進行再発非小細胞肺癌に対する セカンドライン化学療法の検討
昭和大学医学部内科学講座(呼吸器アレルギー内科学部門)
白井 崇生 廣 瀬 敬 村田 泰規 大木 康成 楠本壮二郎 杉山 智英 石田 博雄 中嶌 賢尚 大 西 司
昭和大学腫瘍分子生物学研究所
山岡 利光 大 森 亨
昭和大学歯科病院総合内科
奥田健太郎
要約:進行再発非小細胞肺癌に対するセカンドライン化学療法の有効性を治療薬剤別に比較検 討することを目的とした.1998 年から 2006 年までに当院にて,初回化学療法としてプラチナ 併用化学療法を施行後,再発した非小細胞肺癌患者 253 例のうち,セカンドライン化学療法を 受けた 76 例を対象とした.セカンドライン化学療法の治療効果について,ドセタキセル単剤 あるいはその併用療法群,ゲフィチニブ群,その他の治療群に分け,奏効率,生存期間,無増 悪生存期間を後ろ向きに検討した.患者背景は,年齢中央値 63 歳(39 〜 80 歳),女性 24 例
(31.6%),performance status(PS)0 〜 1 が 61 例(80.3%),組織型は腺癌 57 例(75.0%),
非喫煙者 17 例(22.4%)であった.セカンドライン化学療法で使用した薬剤は,ドセタキセ ル単剤あるいはその併用療法 51 例,ゲフィチニブ 15 例,その他の治療 10 例であった.ドセ タキセル,ゲフィチニブ,その他の治療の奏効率,生存期間中央値,無増悪生存期間中央値 は,6.1% / 20% / 20%,9.6 か月 / 4.2 か月 / 23 か月,2.3 か月 / 2.3 か月 / 1.7 か月で,いずれも 有意差を認めなかった.患者背景では,PS が再発後の予後と関連した.進行再発非小細胞肺 癌に対するセカンドライン化学療法の有効性は,ドセタキセル単剤あるいはその併用療法,ゲ フィチニブ,その他の治療薬剤で同等であった.
キーワード:再発,非小細胞肺癌,セカンドライン化学療法,ドセタキセル,ゲフィチニブ
進行非小細胞肺癌に対する初回化学療法の標準治 療は,プラチナ製剤を含む 2 剤併用療法±ベバシ ズマブである1).しかし,ほとんどの症例は,初回 化学療法後に再発し,セカンドライン化学療法の適 応となる.
進行非小細胞肺癌を対象とし,初回化学療法の有 効性を比較するために 1996 年〜 1999 年に Eastern Clinical Oncology Group で施行された第 III 相試験 では,プラチナ併用療法の中間生存期間は 7.4 〜 8.2 か月であった2).しかし,同グループで 2001 年〜
2004 年に施行された第 III 相試験では,プラチナ併 用療法の中間生存期間は 10.3 か月に延長した1).予
後が延長した理由として,再発後の治療の進歩が一 因と考えられる.
2000 年以前は,進行再発非小細胞肺癌に対する 標 準 治 療 は 存 在 せ ず, 主 に best supportive care
(BSC)で治療されていたが,その予後は 4 〜 5 か 月と極めて不良であった.2000 年に進行再発非小 細胞肺癌に対し,ドセタキセルが BSC よりも予後 を延長することが報告され3,4),さらに,ペメトレ キセド,上皮成長因子受容体チロシンキナーゼ阻害 剤(epidermal growth factor receptor tyrosin kinase inhibitor : EGFR-TKI)のゲフィチニブやエルロチ ニブの有効性が報告されて標準治療と位置付けられ 原 著
446
p446白井崇生0225.indd 446
p446白井崇生0225.indd 446 2013/03/01 15:44:552013/03/01 15:44:55
447 た5‑7).EGFR-TKI は,EGFR 遺伝子変異陽性例に 有効性が高いが8,9),EGFR 遺伝子変異陰性例では 有効性が低い10).したがって,現在,EGFR 遺伝子 変異陽性例では EGFR-TKI を選択し,EGFR 遺伝 子変異陰性例や不明例ではドセタキセルやペメトレ キセドを選択する.
しかし,EGFR 遺伝子変異検査が本邦で測定可能 となったのは 2007 年で,それ以前は EGFR 遺伝子 変異に拘らず薬剤を選択していた.IPASS 試験で は遺伝子変異不明例が 60%以上含まれていた10). さらに,現在の日常臨床においても 22 〜 25%の患 者では EGFR 遺伝子変異不明例であると報告され
ている11,12).再発非小細胞肺癌における EGFR 遺
伝子不明患者の治療方針を決める上で,EGFR 遺伝 子変異が測定できなかった時の再発後の治療薬別の 効果,生存期間を比較検討することが参考になり,
意義があることだと考え,本検討を行った.
研 究 方 法
1998 年から 2006 年までに進行非小細胞肺癌と診 断され,当院で初回化学療法としてプラチナ併用化 学療法を施行後に再発した 253 例のうち,セカンド ライン化学療法を受けた 76 例(30.0%)を対象と した.ドセタキセル単剤あるいは併用療法群(D 群),ゲフィチニブ群(G 群),その他の治療群(O 群)に分け,セカンドライン化学療法の治療効果に ついて後ろ向きに検討した.また,患者背景では,
年 齢, 性 別,performance status(PS), 組 織 型,
喫煙歴,初回時病期,再発時病期,初回治療の効果 により,生存期間や無増悪生存期間に差があるか解 析した.初回化学療法,セカンドライン化学療法と もに,治療薬剤の選択は主治医の判断で決定され た.なお,本後ろ向き解析は,昭和大学医学部倫理 委員会の承認を得た.
再発とは,初回治療不応,部分寛解後の再燃,完 全寛解後の再出現,新病変の出現の全てを含むと定 義した.生存期間は,治療開始日から死亡日までと し,追跡不可能例については,治療開始日から最後 に生存が確認された日とした.無増悪生存期間は,
治療開始日から再発や増悪・死亡が確認された日ま でとした.有意差検定は,2 群間の比較にはχ2検 定を使用した.生存曲線は Kaplan-Meier 法を用い,
log-rank test で検定した.
結 果
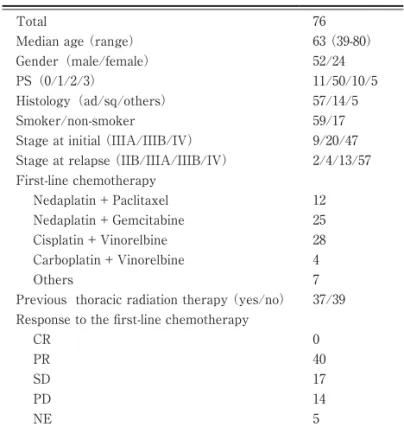
セカンドライン化学療法開始時の患者背景を Table 1 に示す.年齢中央値は 63 歳(39 〜 80 歳),
女 性 24 例(31.6 %),PS 0 〜 1 が 61 例(80.3 %),
組 織 型 は 腺 癌 が 57 例(75.0 %), 非 喫 煙 者 17 例
(22.4%)であった.初回化学療法の奏効率は 56.3%
で,初回化学療法終了後から再発までの期間の中央 値は 3.4 か月であった.
セカンドライン化学療法の治療薬剤別の患者背景 を Table 2 に示す.D 群が 51 例(67.1%),G 群が 15 例(19.7 %),O 群 が 10 例(13.2 %) で あ っ た.
O 群のうち 5 例は,初回化学療法の再投与であっ た.D 群と比較し,G 群では女性,腺癌,非喫煙者 が有意に多かった.3 次治療は,D 群 33 例(64%),
G 群 6 例(40%),O 群 7 例(70%)で受けていた が統計学的有意差を認めなかった(P = 0.087:G 群,P = 0.747:O 群).3 次治療の奏効率は,D 群 が 12%(4/33),G 群が 16%(1/6),O 群が 14%
(1/7)であったが統計学有意差を認めなかった
(P = 0.75:G 群,P = 0.87:O 群).初回化学療法 の奏効率は,D 群 62.5%,G 群 21.4%,O 群 77.8%
で,G 群で有意に低かった.3 次治療として,D 群 では 23 例(45%)がゲフィチニブによる治療を受 け,G 群では 6 例(40%)がドセタキセルによる治 療を受けた.
セカンドライン化学療法の奏効率は,全例では 10.5%で,治療薬剤別では D 群 5.9%,G 群,O 群 がそれぞれ 20%であった.D 群で奏効率が低い傾 向 で あ っ た が, 統 計 学 的 有 意 差 を 認 め な か っ た
(P = 0.09:G 群,P = 0.14:O 群).病状制御率は,
全例では 59.2%で,治療薬剤別では D 群が 58.8%,
G 群,O 群がそれぞれ 60%で,統計学的有意差を 認 め な か っ た(P = 0.94:G 群,P = 0.94:O 群 )
(Table 3).
セカンドライン化学療法後の中間生存期間は,全 例では 9.0 か月で,治療薬剤別では,D 群 9.6 か月,
G 群 4.2 か月,O 群 23 か月で,O 群で長い傾向であっ たが,統計学的有意差を認めなかった(P = 0.071)
(Fig. 1).中間無増悪生存期間は,全例では 2.3 か 月で,治療薬剤別では D 群 2.3 か月,G 群 2.3 か月,
O 群 1.7 か月で,統計学的有意差を認めなかった
(P = 0.493)(Fig. 2).
p446白井崇生0225.indd 447
p446白井崇生0225.indd 447 2013/03/01 15:45:052013/03/01 15:45:05
448
Table 1 Patient characteristics
Total 76
Median age (range) 63 (39-80)
Gender(male/female) 52/24
PS(0/1/2/3) 11/50/10/5
Histology(ad/sq/others) 57/14/5
Smoker/non-smoker 59/17
Stage at initial (IIIA/IIIB/IV) 9/20/47 Stage at relapse (IIB/IIIA/IIIB/IV) 2/4/13/57 First-line chemotherapy
Nedaplatin + Paclitaxel 12
Nedaplatin + Gemcitabine 25
Cisplatin + Vinorelbine 28
Carboplatin + Vinorelbine 4
Others 7
Previous thoracic radiation therapy (yes/no) 37/39 Response to the fi rst-line chemotherapy
CR 0
PR 40
SD 17
PD 14
NE 5
Table 2 Patients characteristics according to the chemotherapy regimen D group G group
P value O group
P value
(n = 51) (n = 15) (n = 10)
Age (70 ≧ /70 <) 11/40 6/9 0.15 1/9 0.40
Gender(male/female) 40/11 7/8 0.02 5/5 0.06
PS(0/1/2/3) 6/34/9/2 1/10/1/3 0.68 4/6/0/0 0.11
Pathology(ad/sq/others) 36/12/3 15/0/0 0.02 6/2/2 0.51
Smoker/non-smoker 45/6 8/7 0.003 6/4 0.03
Stage at initial (IIIA/IIIB/IV) 7/12/32 0/5/10 0.80 2/3/5 0.66
Stage at relapse (IIB/IIIA/IIIB/IV) 0/3/9/39 0/0/4/11 0.06 2/1/0/7 0.66 Response rate to the fi rst-line chemotherapy (%) 62.5 21.4 0.01 77.8 0.38
3rd line chemotherapy (yes/no) 33/18 6/9 0.08 7/3 0.74
D group : Docetaxel single agent therapy or doublet therapy G group : Gefi tinib O group : Other therapy
Table 3 Response rate
D group G group O group Total
(n = 51) (n = 15) (n = 10) (n = 76)
Number (%) Number (%) Number (%) Number (%)
Complete response 0 (0) 0 (0) 0 (0) 0 (0)
Partial response 3 (5.9) 3 (20.0) 2 (20.0) 8 (10.5)
Stable disease 27 (52.9) 6 (40.0) 4 (40.0) 37 (48.7)
Progressive disease 19 (37.2) 4 (26.7) 4 (40.0) 27 (35.5)
Not evaluable 2 (3.9) 2 (13.3) 0 (0) 4 (5.3)
D group : Docetaxel single agent therapy or doublet therapy G group : Gefi tinib O group : Other therapy
p446白井崇生0225.indd 448
p446白井崇生0225.indd 448 2013/03/01 15:45:072013/03/01 15:45:07
449 患 者 背 景 に よ る 生 存 期 間, 無 増 悪 生 存 期 間 を Table 4 に示す.中間生存期間,中間無増悪生存期 間ともに,PS 良好な症例で有意に延長した.
考 察
EGFR 遺伝子変異に拘らずセカンドライン化学療 Fig. 1 shows overall survival from the second-line che-
motherapy estimated with the Kaplan-Meier method. The median survival time (MST) was 9.6 months in group D, 4.2 months in group G, and 23.0 months in group O, respectively.
Fig. 2 shows progression-free survival (PFS) time es- timated with the Kaplan-Meier method. The median PFS time was 2.3 months in group D, 2.3 months in group G, and 1.7 months in group O, respectively.
Table 4 Univariate analysis for overall survival and progression-free survival MST P value median P value Age
≧ 70 4.2 0.21 2.5 0.84
< 70 10.1 1.9
Sex
male 9.0 0.58 2.3 0.97
female 6.8 1.9
Performance status
0 or 1 10.5 <0.01 2.3 0.04
2 or 3 3.8 1.5
Pathology
adenocarcinoma 6.7 0.29 2.3 0.49
non-adenocarcinoma 10.6 1.8
Smoking status
smoker 9.6 0.68 2.3 0.97
never smoker 6.7 2.3
Stage at initial
IIIA or IIIB 6.8 0.25 2.4 0.50
IV 10.5 3.6
Stage at relapse
IIB, IIIA or IIIB 6.8 0.35 2.3 0.36
IV 10.8 4.0
Effi cacy of fi rst-line chemotherapy
CR or PR 7.9 0.50 1.8 0.38
SD or PD 6.8 3.1
p446白井崇生0225.indd 449
p446白井崇生0225.indd 449 2013/03/01 15:45:092013/03/01 15:45:09
450 法の治療薬剤を選択した場合の治療効果について,
治療薬剤別に比較検討した.セカンドライン化学療 法の奏効率,生存期間,無増悪生存期間は,ドセタ キセル単剤あるいはその併用療法,ゲフィチニブ,
その他の治療で,統計学的有意差を認めず同等で あった.O 群の中間生存期間が長い傾向にあったた め,後治療による影響を検討したが,各群の 3 次治 療の頻度,奏効率に有意差を認めなかった.Papat ら13)は,セカンドライン化学療法の治療効果は,
ドセタキセル,ゲフィチニブ,エルロチニブで同等 であったと報告し,われわれの結果と一致してい る.一方,Itaya ら14)は,ゲフィチニブによる治療 が生存期間を延長したと報告しており,われわれの 結果と異なる.再発時においても,EGFR 遺伝子変 異陽性例に対し,EGFR-TKI の奏効率は 70 〜 80%,
中間生存期間は 24 か月で,従来の殺細胞性抗癌剤 の治 療 成 績を上回ることが 報 告され ている15,16). Itaya らの報告は,全例が PS 0 〜 1 で,非喫煙者 の割合が 31%であるのに対し,われわれの検討や Papat らの報告は,PS 3 までを対象とし,非喫煙 者の割合が 10 〜 22%と低いことが,異なった結果 の原因として推察される.
なお,われわれの検討において,全症例での奏効 率,中間生存期間,中間無増悪生存期間は,10.5%,
9.0 か月,2.3 か月で,これまでに報告された大規模 臨床試験での成績の奏効率 6.7 〜 12.6%,中間生存 期間 5.8 〜 9.2 か月,中間無増悪生存期間 2.1 〜 2.9 か月と比較して遜色がなかった3,4,7,17).
本検討において,患者背景で生存期間や無増悪生 存期間と関連したのは,PS のみであった.一方,
Itaya ら14)は,非喫煙者,腺癌では,再発後の予後 が良好であったと報告している.非喫煙者,腺癌,
女性では EGFR 遺伝子変異の陽性率が高いことが 報告されている18).本検討でも,非喫煙者,腺癌,
女性では,ゲフィチニブによる治療を受けた割合が 多かった.しかし,本検討では,67.1%の症例がド セタキセルによる治療を受け,ゲフィチニブによる 治療を受けた症例が少なかったことが,非喫煙者や 腺癌で予後に差を認めなかった一因と考えられる.
現在,3 次治療として推奨されている薬剤はエル ロチニブのみで,殺細胞性抗がん剤が有効であると いうエビデンスはない19).しかし,近年ペメトレ キセドなど非小細胞肺癌に有効な薬剤が数多く開
発され,3 次・4 次治療を受ける患者が増加してい
る20,21).後ろ向きの検討では,3 次・4 次治療によ
り,予後を延長する可能性があると報告されてお
り18,19),今後,3 次・4 次治療の有効性を明らかに
する必要がある.
以上,進行再発非小細胞肺癌に対し,EGFR 遺伝 子変異に拘らずセカンドライン化学療法を選択した 場合,ドセタキセル単剤あるいはその併用療法,ゲ フィチニブ,その他の治療薬剤の有効性は同等で あった.
文 献
1) Sandler A, Gray R, Perry MC, : Paclitaxel- carboplatin alone or with bevacizumab for non- small-cell lung cancer. 355:
2542‑2550, 2006.
2) Schiller JH, Harrington D, Belani CP, : Com- parison of four chemotherapy regimens for ad- vanced non-small-cell lung cancer.
346:92‑98, 2002.
3) Shepherd FA, Dancey J, Ramlau R, : Pro- spective randomized trial of docetaxel versus best supportive care in patients with non-small- cell lung cancer previously treated with plati- num-based chemotherapy. 18:
2095‑2103, 2000.
4) Fossella FV, DeVore R, Kerr RN, : Random- ized phase III trial of docetaxel versus vinorel- bine or ifosfamide in patients with advanced non-small-cell lung cancer previously treated with platinum-containing chemotherapy regi- mens. The TAX 320 Non-Small Cell Lung Can- cer Study Group. 18:2354‑2362, 2000.
5) Kim ES, Hirsh V, Mok T, : Gefi tinib versus docetaxel in previously treated non-small-cell lung cancer (INTEREST): a randomized phase III trial. 372:1809‑1818, 2008.
6) Shepherd FA, Rodrigues PJ, Ciuleanu T, : Erlotinib in previously treated non-small cell lung cancer. 353:123‑132, 2005.
7) Hanna N, Shepherd FA, Fossella FV, : Ran- domized phase III trial of pemetrexed versus docetaxel in patients with non-small-cell lung cancer previously treated with chemotherapy.
22:1589‑1597, 2004.
8) Lynch TJ, Bell DW, Sordella R, : Activating mutations in the epidermal growth factor re- ceptor underlying responsiveness of non-small- cell lung cancer to gefi tinib. 350:
2129‑2139, 2004.
p446白井崇生0225.indd 450
p446白井崇生0225.indd 450 2013/03/01 15:45:112013/03/01 15:45:11
451 9) Paez JG, Janne PA, Lee JC, : EGFR muta-
tions in lung cancer : correlation with clinical re- sponse to gefi tinib therapy. 304:1497‑
1500, 2004.
10) Mok TS, Wu YL, Thongprasert S, : Gefi- tinib or carboplatin-paclitaxel in pulmonary ad- enocarcinoma. 361:947‑957, 2009.
11) 灘波良信,井上貴子,菅野哲平,ほか:日常診 療における非小細胞肺癌 EGFR 遺伝子変異につ いての検討.肺癌 49:662,2009.
12) 山田範幸,朝比奈 肇,大泉聡史,ほか:進行期 非小細胞肺癌の PNA-LNA PCR clamp 法で解析 した EGFR 遺伝子変異の状況と予後との検討.
肺癌 51:460,2011.
13) Popat S, Barbachano Y, Ashley S, : Erlo- tinib, docetaxel, and gefi tinib in sequential co- horts with relapsed non-small cell lung cancer.
59:227‑231, 2008.
14) Itaya T, Yamaoto N, Ando M, : Infl uence of histological type, smoking history and chemo- therapy on survival after first-line therapy in patients with advanced non-small cell lung can- cer. 98:226‑230, 2007.
15) Morita S, Okamoto I, Kobayashi K, : Com- bined survival analysis of prospective clinical trials of gefi tinib for non-small cell lung cancer with EGFR mutations. 15:
4493‑4498, 2009.
16) Rosell R, Moran T, Queralt C, : Screening for epidermal growth factor receptor mutations in lung cancer. 361:958‑967, 2009.
17) Di Maio M, Perrone F, Chiodini P, : Individ- ual patient data meta-analysis of docetaxel ad- ministered once every 3 weeks compared with once every week second-line treatment of ad- vanced non‒small-cell lung cancer.
25:1377‑1382, 2007.
18) Kosaka T, Yatabe Y, Endoh H, : Mutations of the epidermal growth factor receptor gene in lung cancer : biological and clinical implications.
64:8919‑8923, 2004.
19) Azzoli CG, Baker S Jr, Temin S, : American Society of Clinical Oncology Clinical Practice Guideline update on chemotherapy for stage IV non-small-cell lung cancer. 27:
6251‑6266, 2009.
20) Asahina H, Sekine I, Horinouchi H, : Retro- spective analysis of third-line and fourth-line chemotherapy for advanced non-small-cell lung cancer. 13:39‑43, 2012.
21) Girard N, Jacoulet P, Gainet M, : Third-line chemotherapy in advanced non-small cell lung cancer : identifying the candidates for routine practice. 4:1544‑1549, 2009.
p446白井崇生0225.indd 451
p446白井崇生0225.indd 451 2013/03/01 15:45:112013/03/01 15:45:11
452
SECOND-LINE CHEMOTHERAPY IN PATIENTS WITH RELAPSED ADVANCED NON-SMALL LUNG CANCER
Takao SHIRAI, Takashi HIROSE, Yasunori MURATA, Yasunari OKI, Soziro KUSUMOTO, Tomohide SUGIYAMA, Hiroo ISHIDA, Masanao NAKASHIMA and Tsukasa OHNISHI
Division of Respiratory Medicine and Allergology,
Department of Internal Medicine, Showa University School of Medicine
Toshimitsu YAMAOKA and Tohru OHMORI Institute of Molecular Oncology, Showa University School of Medicine
Kentaro OKUDA
Internal Medicine, Showa Dental University
Abstract The aim of this study was to evaluate the response rate, survival time, and progression- free survival (PFS) time of second-line chemotherapy in patients with relapsed advanced non-small cell lung cancer (NSCLC). Between January 1998 and December 2006, of 253 patients with advanced NSCLC who received platinum-based fi rst-line chemotherapy and it recurred, 76 patients who received second- line chemotherapy were retrospectively analyzed. The median time from the fi rst-line chemotherapy to the second-line chemotherapy was 3.4 months. Of these 76 patients, 51 patients received docetaxel-based chemotherapy, 15 patients received gefi tinib, and 10 patients received other chemotherapies. Response rates (RR) for docetaxel-based chemotherapy, gefi tinib, and other chemotherapies were 5.9%, 20%, and 20%, respectively. Median survival times and median PFS times for docetaxel-based chemotherapy, gefi - tinib, and other chemotherapies were 9.6 months and 2.3 months, 4.2 months and 2.3 months, and 23 months and 1.7 months, respectively. There were no signifi cant diff erences in RRs, survival times, and PFS times. Performance status was signifi cantly associated with survival time after recurrence. In con- clusion, three types of chemotherapies showed similar eff ectiveness as second-line chemotherapy in pa- tients with advanced NSCLC.
Key words : relapse, non-small cell lung cancer, second-line chemotherapy, docetaxel, gefi tinib
〔受付:3 月 5 日,受理:3 月 27 日,2012〕
p446白井崇生0225.indd 452
p446白井崇生0225.indd 452 2013/03/01 15:45:112013/03/01 15:45:11