化膿性脳室炎を併発した重症くも膜下出血の一例
8
0
0
全文
(2) Fig. 1 Admission CT (a), CT angiography (CTA: b) and postoperative CTA (c).. a: CT shows subarachnoid hemorrhage with intraventricular hemorrhage and hematoma in the genu of corpus callosum and bilateral frontal lobes. R, right‒ sided. b: CTA shows a left distal anterior cerebral artery aneurysm (maximum diameter, 6.9 mm) with bleb formation. c: Postoperative CTA shows disappearance of the aneurysm.. 現病歴:自宅の浴室で倒れているのを発見され, 術及び脳室ドレナージ術を施行した(Fig. 1c). 近医に救急搬送された.頭部 CT でくも膜下出血. 術後,意識障害の改善はみられず,CT(Fig. 3a). を認め,Japan Coma Scale(JCS)200 の意識障害. では脳梁部の血腫は除去されていたが,脳室内血. を認めたため,気管挿管が行われた後,当院に転. 腫をともなう脳室拡大を依然として認めたため,. 院搬送された.. 脳室ドレナージを外耳口+15 cm に設定し,人工. 入院時現症:気管挿管下であったが自発呼吸を. 呼吸器管理を継続した.第5病日に肺炎を併発し,. 認 め,SpO2 100%(FiO2 : 0.6)で あ っ た.血 圧. sulbactam/ampicillin 6.0 g/日で抗生剤治療を開始. 111/77 mmHg,心拍数 86 回/分,不整.体温 36.2. した.血液培養から Serratia marcescens が検出さ. 度,Glasgow Coma Scale E1VTM1 と意識障害を認. れ,感受性のある meropenem 2.0 g/日に変更した.. めた.瞳孔は正円同大で,対光反射は両側とも迅. 抗生剤変更後も肺炎の改善を認めず,痰培養から. 速,筋緊張に左右差はなかった.. metallo‒b‒lactamase 産 生 Klebsiella pneumoniae も. 入院時画像所見:頭部 CT では,脳梁膝部から. 検出され,感受性のある levofloxacin 500 mg/日を. 両側前頭葉に及ぶ脳内血腫及び脳室内出血を伴う. 第8病日より追加した.これらの抗生剤治療によ. びまん性くも膜下出血(modified Fisher grade 4)と. り肺炎は改善して解熱したが,水頭症は持続した.. 脳室拡大を認めた(Fig. 1a).頭部 CT angiography. ドレナージチューブの度重なる閉塞により第 30. (CTA)では,左遠位部前大脳動脈にブレブを伴. 病日までに髄液ドレナージチューブ(脳室ドレナ. う最大径 6.9 mm の脳動脈瘤(Fig. 1b)を認めた.. ージ及び脊髄ドレナージ)の入れ替えを計7回要. 臨床経過(Fig. 2):血腫の局在と CTA の結果. した.第 30 病日頃より発熱,血中の炎症マーカー. から左遠位部前大脳動脈瘤破裂によるくも膜下出. 及び髄液細胞数の軽度の上昇を認め,髄液培養か. 血(World Federation of Neurological Surgeons grade. ら Corynebacterium striatum が検出されたため,感. 5)と診断し,緊急で開頭脳動脈瘤トラッピング. 受 性 の あ る vancomycin 2.0 g/日 を 開 始 し た.. Neurosurg Emerg Vol. 26, No. 1 2021. 81.
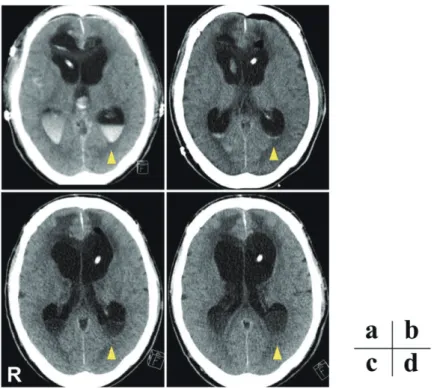
(3) Fig. 2 Chronological CT scans obtained at days 1 (a), 16 (b), 37 (c), and 43 (d) post‒surgery.. Hematoma in the posterior horns of bilateral lateral ventricles decreases from days 1 to 16, but re‒increases as low dense masses from days 37 to 43 (arrowheads). R, right‒sided.. Fig. 3 Clinical courses in the present case.. a: Body temperature. b: Serum levels of C‒reactive protein (CRP). c: Concentrations of white blood cell (WBC) in the peripheral blood. d: The number of WBC per 1 nL of cerebrospinal fluid (CSF). * indicates the operative day of neuroendoscopic evacuation of intraventricular empyema. LVFX, levofloxacin; MEPM, meropenem; SBT/ABPC, sulbactam/ampicillin; VCM, vancomycin.. 82. Neurosurg Emerg Vol. 26, No. 1 2021.
(4) Fig. 4 Follow up diffusion‒weighted magnetic resonance imaging (a) and contrast‒enhanced CT (b).. a: Diffusion‒weighted magnetic resonance images showing high intensity lesions in the posterior horns of bilateral lateral ventricles and frontal lobes at day 40 post‒ surgery. R, right‒sided. b: Contrast‒enhanced CT scans showing near‒ circumferential enhancement of the wall of bilateral lateral ventricles at day 43 post‒surgery. R, right‒sided.. Vancomycin 開始後も髄液細胞数の軽度増加が持. 考 察. 続していた.CT では経時的に両側側脳室後角の 血腫の消退が確認されていた(Fig. 3b)が,第 37. 化膿性脳室炎は,比較的まれな中枢神経系感染. 病日に同部に低吸収の貯留物が認められ(Fig. 3c) , 症であり,髄膜炎の脳室内への進展,脳膿瘍,脳 徐々に増大した(Fig. 3d) .MRI 拡散強調画像では, 神経外科手術などに合併することが知られてい CT で認めた低吸収貯留物は高信号病変として描. る1,3,4).脳室内出血は単独で脳室炎のリスクファ. 出され(Fig. 4),造影 CT で全周性の脳室壁造影. クターになるとの報告はないが,脳室内出血に対. 効果を認めたため(Fig. 5),化膿性脳室炎と診断. する脳神経外科手術が髄液ドレナージ関連脳室炎. し,第 48 病日に内視鏡下脳室内膿瘍除去術及び. のリスクファクターであると報告されている5).. 脳室内灌流(Fig. 6a‒e)を行った.術後,側脳室. また,致死率が 40∼80%に至るとする報告6)や,. 後角の拡散強調画像上の高信号病変は消失した. MRI で脳室炎を認めた 13 例のうち改善例が3例. (Fig. 6f ) .感染所見は改善した.また第 30 病日. のみであったとの報告7)もあり,治療抵抗性で予. から開始した vancomycin は8週間にわたって投. 後不良のことが多い.そのため外科的治療の早期. 与した.膿瘍摘出術後も水頭症管理には難渋し,. 介入を推奨する報告もある8–10).. 連日脳室ドレーンからの髄液排除を行ったが脳室. 化膿性脳室炎は臨床所見が明確でない場合もあ. 拡大は悪化した(Fig. 7a).第 88 病日には脳梁部. り,その診断には画像検査が有用と考えられる.. の残存膿瘍摘出術,第三脳室開窓術も行ったが,. 特に MRI 拡散強調画像が有用とされており11),. 効果はみられず,むしろ第四脳室の孤立性拡大に. 化膿性脳室炎の 95‒100%で拡散強調画像の脳室. よる脳幹の圧迫をきたした(Fig. 7b).全身状態. 内信号異常が認められると報告されている6,12).. 不良及び呼吸障害の悪化により第 94 病日に死亡. 脳室内の化膿性液体貯留は,脳脊髄液中の蛋白や. した.. 壊死組織で構成され,水分子の拡散を制限するた. Neurosurg Emerg Vol. 26, No. 1 2021. 83.
(5) Fig. 5 Neuroendoscopic findings (a‒c) and postoperative diffusion‒ weighted magnetic resonance imaging (d).. a: Removing the capsule of intraventricular empyema with forceps. b: Pus collection is observed in the posterior horns of bilateral lateral ventricles. c: Removing the debris of empyema adhering to the ventricular wall. d: Postoperative diffusion‒weighted image showing the disappearance of empyema in the posterior horns of bilateral lateral ventricles. R, right‒sided.. め,拡散強調画像で高信号となると考えられてい. 髄膜炎の診断は難しく,症状が非特異的である.. る .また CT 所見としては,造影 CT での脳室壁. また脳脊髄液中の白血球数上昇は特異的な情報で. 全周性の造影効果,単純 CT での脳室拡大の進行. はなく,脳脊髄液中の glucose や lactate,グラム. や 脳 室 内 debris を 認 め る こ と が 報 告 さ れ て い. 染色が診断に有用と報告されている2,16).本症例. る11,14).. も脳神経外科手術の術後であったが,脳脊髄液は. 本症例では,単純 CT で脳室内膿瘍を疑う構造. 軽度の細胞数及び蛋白の上昇のみであり所見に乏. 物が増大したことから,頭部 MRI,造影 CT を施. しかった.これは脳室内膿瘍が被膜形成により孤. 行したことで診断に至った.脳室内出血を伴う症. 立化したことにより,髄液細胞数の著明な増加を. 例に長期にわたって脳室ドレナージを施行してい. 伴わなかったためと考えられた.. る場合,脳室内の血腫が培地となって膿瘍を併発. 化膿性脳室炎の治療としては,肺炎球菌などの. する可能性があり,血腫が存在していた部分の変. グラム陽性球菌やグラム陰性桿菌をターゲットし. 化を確認するため,CT ないし MRI でフォローア. た早期の広域スペクトラムの経静脈的抗菌薬によ. ップすることが重要と考えられた.また感染予防. る加療が有効とされており,vancomycin と抗緑膿. を目的として脳室ドレナージを入れ替えるべきか. 菌作用のある b‒lactamase 系(cefepime, ceftazidime,. どうかは controversial である が,脳室ドレナー. meropenem)の併用が推奨されている2).しかし,. ジの長期留置,髄液検査の回数,脳室ドレナージ. 長期間に及ぶ抗菌薬投与による多剤耐性菌の出現,. を繰り返し行うことが脳室炎のリスクファクター. 抗 菌 薬 の 脳 脊 髄 液 移 行 性 の 問 題17)に 加 え,. となるとの報告もあり5,15),本症例のように全身. antibiotic‒resistant biofilm の 形 成 や inflammatory‒. 管理,水頭症管理に難渋する症例ではやむを得な. cell debris による更なる炎症反応の惹起などで病. い部分はあるが,可能な限り早期に髄液ドレナー. 態は複雑となり,治療効果が不十分なことも多い. ジ管理を離脱することが重要と考えられた.. とされている18).. 脳神経外科手術の術後や頭部外傷後の脳室炎や. また経静脈的抗菌薬投与に不応性の難治性脳室. 13). 15). 84. Neurosurg Emerg Vol. 26, No. 1 2021.
(6) Fig. 6 CT scans on the 93th hospital days showing marked enlargement of ventricles. Note that pons is compressed by enlarged forth ventricle. R, right‒sided.. 炎に対して,髄腔内抗菌薬投与の有効性と安全性. の閉塞が起きた非交通性水頭症に加え,くも膜下. を示した報告 もあり,脳室内膿瘍を併発してい. 出血と髄膜炎による脳脊髄液の吸収障害をきたし. る場合は基本的に神経内視鏡などを用いた摘出. た交通性水頭症の両者が混在した病態と考えられ,. 術 が必要と考えられ,髄腔内持続灌流 や抗菌. そのため透明中隔開窓術や第三脳室開窓術を行っ. 薬の髄腔内投与 は摘出術に併せて行ってもよい. ても交通性水頭症の要素が残存し水頭症コントロ. と考えられた.. ールに難渋したと考えられた.本症例で他に有効. 脳室炎に対して神経内視鏡を用いて外科的治療. な可能性があった外科的治療としては,内視鏡的. を行うことにはいくつかのメリットがある.High‒. 脈絡叢焼却術22)や孤立性第四脳室に対する内視鏡. flow irrigation を行うことで脳脊髄液の灌流を活性. 下中脳水道形成術,開頭によるマジャンディー孔. 化 で き,膿 瘍 や 脳 室 壁 に 付 着 す る infection‒. 開窓術23,24)などが挙げられる.これらを行うこと. induced membrane を除去することで,経静脈的ま. で水頭症をコントロールし,脳室炎治癒後に髄液. たは経髄液腔的に投与する抗菌薬の有効性が向上. シャント手術を行い得た場合救命できた可能性が. する可能性がある .また,起因菌同定の可能性. あった.しかし本症例では,重症くも膜下出血に. が増し,細菌学的な診断をつけやすくなり治療の. よる遷延性意識障害と肺炎の併発,長期髄液ドレ. 有用な指標となる. ナージ管理による廃用症候群のために全身状態が. 19). 18). 18). 19). 18). .. 7, 8). また脳室炎やそれに伴う水頭症の治療に際し,. 不良であり,それまでに行ってきた水頭症手術に. 内視鏡下に膿瘍の摘出を行うだけでなく,透明中. よる改善を期待して,これらの侵襲的な追加治療. 隔開窓術や第三脳室開窓術を併せて行うことが有. は行わないという方針であったが,全身状態が許. 効とする報告がある. せばこれらの治療も念頭に置く必要があると考え. .本症例では,抗菌薬治. 20, 21). 療と髄液ドレナージ管理を行ったが,くも膜下出. られた.. 血後及び脳室炎による二次性水頭症のコントロー. 結 語. ルに難渋した.感染及び水頭症のコントロールを 目的に,膿瘍摘出術,infection‒induced membrane. 重症くも膜下出血後に発症した化膿性脳室炎の. の除去,透明中隔開窓術,第三脳室開窓術を行っ. 一例を経験した.化膿性脳室炎は重篤な疾患であ. たが水頭症のコントロールを得ることができず救. り,早期発見および外科的介入を含めた積極的治. 命することはできなかった.本症例は血腫や炎症. 療が重要である.. による中脳水道・マジャンディー孔・ルシュカ孔. Neurosurg Emerg Vol. 26, No. 1 2021. 85.
(7) COI 筆頭演者は日本脳神経外科学会への COI 自己 申告を完了しております.本論文の発表に際して 開示すべき COI はありません.. 文献 1) Bayston R, Hart CA, Barnicoat M, et al: Intraventricular vancomycin in the treatment of ventriculitis associated with cerebrospinal fluid shunting and drainage. J Neurol Neurosurg Psychiatry 50: 1419‒1423, 1987. 2) Tunkel AR, Hasbun R, Bhimraj A, et al: 2017 Infectious Diseases Society of America s Clinical Practice Guidelines for healthcare‒associated ventriculitis and meningitis. Clin Infect Dis 64: e34‒65, 2017. 3) Bakshi R, Kinkel PR, Mechtler LL, et al: Cerebral ventricular empyema associated with severe adult pyogenic meningitis: computed tomography findings. Clin Neurol Neurosurg 99: 252‒255, 1997. 4) Amey RS, Rajesh K, Arivazhagan A: Spontaneous intraventricular rupture of pyogenic brain abscess: a short series of three cases and review of literature. Surg Neurol Int 7: S947‒S951, 2016. 5) Mayhall CG, Archer NH, LambVA, et al: Ventriculostomy‒related infections. A prospective epidemiologic study. N Engl J Med 310: 553‒559, 1984. 6) Fujikawa A, Tsuchiya K, Honya K, et al: Comparison of MRI sequences to detect ventriculitis. AJR Am J Roentgenol 187: 1048‒1053, 2006. 7) Hazany S, Go JL, Law M, et al: Magnetic resonance imaging of infectious meningitis and ventriculitis in adults. Top Magn Reson Imaging 23: 315‒325, 2014. 8) Terada Y, Mineharu Y, Arakawa Y, et al: Effectiveness of neuroendoscopic ventricular irrigation for ventriculitis. Clin Neurol Neurosurg 146: 147‒51, 2016. 9) Wang F, Yao XY, Zou ZR, et al: Management of pyogenic cerebral ventriculitis by neuroendoscopic surgery. World Neurosurg 98: 6‒13, 2017. 10) Qin G, Liang Y, Xu K, et al: Neuroendoscopic lavage for ventriculitis: Case report and literature review. Neurochirurgie 66: 127‒132, 2020. 11) Melanie BF, Robert LW, Sanjay M: CT and MR Imaging Features of Pyogenic Ventriculitis. AJNR Am J Neuroradiol. 22: 1510‒1516, 2001. 12) Pezzullo JA, Tung GA, Mudigonda S, et al: Diffusion‒. 86. weighted MR imaging of pyogenic ventriculitis. AJR Am J Roentogenol 180: 71‒75, 2003. 13) Jae TH, Byung CS, Jae HS, et al: Significance of diffusion‒weighted imaging and apparent diffusion coefficient maps for the evaluation of pyogenic ventriculitis. Clinical Neurol Neurosurg 110(2): 137‒144, 2008. 14) Rohit B, Peter RK, Laszlo LM, et al: Cerebral ventricular empyema associated with severe meningitis: computed tomography findings. Clinical Neurol Neurosurg 99: 252‒255, 1997. 15) Freng S, Kai W, Yueqiao X, et al: Assessment of risk factors for external ventricular drainage‒induced infections in the neurosurgery department. Int J Clin Exp Med 11: 12664‒12669, 2018. 16) Hussein K, Bitterman R, Shofty B, et al: Management of post‒neurosurgical meningitis: narrative review. Clin Microbiol Infect 23: 621‒628, 2017. 17) Wada T, Kuroda K, Yoshida Y, et al: A case of posttraumatic severe ventriculitis treated by intraventricular lavage. No Shinkei Geka 28: 737‒743, 2000. 18) Terada Y, Arakawa Y, Funaki T, et al: Effectiveness of neuroendoscopic ventricular irrigation for ventriculitis. Clinical Neurol Neurosurg 146: 147‒151, 2016. 19) Saad AK, Muhammad W, Usman TS, et al: Intrathecal and intraventricular antibiotics for postoperative Gram‒negative meningitis and ventriculitis. Surg Neurol Int 8: 226, 2017. 20) Chugh A, Husain M, Gupta RK, et al: Surgical outcome of tuberculous meningitis hydrocephalus treated by endoscopic third ventriculostomy: prognostic factors and postoperative neuroimaging for functional assessment of ventriculostomy. J Neurosurg Pediatr 3: 371‒7, 2009. 21) Husain M, Jha DK, Rastogi M, et al: Role of neuroendoscopy in the management of patients with tuberculous meningitis hydrocephalus. Neurosurg Rev 28: 278‒83, 2005. 22) Warf BC: Comparison of endoscopic third ventriculostomy alone and combined with choroid plexus cauterization in infants younger than 1 year of age: a prospective study in 550 African children. J Neurosurg Pediatr 103: 475‒48, 2005. 23) Michael JF, Sven K, Kim HM, et al: Endoscopic Aqueductoplasty and Interventriculostomy for the Treatment of Isolated Fourth Ventricle in Children. Neurosurg 55: 372‒377, 2004. 24) Lena A, Mathias K, Birgit EW, et al: Microsurgical outlet restoration in isolated fourth ventricular hydrocephalusu: a single‒instutional experience. Childs Nerv Syst 28: 2101‒2107, 2012.. Neurosurg Emerg Vol. 26, No. 1 2021.
(8) Abstract. A case of pyogenic ventriculitis after severe subarachnoid hemorrhage Yusuke Kuroda1,2), Masato Shiba1), Tomonori Ichikawa3), Seiji Hatazaki1), Naoki Toma1), and Hidenori Suzuki1) Department of Neurosurgery, Mie University Graduate School of Medicine1) Department of Neurosurgery, Mie Prefectural General Medical Center2) Department of Neurosurgery, Ise Red Cross Hospital3) A man in his 60s was referred to our hospital due to severe (World Federation of Neurological Surgeons grade 5) subarachnoid hemorrhage associated with hematoma in the genu of the corpus callosum and intraventricular hemorrhage due to a ruptured left distal anterior cerebral artery aneurysm. The aneurysm was treated with direct trapping, and external ventricular drainage was performed for acute hydrocephalus. After surgery, the patient required antibiotic therapy for pneumonia and sepsis due to carbapenem‒resistant Enterobacteriaceae. Ventricular drainage catheters were repeatedly replaced for prolonged hydrocephalus. At and after 30 days post‒admission, the patient was diagnosed with meningitis based on increased leukocytes in the cerebrospinal fluid (less than 424/nL). At 40 days post‒admission, diffusion‒weighted magnetic resonance images showed growing high‒intensity masses in the corpus callosum and bilateral lateral ventricles where the hematoma had been, and computed tomography revealed enhancement of the entire wall of ventricles by a contrast medium, leading to a diagnosis of pyogenic ventriculitis. Endoscopic aspiration of isolated and encapsulated empyema was performed and ventricles were irrigated. In spite of repeated ventricular drainage and endoscopic third ventriculostomy, however, the patient died because of uncontrolled hydrocephalus on the 95th hospital day. Considering the high mortality of pyogenic ventriculitis, early diagnosis and treatment are essential, but early diagnosis is sometimes difficult in cases with a limitedly increased number of leukocytes in the cerebrospinal fluid due to isolated and encapsulated intraventricular empyema, as in this case. In cases with prolonged ventricular drainage for hydrocephalus and intraventricular hemorrhage, pyogenic ventriculitis should be kept in mind for early diagnosis based on findings of computed tomography and magnetic resonance imaging. (Received June 30, 2020) (Accepted September 25, 2020) Key words: pyogenic ventriculitis, hydrocephalus, intraventricular empyema, endoscopic aspiration. Neurosurg Emerg Vol. 26, No. 1 2021. 87.
(9)
図


関連したドキュメント
にて優れることが報告された 5, 6) .しかし,同症例の中 でも巨脾症例になると PLS は HALS と比較して有意に
⑫ 亜急性硬化性全脳炎、⑬ ライソゾーム病、⑭ 副腎白質ジストロフィー、⑮ 脊髄 性筋萎縮症、⑯ 球脊髄性筋萎縮症、⑰
These results are motivated by the bounds for real subspaces recently found by Bachoc, Bannai, Coulangeon and Nebe, and the bounds generalize those of Delsarte, Goethals and Seidel
The following result about dim X r−1 when p | r is stated without proof, as it follows from the more general Lemma 4.3 in Section 4..
0.1. Additive Galois modules and especially the ring of integers of local fields are considered from different viewpoints. Leopoldt [L] the ring of integers is studied as a module
When making early preplant surface applications (15 to 45 days prior to planting), use a tank mix of Satellite HydroCap herbicide with other herbicides registered for use in a
As can be seen, the sacred sites associated with Nichiren that are listed in regional chronicles and records of famous places are based on the en- tries found in Shinpen
Zaltus SX, applied as part of a burndown program, may be used for residual weed control, as well as to assist in postemergence burndown of many weeds where field corn will be
