【症例】多発外傷を合併した胸部大動脈急性解離に対してステントグラフト内挿術と開胸止血術を施行した 1 例
4
0
0
全文
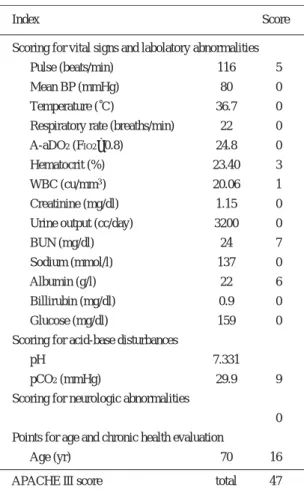
(2) 12. 日血外会誌 15巻 1 号 Table 1 APACHE III score. レベルに存在すると考え,この範囲をステントグラフ ト (SG) で被覆することとした. MDCTで測定したとこ. Index. ろ,同部位の大動脈径はTh5の高さで35mm,Th12で. Score. SMA Scoring for vital signs and labolatory abnormalities. 27mmであり,Th5上縁からTh12下縁にかけての大動脈長 は210mmであった.UBE thin wall graft ®とZ-ステント® で38mm × 130mmと30mm × 130mmの 2 つのSGを作成. Pulse (beats/min). 116. 5. Mean BP (mmHg). 80. 0. Temperature (˚C). 36.7. 0. 22. 0 0. し,これらをオーバーラップさせて被覆大動脈長を調. Respiratory rate (breaths/min). 節できるようにした.外腸骨動脈の蛇行が著しかった. A-aDO2 (FIO2 =0.8). 24.8. ため,約 5cmの傍腹直筋切開から後腹膜経路で右外腸. Hematocrit (%). 23.40. 3. 骨動脈を露出し,TPEGのアプローチとした.22Frのデ. WBC (cu/mm3 ). 20.06. 1. リバリーシステムを用いて,Th5上縁から,Th12下縁に. Creatinine (mg/dl). 1.15. 0. 存在する腹腔動脈起始部の直上までSGを一部重複させ. Urine output (cc/day). て留置した. TPEG終了 4 時間後より循環動態が不安定となり,胸 部単純レントゲン写真にて右側血胸の進行を認めた. 胸腔穿刺で多量の血液が確認されたため,TPEG施行 6 時間後に開胸手術を施行した.広範囲に椎体骨折によ. 3200. 0. BUN (mg/dl). 24. 7. Sodium (mmol/l). 137. 0. Albumin (g/l). 22. 6. Billirubin (mg/dl). 0.9. 0. Glucose (mg/dl). 159. 0. Scoring for acid-base disturbances. る胸膜下血腫があり,壁側胸膜の損傷部位から静脈性 出血を認めた.肺実質からの出血は認めなかった.電. pH. 7.331. pCO2 (mmHg). 29.9. 9. Scoring for neurologic abnormalities. 気メスによる凝固とシート状組織接着閉鎖剤 (タココン. 0. ブ ®)による圧迫で止血しえた. Points for age and chronic health evaluation. 術後経過は良好で,第 6 病日で人工呼吸器より離脱. Age (yr). し,第44病日に退院となった.術後のCT (Fig. 2) では解. APACHE III score. 離腔は閉鎖され,腹腔動脈の血流も維持されており,. 70. 16. total. 47. 両側血胸も軽快し,消失した.くも膜下出血は保存的 治療で軽快し,対麻痺は発生しなかった. な外科的修復が推奨されている10).急性期手術の成績. 考 察. が悪いのは,外傷性大動脈損傷の 3 割以上の症例が頭. 鈍的外力による胸部大動脈損傷の好発部位は大動脈峡. 部外傷等の他部位の出血性損傷を合併しており11),従. 部,上行大動脈,弓部大動脈の順と報告されている7).. 来術式に不可欠な抗凝固薬による出血の助長が一因で. 大動脈損傷が多く発生する機序として次の 2 つが考え. あると考えられている.TPEGは従来の術式と比較して. られている.ひとつは胸部の水平方向の急激な衝撃に. 抗凝固薬の投与量が少なく12),呼吸器合併症の原因と. 際し,心臓,上行大動脈,弓部大動脈,動脈管索,お. なる左側開胸操作や補助循環装置が不要である.本症. よび胸部下行大動脈との間に位置のずれが生じること. 例の右側血胸に対しては追加の止血術が必要であった. による外傷の発生である7).これに対して,胸部を下か. ものの,外傷性くも膜下出血が悪化することなく経過. ら突き上げられて生じる垂直方向の力が加えられた場. したため,多発外傷を合併した大動脈解離に対して. 合には大動脈峡部小彎側が過伸展され断裂するとい. TPEGは有用な手段であると思われた.. う,いわゆるshovel mechanismも考察されている7).今回. 外傷性大動脈解離に対するTPEGの成績を向上させる. の症例は落下して材木の下敷きになったことから,こ. ためには,解離範囲や主要分枝の位置,多発外傷や臓. の両者が複合して発生した大動脈損傷と考えられた.. 器虚血の有無を迅速に診断し,SG留置部位の血管径と. 8, 9). ,報告. 長さを正確に評価することが必要である.MDCTは従. されているガイドラインにおいても診断確定後は迅速. 来のCTと比較して,胸腹部大動脈の広範囲を短時間で. 外傷性大動脈損傷の自然予後は非常に悪く. 12.
(3) 2006年 2 月. 相良ほか:急性外傷性胸部大動脈解離に対するTPEG. 13. celiac artery. Fig. 1. Sagittal reconstruction of multidetector-row computed tomography. Arrow indicates acute aortic dissection (DeBakey IIIb).. Fig. 2. Postoperative three-dimensional reconstruction of computed tomography. Endovascular graft covered the thoracic aortic injury. Arrow indicates the celiac artery.. 撮影でき,三次元画像上の正確な距離の計測が可能で. 結 語. ある13, 14).今回の症例ではMDCTにより多発外傷を伴う 急性大動脈解離を迅速に診断することができただけで. 多発外傷を合併した急性外傷性大動脈解離におい. なく,術前に綿密なSGの設計が可能であった.しかし. て,MDCTは迅速な全身精査とTPEGの術前計画に有効. ながらMDCTで計測したSG予測留置長でも,SGが実際. であった.TPEGは多発外傷からの出血を助長させるこ. に留置される長さとは誤差が生じる.本症例において. となく大動脈損傷部位を被覆することができる,低侵. は,末梢側のSGが腹腔動脈起始部を被覆しないよう. 襲な治療法であると考えられた.. に,作製した 2 つのSGによって被覆する大動脈長を調 節した.今後は術前にデバイスの長さを可能な限り正. 文 献. 確に把握する方法のみでなく,今回自作したような. 1) Creasy, J. D., Chiles, C., Routh, W. D., et al.: Overview of. modular typeのSGで術中にも長さを調節しうる工夫や,. traumatic injury of the thoracic aorta. Radiographics, 17:. 患者の大動脈の三次元形態を考慮したSGを作成するな. 27-45, 1997.. どの方法が必要であると思われた.. 2) Turney, S. Z., Attar, S., Ayella, R., et al.: Traumatic rupture. 広範囲のTPEGは人工血管置換術の場合と同様に,脊. of the aorta: A five-year experience. J. Thorac. Cardiovasc.. 髄虚血による対麻痺の発生が危惧される15, 16).人工血管. Surg., 72: 727-734, 1976.. 置換術による対麻痺は術直後あるいは術後数週間の早. 3) Mattox, K. L., Holzman, M., Pickard, L. R., et al.: Clamp/. 期に徴候が現れ,TPEGによる対麻痺は遅発性に発生す. repair: A safe technique for treatment of blunt injury to the descending thoracic aorta. Ann. Thorac. Surg., 40: 456-. 17). るとされている .またTPEGによる対麻痺の発生率は. 463, 1985.. 3%とされており,外科手術の 5∼15% 18)に比し有意に. 4) Verdant, A., Pagé, A., Cossette, R., et al.: Surgery of. 低率であると報告されている19).本症例において急性. descending thoracic aorta: Spinal cord protection with Gott. 期の対麻痺は認めなかったが,今後も引き続き対麻痺. shunt. Ann. Thorac. Surg., 46: 147-154, 1988.. に対する注意が必要であるものと考えられる.. 5) Turney, S. Z.: Blunt trauma of the thoracic aorta and its branches. Semin. Thorac. Cardiovasc. Surg., 4: 209-216, 1992. 6) Knaus, W. A., Wagner, D. P., Draper, E. A., et al.: The. 13.
(4) 14. 日血外会誌 15巻 1 号 のMDCT診断.臨放,48:1639-1645,2003.. APACHE III prongostic system: Risk prediction of hospital. 14) Velazquez, O. C., Woo, E. Y., Carpenter, J. P., et al.: De-. mortality for critically ill hospitalized adults. Chest, 100: 1619-1636, 1991.. creased use of iliac extensions and reduced graft junctions. 7) Besson, A. and Saegesser, F.: A Colour Atlas of Chest Trauma. with software-assisted centerline measurements in selection. and Associated Injuries, Vol. II, London, 1982, Wolfe Med.. of endograft components for endovascular aneurysm repair. J. Vasc. Surg., 40: 222-227, 2004.. Publ., pp. 136-151. 8) Parmley, L. F., Mattingly, T. W., Manion, W. C., et al:. 15) Tiesenhausen, K., Amann, W., Koch, G., et al.: Cerebrospinal. Nonpenetrating traumatic injury of the aorta. Circulation,. fluid drainage to reverse paraplegia after endovascular thoracic aortic aneurysm repair. J. Endovasc. Ther., 7: 132-135, 2000.. 17: 1086-1101, 1958. 9) Finkelmeier, B. A., Mentzer, R. M., Kaiser, D. L., et al.:. 16) Greenberg, R., Resch, T., Nyman, U., et al.: Endovascular. Chronic traumatic thoracic aneurysm. Influence of operative. repair of descending thoracic aortic aneurysm: An early. treatment on natural history: An analysis of reported cases,. experience with intermediate-term follow-up. J. Vasc. Surg., 31: 147-156, 2000.. 1950-1980. J. Thorac. Cardiovasc. Surg., 84: 257- 266, 1982. 10) Nagy, K., Fabian, T., Rodman, G., et al.: Guidelines for the. 17) Carroccio, A., Marin, M. L., Ellozy, S., et al.: Pathophysi-. diagnosis and management of blunt aortic injury. An EAST. ology of paraplegia following endovascular thoracic aortic. Practice Management Guidelines Work Group. J. Trauma,. aneurysm repair. J. Card. Surg., 18: 359-366, 2003. 18) Coselli, J. S., LeMaire, S. A., Figueiredo, L. P., et al.: Paraple-. 48: 1128-1143, 2000.. gia after thoracoabdominal aortic aneurysm repair: Is dis-. 11) Smith, R. S. and Chang, F. C.: Traumatic rupture of the aorta: Still a lethal injury. Am. J. Surg., 152: 660-663, 1986.. section a risk factor ? Ann. Thorac. Surg., 63: 28-36, 1997.. 12) Rousseau, H., Soula, P., Perreault, P., et al.: Delayed treatment. 19) Rodrigues Alves, C. M., da Fonseca, J. H., de Souza, J. A.,. of traumatic rupture of the thoracic aorta with endoluminal. et al.: Endovascular treatment of thoracic disease: Patient. covered stent. Circulation, 99: 498-504, 1999.. selection and a proposal of a risk score. Ann. Thorac. Surg.,. 13) 小林泰之,船窪正勝,濱田健司,他:大血管疾患領域. 73: 1143-1148, 2002.. A Case of Transluminally Placed Endovascular Grafting for Acute Thoracic Aortic Dissection with Multiple Trauma Daisuke Sagara, Hiroshi Mitsuoka, Naoki Unno, Kazunori Inuzuka and Kei Ishimaru Second Department of Surgery, Hamamatsu University School of Medicine Key words: Aortic injury, Stent-graft, Multidetector-row CT, Anticoagulant. A 70-year-old man was transferred to our hospital with unstable vital signs and an APACHE III score of 47. Multidetector-row computed tomography (MDCT) detected acute aortic dissection, accompanied with bilateral hemothorax, thoracic vertebral fracture, and subarachnoid hemorrhage. The aortic dissection was immediately treated by transluminally placed endovascular grafting (TPEG), which covered the level Th-5 to -12 of the thoracic aorta. Right thoracotomy was made to coagulate the pleural bleeding due to the vertebral fracture, which aggravated the right hemothorax even after TPEG. The postoperative course was uneventful and there was no paraplegia. The patient was discharged on the 44th postoperative day. Postoperative computed tomography confirmed disappearance of the subarachnoid hemorrhage and the hemothorax, and successful placement of the stent-graft with spared patency of the celiac artery. Not only was it feasible for the whole body examination for other trauma, MDCT enabled precise preoperative planning for the emergency TPEG. Since blunt aortic injury is frequently accompanied by multiple trauma, TPEG could treat the complicated conditions less invasively, with a minimal amount of preprocedural anticoagulant for the aortic surgery, and with a reduced volume of blood loss. 14. (Jpn. J. Vasc. Surg., 15: 11-14, 2006).
(5)
図

関連したドキュメント
Quantitative Analysis of Respiratory Kinetics in Breathing Chest Radiographs Obtained Using a Dynamic Flat-Panel Detector Rie TANAKA, Shigeru SANADA, Masayuki SUZUKI, Takeshi
本症例における IL 6 および IL 18 の動態につい て評価したところ,病初期に IL 6 は s JIA/ inac- tive より高値を示し,敗血症合併時には IL
4 Hopwood JJ, Elliott H: Detection of Morquio A Syndrome using radiolabelled substrates derived from keatan sulphate for the estimation of galactose 6- sulphate sulphatase.. 6 Doman
PHA-P; Phytohemagglutinin-P Con A;Concanavalin A PWM ;Pokeweed mitogen PPD ;purified protein derivative NWSM ;Nocardia water-soluble mitogen.. 免疫系 の中枢器 官であ
幽幽には12例が含まれている.このうち,閉胸式 massage(CCCM)ないし前胸壁叩打を施行したも
にて優れることが報告された 5, 6) .しかし,同症例の中 でも巨脾症例になると PLS は HALS と比較して有意に
信心辮口無窄症一〇例・心筋磁性一〇例・血管疾患︵狡心症ノ有無二關セズ︶四例︒動脈瘤︵胸部動脈︶一例︒腎臓疾患
今回completionpneumonectomyを施行したが,再
