多彩な頭頸部病変を呈した Peptostreptococcus micros による 敗血症性肺塞栓症の 1 例
宮城厚生協会坂総合病院呼吸器内科
生方 智 神宮 大輔 矢島 剛洋 庄司 淳 高橋 洋
(平成 25 年 6 月 17 日受付)
(平成 25 年 7 月 30 日受理)
Key words : septic pulmonary embolism,Peptostreptococcus micros
序 文
敗血症性肺塞栓症(Septic pulmonary embolism,
SPE)は敗血症に伴う菌塊が塞栓子となって肺動脈に 塞栓を来す稀な疾患であり,臨床症状として発熱,呼 吸器症状を伴い,画像所見では肺野末梢に両側性にし ばしば空洞を伴う多発結節影を示す1).SPE は通常は 急性かつ重篤な疾患であるが2),今回私たちは慢性の 経過で多彩な頭頸部病変を呈したPeptostreptococcus
microsによる SPE の 1 例を経験したので報告する.
症 例 患者:46 歳,男性.
主訴:めまい,食思不振.
既往歴:特記事項なし.
服薬:サプリメント,漢方薬含めてなし.
喫煙歴:current smoker(40 本×13 年間).
飲酒歴:機会飲酒程度.
職業歴:土木業.
居住環境:千葉県で同僚 6 人と寮での共同生活.実 家が宮城県.
現病歴:当院受診 2 カ月前から難聴や左眼瞼腫脹を 自覚した.近医耳鼻科や眼科で内服抗菌薬による治療 を受けていたが改善しなかったため,特発性眼窩炎症 の診断でステロイド治療を受けた.当初プレドニゾロ ン 30mg!日から開始され,以後 1 週間毎に漸減投与 されていたが自覚症状は改善せず,治療開始 1 カ月で 通院を自己中断した.その後も仕事を続けていたが,
当院受診 2 週間前より回転性めまいと食思不振が出現 したため宮城県に帰省し,当院内科外来を受診した.
外来受診時の体温は 36.6℃ で,身体所見においては
両側耳漏を認めたが,咳嗽や喀痰などの呼吸器症状は 認めなかった.スクリーニングでの胸部単純レントゲ ン写真にて両肺多発結節影を認め,精査加療目的で当 科に入院した.
入院時現症:身長 183cm,体重 63kg(2 カ月間で 15 kg の減少),血圧 102!69mmHg,脈拍数 130!分・整,
体温 39.2℃,SpO2(大気下)98%.両側膿性耳 漏 あ り,左眼瞼腫脹と眼球運動障害あり(Fig. 1A),視野・
視力障害なし.両側扁桃腫大なく,咽頭に異常なし,
齲歯多数.左頸部に圧痛あるが,リンパ節腫脹はなし.
胸部・腹部・皮膚・関節所見に異常なし.
入院時検査所見(Table 1):白 血 球 数 18,600!μL,
CRP 23.5mg!dL,赤沈 60 分 119mm と著明な炎症所 見を認めた.胸部 CT では両肺野末梢を主体に多発結 節影を認め,内部は充実性から空洞まで様々な病変を 呈していた.また,頭頸部 CT では両側乳突蜂巣の含 気低下,左眼窩内と深頸部に腫瘤性病変を認めた(Fig.
1B,Fig. 2).
入院後経過:臨床経過は慢性であり,頭頸部と肺病 変の存在から入院当初は Wegener 肉芽腫症,悪性腫 瘍などを疑った.しかし,入院直後に発熱を認め,そ の際に採取した血液培養 2 セットと両側耳漏培養から
P. microsが検出されたことから,頭頸部領域の膿瘍に
随伴した SPE が疑われた.血液培養陽性が判明した 入院 3 日目からメロペネム 0.5g×3 回!日を開始した.
さらに,入院 7 日目に肺病変評価のため気管支鏡検査 を行った.細胞診 classI,培養検査にて一般細菌,真 菌,抗酸菌は検出されなかった.全身検索にて悪性腫 瘍は認めず,頭頸部病変以外の感染巣や感染性血栓性 静脈炎は確認できなかった.
メロペネム開始後にめまいや膿性耳漏などの臨床症 症 例
別刷請求先:(〒985―8506)宮城県塩釜市錦町 16 番 5 号
坂総合病院呼吸器内科 生方 智
Fig. 1A Eye movement on admission (A1-4) and on the 40th hospital day (A1ʼ-4ʼ). Although left eye movement disorder was present on admission, on the 40th hospital day, the disorder had improved after the antimicrobial therapy.
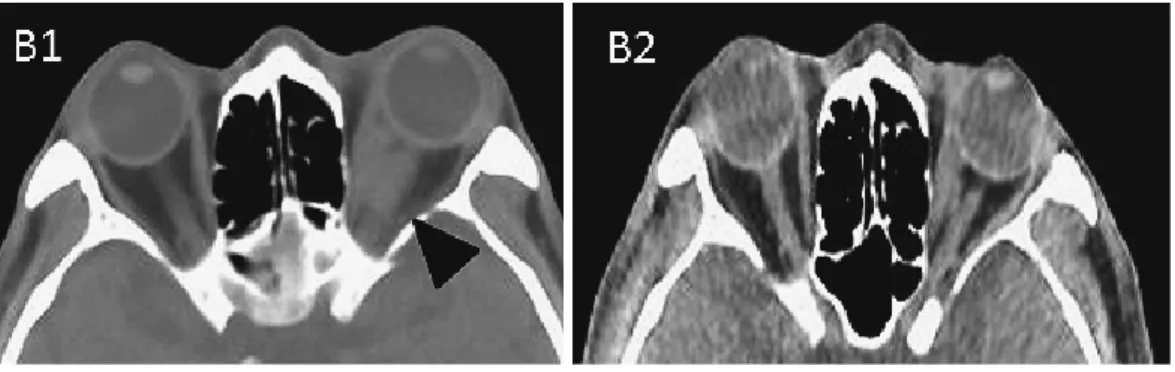
Fig. 1B Axial CT of the orbits (B1). A mass lesion is present in the left orbit on admission (arrow head). The intraocular pressure of the right and left were different (right; 12mmHg, left;
17mmHg). The CT image taken on the 57th hospital day (B2), showed reduction of the mass le- sion and the intraocular pressure was 13 mmHg in both eyes.
Table 1 Laboratory findings on admission and bacterial test
Hematology Biochemistry Other tests
WBC 18,600 /μL AST 52 IU/L HIV negative
Seg 97 % ALT 82 IU/L HTLV-1 Ab negative
Lympho 1 % ALP 506 IU/L
Mono 2 % γ‐ GTP 141 IU/L β-D-glucan <1.2 pg/dL
Eosino 0 % T.Bil 0.8 mg/dL Aspergillus Ag negative
RBC 449×104/μL LDH 185 IU/L Cryptococcus Ag negative
Hb 12.5 g/dL CK 123 IU/L
PLT 43.8×104/μL Na 131 mEq/L Bacterial culture
K 4.3 mEq/L blood P. micros
Coagulation Cl 94 mEq/L otorrhea P. micros
PT% 59.3 % BUN 15.4 mg/dL sputum S. pneumoniae
PT-INR 1.38 Cr 0.62 mg/dL BAL* negative
APTT 36.6 sec TP 7.8 g/dL CSF** negative
D-dimer 2.18 mg/mL Alb 2.5 g/dL neck abcess negative
CRP 23.5 mg/dL
Urinalysis ESR 1hour 119 mm Blood sugar 108 mg/dL
Protein (2+) HbA1c (JDS) 6.4 %
Occult blood (1+) MPO-ANCA <1.3 IU/mL
Glucose (−) PR3-ANCA <3.5 IU/mL
*; Bronchoalveolar lavage, **; Cerebrospinal fluid
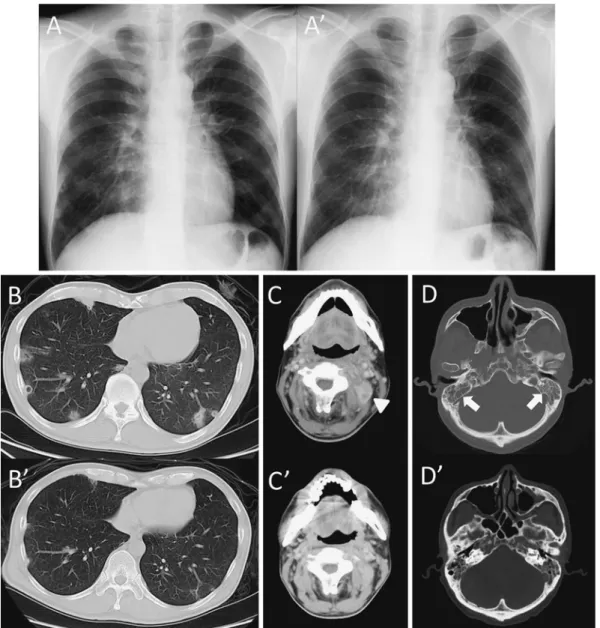
Fig. 2 Chest radiography on admission showed multiple nodules (A). Chest CT (B) demonstrated bilateral multiple pulmonary nodules and cavities. (C) Axial CT slice of the third cervical verte- bra showed a mass lesion (arrow head). (D) Acute mastoiditis is seen in both ears (arrow). Fol- low up chest radiograph (Aʼ) and CT (Bʼ 〜 Dʼ) showed that all lesions had almost disappeared after the antimicrobial therapy for five weeks.
状は速やかに改善した(Fig. 3).P. microsの薬剤感受 性(Table 2)が判明し,ペニシリン系に感受性があ ることを確認の後,アンピシリン 2g×4 回!日に de- escalation した.抗菌薬はメロペネムを 7 日間,アン ピシリンを 28 日間の合計 35 日間投与した.治療終了 時には眼球運動所見の改善と左眼球の眼圧の低下が認 められ(Fig. 1A),治療終了 1 カ月後に施行した CT 所見においても両肺野の多発結節影の消失,両側乳突 蜂巣の含気改善,左深頸病変の消失,左眼窩内病変の 縮小を確認した(Fig. 1B,Fig. 2).後日,本症例の 保存検体より DNA を抽出してP. microsの 16S rRNA 遺伝子をターゲットとした nested PCR を施行した.
既存報告3)に沿ってまず 1st round PCR を施行,続い
て内部に新規 primer を設定して(SENSE 5ʼ-AGGGG GATAGCCGTTGGAAA-3ʼ,ANTISENSE 5ʼ-ACCTG TATAGTTGTCCCGA-3ʼ),同一の条件で 2nd round PCR を施行した.患者検体を用いた検索では,培養 陰性であった喀痰,気管支肺胞洗浄液(Bronchoalveo- lar lavage,BAL)および頸部穿刺液においても 870bp の 16S rRNA 遺伝子断片が増幅された(Fig. 4).
考 察
敗血症性肺塞栓症(Septic pulmonary embolism,
SPE)の原疾患は Lemierre 症候群4)が有名であり,代 表 的 な 起 炎 菌 はFusobacterium speciesで あ る.Le- mierre 症候群以外の頭頸部領域の報告では硬膜静脈 洞内血栓を伴うくも膜下膿瘍5)や乳様突起炎6),及び歯
Fig. 3 Clinical course MEPM: meropenem, ABPC: ampicillin BT: body temperature
Fig. 4 The specific PCR for Peptostreptococcus mi- cros
M, Marker; lane 1, Positive control; lane 2, Nega- tive control; lane 3, Neck abscess; lane 4, Cerebro- spinal fluid; lane 5, Urine; lane 6, Bronchoalveolar lavage; lane 7, Bronchial lavage; lane 8, Sputum Table 2 Antimicrobial susceptibility of
Peptostreptococcus micros
antimicrobial susceptibility MIC (μg/mL)
PIPC S ≦32
LMOX S ≦16
GM R ≧64
CLDM S ≦2
MINO S ≦4
CFX S ≦16
PIPC: piperacillin, LMOX: latamoxef, GM: genta- micin, CLDM: clindamycin, MINO: minocycline, CFX: cefoxitin
性感染症7)などが報告されている.我々が検索した限 りでの本邦の SPE 報告例は 98 例であり,そのほとん どは急性経過であった.また,起炎菌が判明した 68 例(69.4%)のうち,Peptostreptococcus species の症 例は感染源が肝膿瘍8)と口腔内感染症9)の 2 例のみで あった.本邦以外の報告においても,Sinave ら10)の報 告ではPeptostreptococcusspecies による SPE を合併し た Lemierre 症候群は 38 例中 2 例と稀であり,その 臨床経過も咽頭感染後の急性経過であり,本症例の様 な慢性経過の症例は極めて稀な病態と考えられた.
P. microsはグラム陽性嫌気性球菌であり,1990 年
代後半に導入された遺伝子解析に基づく遺伝学的分類 法(系統分類)においてはParvimonas micraに分類さ れている11).通常は口腔内や消化管の細菌叢を形成し ている12)が,歯性感染症以外にも頭頸部や肺などの深 部感染症の病原菌として臨床細菌学的に重要性が高い
菌種である.一方で血液培養陽性例中のPeptostrepto-
coccus属の占める割合は当院の 2001 年から 2011 年の
10 年間のデータでは 0.2% であり,文献的13)にも 0.4%
と低く,菌血症の起炎菌としては稀と考えられる.本 症例では血液培養陽性と検体採取が困難な眼窩内病変 を除いた全ての検体においてP. microsが培養あるい は PCR 陽性であり,血行性進展を伴った一元的なP.
micros感染症と診断した.
本症例の推定感染経路として,齲歯や頭頸部病変が
P. microsの侵入門戸となって血行性に深頸部や肺に病
変を形成したと考えられた.また,臨床経過が慢性で あったのは,治療自己中断やステロイド投与による免 疫力低下が関与したと推測された.
SPE に対する抗菌薬投与期間は 4〜8 週間と報告さ れている2).P. microsの薬剤感受性はペニシリン系に 対して通常良好であるが,耐性株も報告されており14), 抗菌薬投与期間が長期に及ぶ疾患であるので抗菌薬選 択と菌株の感受性の確認は重要である.本症例では,
ペニシリン感受性株であることを確認の上,アンピシ リンへの de-escalation を行った.また,脳静脈洞血 栓を有する症例では抗凝固療法が行われることがあ る5)が,血栓が確認されない症例には推奨されていな い2).本症例では全身検索にて血栓は確認できなかっ たため抗凝固療法は行わず,抗菌薬治療期間は 5 週間 であったが治療終了後の再燃は見られていない.
今回我々は慢性の経過で多彩な頭頸部病変を呈した
P. microsによる SPE の 1 例を経験した.多発肺結節
影に遭遇した際には慢性経過であっても SPE を鑑別 診断の一つとして認識しておくことが望ましい.
本論文の要旨は第 61 回日本感染症学会東日本地方 会学術集会(2012 年 10 月)において報告した.
利益相反自己申告:申告すべきものなし 文 献
1)Cook RJ, Ashton RW, Aughenbaugh GL, Ryu JH:Septic pulmonary embolism : presenting features and clinical course of 14 patients.
CHEST 2005;128:162―6.
2)Golpe R, Marin B, Alonso M:Lemierreʼs syn- drome (necrobacillosis). Postgrad Med J 1999;
75:141―4.
3)Riggio MP, Lennon A, Smith A:Detection of Peptostreptococcus microsDNA in clinical samples by PCR. J Med Microbiol 2001;50:249―54.
4)Lemierre A:On certain septicaemias due to anaerobic organisms. Lancet 1936;230:701―3.
5)Hoshino C, Satoh N, Sugawara S, Kuriyama C, Kikuchi A, Ohta M:Septic cavernous sinus thrombosis complicated by narrowing of the in- ternal carotid artery, subarachnoid abscess and
multiple pulmonary septic emboli. Intern Med 2007;46:317―23.
6)Lee SJ, Weon YC, Cha HJ, Kim SY, Seo KW, Jegal Y,et al.:A case of atypical skull base os- teomyelitis with septic pulmonary embolism. J Korean Med Sci 2011;26:962―5.
7)Shiota Y, Arikita H, Horita N, Hiyama J, Ono T, Ohkawa S,et al.:Septic pulmonary embolism associated with periodontal disease : Reports of two cases and review of the literature. CHEST 2002;121:652―4.
8)高松健次,南川博司,西本正紀,宮本 修:肝
膿 瘍 に 併 発 し たPeptostreptococcusに よ る septic pulmonary emboli の 1 例.感 染 症 誌 1984;
58:340―6.
9)諫田淳也,蝶名林和久,渡邊光正,有馬靖佳,通
堂 満:Lemierre 症 候 群 の 1 例.内 科 2005;
96:386―8.
10)Sinave CP, Hardy GJ, Fardy PW:The Le- mierre syndrome : suppurative thrombophlebitis of the internal jugular vein secondary to oro- pharyngeal infection. Medicine 1989;68:85―
94.
11)渡邊邦友,後藤隆次,田中香お里:グラム陽性
嫌気性球菌群〜分類命名の変化と病原因子・全 ゲノム解析研究の動向.モダンメディア 2010;
56:16―24.
12)Murdoch DA:Gram-positive anaerobic cocci.
Clin Microbiol Rev 1998;11:81―120.
13)Cockerill FR 3rd, Hughes JG, Vetter EA, Muel- ler RA, Weaver AL, Ilstrup DM,et al.:Analysis of 281,797 Consecutive Blood Cultures Per- formed over an Eight-Year Period : Trends in Microorganisms Isolated and the Value of An- aerobic Culture of Blood. Clin Infect Dis 1997;
24:403―18.
14)Wren MW:Anaerobic cocci of clinical impor- tance. Br J Biomed Sci 1996;53:294―301.
A Case of Septic Pulmonary Embolism due toPeptostreptococcus micros with Multiple Infection of the Head and Neck
Satoshi UBUKATA, Daisuke JINGU, Takehiro YAJIMA, Makoto SHOJI & Hiroshi TAKAHASHI Department of Respiratory Medicine, Saka General Hospital
A 46-year-old man with no underlying diseases visited our hospital with otorrhea, ocular motility disor- der of the left eye, dizziness and loss of appetite which had lasted for two months. Chest radiography and computed tomography (CT) showed bilateral multiple pulmonary nodules and cavities. Furthermore, CT of the head and neck revealed bilateral mastoiditis, a left orbital abscess and a deep neck abscess.Peptostrepto- coccus microswas cultured from blood and otorrhea specimens. In addition,P. microsDNA was detected with the polymerase chain reaction (PCR) method in the specimens from the site of culture-negative lesions (i.e.
sputum, bronchoalveolar lavage, neck abscess). Thus, we diagnosed the lung lesions as septic pulmonary em- bolisms (SPEs). The clinical findings of the head and neck had improved following antibiotics treatment for five weeks, and follow-up chest radiography and CT showed that all lesions almost disappeared. Since some SPE patients demonstrate a slow progression, SPE should be included in the differential diagnosis of multi- ple pulmonary nodules such as Wegenerʼs glanulomatosis or neoplasm.
〔J.J.A. Inf. D. 87:761〜766, 2013〕