圧薬を使用 している患者と定義した.糖尿病は,空腹時血糖値 126 mg/dl以上,随時血糖値が 200 mg/dl 以上,もし くは糖尿病治療薬を使用している患者と定義した.心 不全の既往歴は,フラミンガム基準5)に基づいて診 断した.脳梗塞の既往については,画像と専門医によ る診断と定義した. 心血管イベント 主要評価項目は,心房細動に伴う塞栓症と心血管死 の複合エンドポイントとした.副次評価項目は出血イ ベントとした.出血イベントは,大出血と小出血に分 類した.大出血の基準は,ISTH 基準6)に従い,致死 的出血,ヘモグロビン値が 2 g/dl 以上低下する出血, 2単位以上の輸血を要する出血とした.小出血は,大 出血以外の全ての出血とした. 統計解析 2 群間比較は,連続変数は t 検定を,カテゴリカル 変数はχ2検定を用いた.Cox 比例ハザード解析を用 いてイベント発症に関与する因子を検討した.カプ ランマイヤー曲線を用いて “off-label" under-dose 群 と standard dose 群のイベント発生の差異を図で示し た.全ての統計解析は IBM SPSS Statistics software version 24.0 (SPSS Inc., IBM, Somers, New York, USA) を用いた.P < 0.05 を統計的に有意とした.
結 果
組み入れ基準を満たした全患者 300 例の背景と, “off-label" under-dose 投与の有無で分けた患者背景
All patients Standard dose “Off-label”
(N = 300) (N = 235) under-dose P value (N = 65) Age (years) 68 ± 10 66 ± 10 75 ± 9 < 0.001 Male gender 213 (71) 172 (73) 41 (63) 0.08 Height (cm) 163 ± 9 164 ± 8 161 ± 10 0.02 Body weight (kg) 64 ± 12 65 ± 11 62 ± 12 0.18
Body mass index (kg/m2) 24 ± 4 24 ± 4 24 ± 4 0.90
Systolic blood pressure (mmHg) 130 ± 22 131 ± 23 129 ± 21 0.59
Diastolic blood pressure (mmHg) 81 ± 15 81 ± 16 77 ± 14 0.06
Heart rate (beats/min) 86 ± 22 86 ± 23 83 ± 19 0.26
Creatinine (mg/dl) 0.80 ± 0.19 0.78 ± 0.18 0.87 ± 0.24 < 0.001
Creatinine clearance (ml/min) 80 ± 23 84 ± 23 63 ± 13 < 0.001
Paroxysmal atrial fibrillation 162 (54) 129 (55) 33 (51) 0.33
CHADS2 score 1.7± 1.3 1.6 ± 1.3 2.0 ± 1.4 0.04
Anemia 54 (18) 39 (17) 15 (23) 0.15
Hypertension 175 (58) 134 (57) 41 (63) 0.23
Diabetes mellitus 78 (26) 60 (26) 18 (28) 0.42
History of heart failure 66 (22) 49 (21) 17 (26) 0.23
History of cerebral infarction 59 (20) 49 (21) 10 (15) 0.21
Combined antiplatelet therapy 4 (1) 3 (1) 1 (2) 0.63
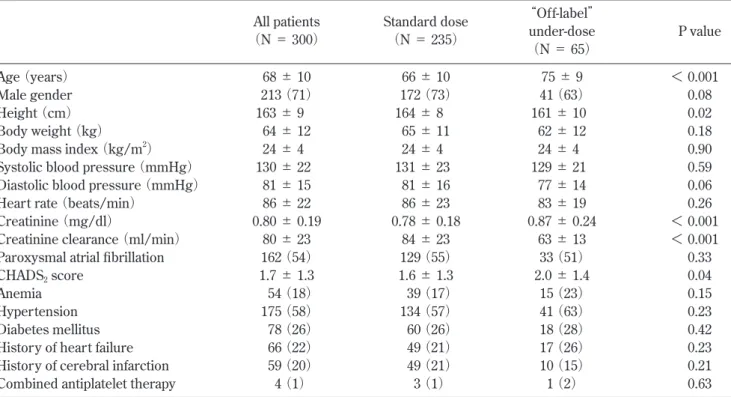
Table 1 Baseline clinical characteristics.
Values are given as mean± SD or number (%). Differences were evaluated with Chi-square analyses (categorical variables) and 2-sample t tests (continuous variables).
の比較を Table 1 に示す.“off-label" under-dose 投与 は 65 例 (22%) であった.全患者の平均年齢は 68 ± 10歳 で,standard dose 群 66 ± 10 歳 に 対 し て “off-label"under-dose 群 は 75 ± 9 歳 と 有 意 に 高 齢(P < 0.001)であった.全患者では男性が 213 例(71%) で,standard dose 群 と “off-label" under-dose 群 に 有 意差は認めなかった.全患者の平均クレアチニンが 0.80± 0.19 mg/dl,平均クレアチニンクリアランスが 80± 23 ml/min であったが,“off-label" under-dose 群 では standard dose 群に比し,クレアチニンは有意に 高く,クレアチニンクリアランスは有意に低値であっ た.全患者の平均 CHADS2スコアは 1.7 ± 1.3 であり, “off-label" under-dose 群では standard dose 群に対し有 意に高値であった.全患者の基礎疾患は,貧血 54 例 (18%),高血圧症 175 例(58%),糖尿病 78 例(26%),
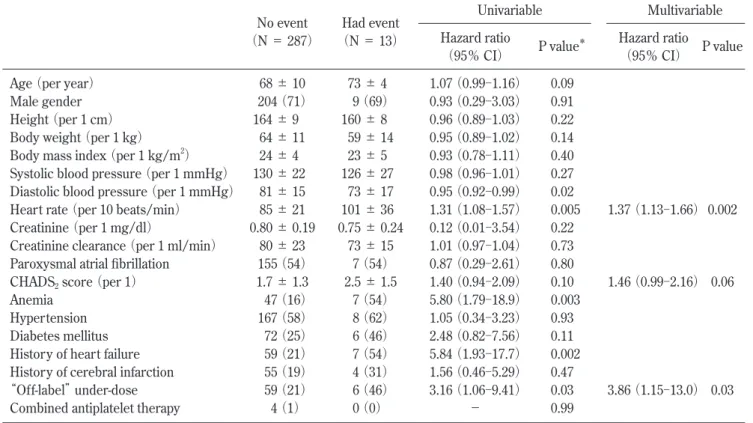
心不全既往 66 例(22%),脳梗塞既往 59 例(20%) であり,standard dose 群と “off-label" under-dose 群に 有意差を認めなかった.多変量解析にて,“off-label" under-dose投与患者の背景を検討したところ,年齢(10 歳毎 ; ハザード比= 1.99, 95%信頼区間= 1.372.92, P< 0.001)とクレアチニンクリアランス(10 ml/min 毎 ; ハザード比= 0.64, 95%信頼区間= 0.51-0.80, P < 0.001)が “off-label” under-dose 投与の独立した因子と なった. 複合心血管イベント 平均観察期間 13 ± 11 カ月で,複合心血管イベント は 13 例(4%;塞栓症 4 例,心血管死 9 例)であった. 塞栓症の詳細は,脳梗塞 3 例,網膜中心動脈閉塞症 1 例であった.心血管死の詳細は,心不全死 3 例,心室 性不整脈による突然死 6 例であった.Table 2 に複合 心血管イベント発生に関与する単変量解析,および多 変量解析結果を示す.年齢,性別に有意差は認めず, 処方時の拡張期血圧,心拍数,貧血,心不全既往,お よび “off-label" under-dose 群が有意な因子であった. 多変量解析では,“off-label" under-dose 群 (ハザード 比= 3.86, 95%信頼区間= 1.15-13.0, P = 0.03)と,処 方時の心拍数 (10 拍/分毎 ; ハザード比= 1.37, 95% 信頼区間= 1.13-1.66, P = 0.002) が独立した複合心血 管イベント発症の危険因子であった.CHADS2スコア 増加はイベント発症に有意な傾向を認めた(P = 0.06). Fig. 1 に “off-label" under-dose 群 と standard dose 群 別のカプランマイヤー曲線を示す.“off-label"
Univariable Multivariable
No event Had event
Hazard ratio P value* Hazard ratio P value
(N = 287) (N = 13)
(95% CI) (95% CI)
Age (per year) 68 ± 10 73 ± 4 1.07 (0.99-1.16) 0.09
Male gender 204 (71) 9 (69) 0.93 (0.29-3.03) 0.91
Height (per 1 cm) 164 ± 9 160 ± 8 0.96 (0.89-1.03) 0.22
Body weight (per 1 kg) 64 ± 11 59 ± 14 0.95 (0.89-1.02) 0.14
Body mass index (per 1 kg/m2) 24 ± 4 23 ± 5 0.93 (0.78-1.11) 0.40
Systolic blood pressure (per 1 mmHg) 130 ± 22 126 ± 27 0.98 (0.96-1.01) 0.27 Diastolic blood pressure (per 1 mmHg) 81 ± 15 73 ± 17 0.95 (0.92-0.99) 0.02
Heart rate (per 10 beats/min) 85 ± 21 101 ± 36 1.31 (1.08-1.57) 0.005 1.37 (1.13-1.66) 0.002 Creatinine (per 1 mg/dl) 0.80 ± 0.19 0.75 ± 0.24 0.12 (0.01-3.54) 0.22
Creatinine clearance (per 1 ml/min) 80 ± 23 73 ± 15 1.01 (0.97-1.04) 0.73 Paroxysmal atrial fibrillation 155 (54) 7 (54) 0.87 (0.29-2.61) 0.80
CHADS2 score (per 1) 1.7 ± 1.3 2.5 ± 1.5 1.40 (0.94-2.09) 0.10 1.46 (0.99-2.16) 0.06
Anemia 47 (16) 7 (54) 5.80 (1.79-18.9) 0.003
Hypertension 167 (58) 8 (62) 1.05 (0.34-3.23) 0.93
Diabetes mellitus 72 (25) 6 (46) 2.48 (0.82-7.56) 0.11
History of heart failure 59 (21) 7 (54) 5.84 (1.93-17.7) 0.002 History of cerebral infarction 55 (19) 4 (31) 1.56 (0.46-5.29) 0.47
“Off-label” under-dose 59 (21) 6 (46) 3.16 (1.06-9.41) 0.03 3.86 (1.15-13.0) 0.03
Combined antiplatelet therapy 4 (1) 0 (0) - 0.99
Table 2 Univariable and multivariable model for prediction of combined cardiovascular event in AF patients.
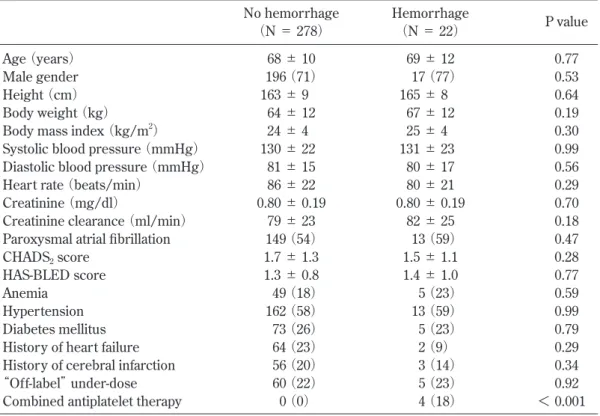
dose群は,有意に複合心血管イベントが多いことが 示された (Log-rank P = 0.03). 出血イベント 平均観察期間 13 ± 11 カ月で,出血イベントは 22 例(7%;大出血 3 例,小出血 19 例)であった.大出 血 3 例の内訳は,脳出血 2 例,上部消化管出血 1 例で あった.出血イベントについての単変量解析結果を Table 3に示す.出血イベント群と非出血群の HAS-BLEDスコアに有意差は認めなかった.抗血小板剤内 服が出血イベント群で有意に高かった(P < 0.001). しかし,多変量解析では “off-label" under-dose 投与を 含め,有意な因子は認めなかった. 考 察 今回の研究結果で得られた要点は,1) リバーロキ サバンの “off-label" under-dose 投与患者は,複合心血 管イベントが独立して有意に多かった,2) “off-label" under-dose投与患者で,出血イベントの有意な抑制 は確認できなかった. "off-label" under-dose 投与と複合心血管イベント 2013 年 10 月に発表されたリバーロキサバンの特 定使用成績調査における “off-label" under-dose 投与 は 39%,2,086 名の非弁膜症性心房細動患者を集めた RAMSES study7)で は 30.4 % に “off-label" under-dose 投与がなされており,本研究の 22%も含め,日常臨 床である一定の頻度で行われていることが示唆され た.“off-label" under-dose 投与の要因として,医師の 出血性合併症に対する懸念などが指摘されている.本 研究においても,“off-label" under-dose 群は,有意に 高齢でクレアチニンクリアランスは低値であった.高 齢かつ,正常下限程度の腎機能の患者は,非高齢者 と比較すると見た目の弱々しさ(フレイルティ)が 目立ち,処方医が『出血リスクが高そうな患者』と 考え,出血リスク軽減のために敢えて減量して投与 するといった判断が,“off-label" under-dose 投与に大 きくかかわっているのではないかと考える.実際に RAMSES study7)では,65 歳以上の高齢者が “off-label" under-dose投与の独立した因子であった.本研究の 結果から,医師の判断がかえって塞栓症や心血管死の 複合イベントを増加させていることが示唆され,注 意喚起が必要である.本研究の結果は,SAKURA AF Registry3)の “off-label" under-dose 投与と心血管イベ ント発症に有意な関係はないとの報告とは異なる結果 であった.これには患者背景・DOAC の種類・主要 評価項目の違いなどの関与が考察されるが,今後さら なる検討が必要である. また今回,処方時の心拍数が複合心血管イベント発 症の独立した予測因子であった.洞調律では,心拍数 が心血管イベント発症の予測因子であることはすでに 報告されているが,心房細動患者では心拍数と心血管 Fig. 1 Kaplan-Meier estimates of cumulative cardiovascular events-free survival in atrial
fibrillation patients with “off-label” under-dosing compared with standard dosing of rivaroxaban.
イベント発症については明確なデータは得られていな い8).本研究は処方時の調律が混在しているため,今 後調律を揃えた検討を要すると考える. "off-label" under-dose 投与と出血イベント 本研究では,抗血小板剤内服が単変量解析にて出血 イベントの有意な因子であった.これは以前の報告9)と 合致するものである.しかし,“off-label" under-dose 投与は出血イベントの有意な因子とはならず,多変量 解析でも出血抑制の効果を確認できなかった. 以上の結果から,DOAC のリバーロキサバン処方 にあたって,腎機能が保持されている場合,大規模臨 床研究が示した有効性と安全性が確認されている添付 文書に従った適切な処方を行うことが必要であり,出 血リスクが高いと判断する場合には減量投与可能な薬 剤への変更を検討すべきである. 本研究の限界 本調査の限界は,1) 単施設の比較的短期間での研 究であること,2) 研究デザイン上,抗凝固薬以外の 薬剤によるイベント発症への関与が不明であることが 挙げられる. 結 論 非弁膜症性心房細動患者に対し,DOAC を開始す る際には,添付文書に従った用量調整基準を遵守する ことが肝要である. 利益相反:本研究において開示すべき COI はあり ません.
No hemorrhage Hemorrhage P value
(N = 278) (N = 22)
Age (years) 68 ± 10 69 ± 12 0.77
Male gender 196 (71) 17 (77) 0.53
Height (cm) 163 ± 9 165 ± 8 0.64
Body weight (kg) 64 ± 12 67 ± 12 0.19
Body mass index (kg/m2) 24 ± 4 25 ± 4 0.30
Systolic blood pressure (mmHg) 130 ± 22 131 ± 23 0.99
Diastolic blood pressure (mmHg) 81 ± 15 80 ± 17 0.56
Heart rate (beats/min) 86 ± 22 80 ± 21 0.29
Creatinine (mg/dl) 0.80 ± 0.19 0.80 ± 0.19 0.70
Creatinine clearance (ml/min) 79 ± 23 82 ± 25 0.18
Paroxysmal atrial fibrillation 149 (54) 13 (59) 0.47
CHADS2 score 1.7± 1.3 1.5 ± 1.1 0.28
HAS-BLED score 1.3± 0.8 1.4 ± 1.0 0.77
Anemia 49 (18) 5 (23) 0.59
Hypertension 162 (58) 13 (59) 0.99
Diabetes mellitus 73 (26) 5 (23) 0.79
History of heart failure 64 (23) 2 (9) 0.29
History of cerebral infarction 56 (20) 3 (14) 0.34
“Off-label” under-dose 60 (22) 5 (23) 0.92
Combined antiplatelet therapy 0 (0) 4 (18) < 0.001
Table 3 Univariable model for prediction of hemorrhage event in AF patients.
ABSTRACT
Real-World Evidence of Adverse Clinical Outcomes in Atrial Fibrillation Patients Newly Initiated on “Off-Label"
Under-dosing of Rivaroxaban
Yoshinobu SUWA, Yoko MIYASAKA, Shoko HARADA, Eri NAKAI, Naoki TANIGUCHI and Ichiro SHIOJIMA
Division of Cardiology, Department of Medicine II, Kansai Medical University
Background: Clinical trials have shown efficacy and safety of direct oral anticoagulants (DOAC) comparable with that of warfarin in preventing stroke in patients with non-valvular atrial fibrillation (AF). However, post-marketing surveillance showed that numerous patients received “off-label" under-dosing of DOAC. Methods: Between 2012 and 2015, consecutive AF patients newly initiated on rivaroxaban with preserved renal function were evaluated and prospectively followed until death or last follow-up. Patients were divided into two groups; taking rivaroxaban 15 mg (standard dose) and 10 mg (“of f-label" under-dose). Primar y outcome was cardiovascular events (embolic events or car-diovascular death) and secondar y outcome was hemorrhage. Cox propor tional hazards modeling was used to assess independent risk factors for events. Results: Of 300 non-valvular AF patients (68± 10 years old, 22 % “off-label" under-dose), 13 (4.3% ) had cardiovascular events and 22 (7% ) had hemorrhagic events during mean follow-up of 13± 11 months. In the multivariable Cox proportional hazards model, “off-label" under-dosing of rivaroxaban carried significant independent risk of cardiovascular events but not hemorrhagic events. Conclusion: In non-valvular AF with preserved renal function, “off-label" under-dosing of rivaroxaban carries increased risk of cardiovascular events, but do not prevent hemor-rhagic events.
文 献
1) Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz MD, Camm AJ, Weitz JI, Lewis BS, Parkhomenko A, Yamashita T, Antman EM: Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fi-brillation: a meta-analysis of randomized trials. Lancet 2014, 383: 955962
2) Miller CS, Grandi SM, Shimony A, Filion KB, Eisen-berg MJ: Meta-analysis of efficacy and safety of new oral anticoagulants (dabigatran, rivaroxaban, apixa-ban) versus warfarin in patients with atrial fibrillation.
Am J Cardial 2012, 110: 453460
3) Murata N, Okumura Y, Yokoyama K, Matsumoto N, Tachibana E, Kuronuma K, Oiwa K, Matsumoto M, Kojima T, Hanada S, Nomoto K, Arima K, Takahashi F, Kotani T, Ikeya Y, Fukushima S, Itoh S, Kondo K, Chiku M, Ohno Y, Onikura M, Hirayama A: Clinical outcomes of off-label dosing of direct oral anticoagu-lant therapy among Japanese patients with atrial fibril-lation identified from the SAKURA AF Registry. Circ
J 2019, 83: 727735
4) Means RT: Disorders of red cells. Greer JP eds. Win-trobe's Clinical Hematology, Thirteenth Edition, Lip-pincott Williams & Wilkins, Philadelphia, 2014, pp 5871042.
5) McKee PA, Castelli WP, McNamara PM, Kannel WB: The natural history of congestive heart failure: the Framingham study. N Engl J Med 1971, 285: 1441
1446
6) Schulman S, Kearon C: Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost 2005, 3: 692694
7) Basaran Ö, Dagon V, Beton O, Tekinalp M, Aykan AC, Kalaycioglu E, Bolat I, Tasar O, Safak Ö, Kalcik M, Yaman M, Inci S, Altintas B, Kalkan S, Kirma C, Bi-teker M: Suboptimal use of non-vitamin K antagonist oral anticoagulants; Results from the RAMSES study.
Medicine 2016, 95: 35 (e4672)
8) Van Gelder IC, Groenveld HF, Crijns HJ, Tuininga YS, Tijssen JG, Alings AM, Hillege HL, Bergsma-Kadijk JA, Cornel JH, Kamp O, Tukkie R, Bosker HA, Van Veldhuisen DJ, Van den Berg MP; RACE II Investiga-tors: Lenient versus strictrate control in patients with atrial fibrillation. N Engl J Med 2010, 362: 13631373
9) Sotomi Y, Hirata A, Amiya R, Kobayashi T, Hirayama A, Sakata Y, Higuchi Y: Bleeding risk of add-on anti-platelet agents to direct oral anticoagulants in pa-tients with nonvalvular atrial fibrillation (From 2216 patients in the DIRECT Registry). Am J Cardiol 2019,