防衛医科大学校 脳神経外科(受稿日 2015. 12. 6)(脱稿日 2016. 6. 17)〔連絡先:〒 359-8513 埼玉県所沢市並木 3-2 防衛医科大学校 脳神 経外科 大谷直樹〕[Address correspondence: Naoki OTANI, M.D., Department of Neurosurgery, National Defense Medical College, 3-2 Namiki, Tokorozawa, Saitama 359-8513, Japan]
脳卒中の外科 44: 417 〜 424,2016
特集 バイパス術に関連する問題
慢性期脳虚血性病変に対して安全確実に
STA-MCA バイパス術を完遂するための外科的治療戦略
大谷 直樹,和田孝次郎,井中 康史,西田 翔,田之上俊介
熊谷 光佑,藤井 和也,豊岡 輝繁,森 健太郎
Surgical Strategies and Technical Tips for Performing
Extracranial-Intracranial Bypass for Occlusive Cerebrovascular
Disease
Naoki O
TANI, M.D., Kojiro W
ADA, M.D., Yasufumi I
NAKA, M.D., Sho N
ISHIDA, M.D.,
Shunsuke T
ANOUE, M.D., Kohsuke K
UMAGAI, M.D., Kazuya F
UJII, M.D.,
Terushige T
OYOOKA, M.D., and Kentaro M
ORI, M.D.
Department of Neurosurgery, National Defense Medical College, Tokorozawa, Saitama, Japan
Summary: Extracranial-intracranial (EC-IC) bypass is one of the most fundamental techniques for cerebrovascular surgery. We describe our surgical results and strategy for performing the EC-IC by-pass safely and precisely in patients with chronic stage ischemia. Surgical indications were decided for symptomatic internal carotid or middle cerebral artery occlusive disease with misery perfusion detected using quantitative single-photon emission computed tomography. Antiplatelet medications were continued, and intravenous hyperosmotic colloid infusion was started 1 week before operation. Target recipient M4 arteries were superimposed on the superficial temporal artery and cranial bone. Preparation of the superficial temporal artery was performed by using an ultrasound instrument (Har-monic Scalpel®). The craniotomy site was located under the supratemporal line. Various anastomotic
techniques were adopted, including continuous, running, and intermittent suturing methods. The sec-ond target recipient artery was confirmed using intra-arterial indocyanine green videoangiography. Hyperbaric oxygen therapy was performed for wound problems. Forty patients (43 sides) underwent EC-IC bypass between September 2010 and March 2015 (mean age, 64.5 years; 28 men and 12 women; double bypass in 35 patients and single bypass in eight). Postoperative complications were chronic subdural hematomas and skin problems in five patients each. None of the patients had permanent deficit. Well-drained operative field and steady hand movements are necessary to perform safe and se-cure bypass procedures. The various technical tips and surgical strategies that we have suggested can contribute to improving surgical results.
Key words: ・ STA-MCA bypass ・ surgical results ・ EC-IC bypass ・ microneurosurgery Surg Cereb Stroke (Jpn) 44: 417-424, 2016
原 著
は じ め に
わが国においては,Japanese Extracranial-Intracranial
(EC-IC) Bypass Trail において血行力学的脳虚血例に対
する浅側頭動脈-中大脳動脈吻合(superficial temporal
ar-tery-middle cerebral artery〔STA-MCA〕バイパス)術に
よる脳梗塞の予防効果の優位性が示された
14)15).一方で,
1985 年の EC-IC Bypass Study group からの randomized
trial study を 筆 頭 に
5),2011 年 の Carotid Occlusion
Sur-gery Study(COSS)
23)では,内科的治療に対するバイパス
術の優位性はみられなかったと報告されている.したがっ
て,今後もさらなる厳密な手術適応のもと安全かつ確実に
手術を遂行し,可及的に合併症を軽減させるべく手術戦略
を立て術中手技を洗練させていく必要がある.ここで
は,われわれの施設における安全かつ確実な血管吻合と血
流改善を目的とした慢性期 STA-MCA バイパス術に対す
る手術戦略と治療成績を提示するとともに,文献的考察を
加えて報告する.
対象患者と方法
症候性(一過性脳虚血発作,あるいは minor stroke)の内
頚動脈系主幹動脈〔MCA,内頚動脈(internal carotid
ar-tery:ICA)〕の狭窄,あるいは閉塞性病変を認める症例
で,modified Rankin Scale(mRS)が 1-2 で activity of
dai-ly living(ADL)が自立しており,広範囲脳梗塞を認めず,
quantitative single photon emission computed
tomogra-phy(QSPECT)精査にて脳血管予備能障害(Stage Ⅱ領域)
がみられる症例を手術対象とした.手術は全例ともに発症
後,慢性期に施行した.もやもや病,類もやもや病,さら
には急性期血行再建を目的とした緊急バイパス症例は本患
者対象群からは除外した.入院記録,手術記録,および画
像所見から臨床像と治療成績を後方視的に検討した.
手術前準備
術前精査において心機能を評価して,虚血性心疾患の合
併の有無を確認した.また,頚部の頚動脈狭窄病変の有無
を確認した.複数の抗血小板薬を内服している場合には手
術 1 週間前から単剤に減薬した.ただし,一過性脳虚血発
作が持続している場合には複数投与を継続した.抗凝固薬
を内服している患者では,いったん休薬してヘパリン持続
点滴に移行した.手術 1 週間前から脱水補正を目的とし
て,低分子デキストラン 250 ml/日の持続点滴を開始した.
手術戦略の策定
頭部 computed tomography(CT),magnetic resonance
imaging(MRI)と digital subtraction angiography(DSA)に
よる解剖学的情報に加えて QSPECT にて頭蓋内血流動態
を把握することによって適切な recipient artery,ならび
に開頭範囲を決定した.頭部 CT は Aquilion
TM64 列(東芝
メディカルシステムズ)を用いておのおのの volume data
を収集した.得られたデータは,ワークステーション(Zio-station,ザイオソフト)に転送して,volume rendering 法
を用いた画像構築を施行した.閾値法を用いて骨を画像か
ら消去することにより,脳表を走行する動脈(M4)の形態
が把握できるような three dimensional computed
tomog-raphy angiogtomog-raphy(3D-CTA)画像を作成し,術前シミュ
レーションを施行した(Fig. 1A).recipient artery の選定
については SPECT による血流低下部位,さらには吻合に
おける容易性などを考慮して決定した.
手 術 方 法
全身麻酔導入前に STA の走行を確認し,recipient
ar-tery をトレースして開頭範囲をマーキングした.double
anastomosis 症例では,STA 頭頂枝の直上を皮膚切開し
て,前頭側へいたる弧状の皮膚切開を施行した.収縮期血
圧は 120 mmHg 以上,呼気中 CO
2濃度を 40-45 mmHg に
維持した.また,麻酔導入時に不用意な血圧低下をきたさ
ぬように注意喚起をした.手術体位は jack knife position
で,可及的に髄液の流出を防止すべく,開頭部位が最上位
になるように留意しながら 3 点固定した.体幹は,左右回
転ができるように側板固定を施行した.
STA の剝離と断端の処理
STA の剝離には Harmonic scalpel を使用した(Fig. 1B).
55,000 Hz の超音波ブレード振動による摩擦熱により組織
中の蛋白変性をきたし,粘着性物質を生成することで血管
をシールして止血効果を得ながら切開を進める器具であ
る
31).局所麻酔はせず,15 番メスで皮膚切開後,先細り
モスキートペアンにて parietal branch 直上を全長剝離
し,小児用ゴムフックで展開した.STA 基部,頭頂枝,
前頭枝を剝離して,おのおの 1 号絹糸で確保した.その絹
糸を持ち上げながら,Harmonic scalpel で STA を全周剝
離した.前頭枝,頭頂枝ともに 7 cm 以上剝離して切離し
た.ヘパリン加生理食塩水で血管内腔を洗浄し,十分膨ら
ませて 20 万倍塩酸パパベリンを塗布したセレシート(富士
システムズ)で被覆した.STA 断端の処理は注射器に接続
したヒーロン針を STA 内腔に挿入留置し,左手の鑷子で
外膜をもちながら,右手のマイクロハサミで吻合部から約
1 cm にわたって外膜を十分に切離除去した.吻合面は約
60 度で切開し,さらに追加切開して吻合長は約 3 mm(目
盛付ラバーダム上で計測)とした.pyoktanin blue
mark-ing pen を用いて吻合部に直接塗布することで,視認性の
向上に努めた(Fig. 1E).
開頭と吻合術野の作成
開頭範囲は可及的に上側頭線内に収まるようにした.硬
膜切開の直前にインドシアニン・グリーン(indocyanine
green:ICG)を静注して,脳表の target recipient artery
あるいは sylvian vein の位置を確認して,必要最小限の硬
膜切開を施行した(Fig. 1C, D).吻合術野の作成について
は,可及的に髄液排出を抑え,recipient artery の下にラ
バーダム,ゼルフォームを敷くことでできるだけ縫合部を
Fig. 1 We preoperatively obtained a three-dimensional computed tomographic angiographic image, which allowed us to understand the anatomical architecture of the superficial temporal artery (STA), recipient artery, and extent of the craniotomy (A). Preparation of the STA was performed using Harmonic Scalpel. Friction heat produced by the ultrasound instrument induces protein changes, allowing for dissection of the STA with complete hemostasis. The parietal branch is carefully dissected using the ultrasonic scalpel with elevation performed using 1-0 silk suture (B). Just before dural opening, indocyanine green angiography is performed to confirm the re-cipient superficial cerebral artery over the dura (C) and trace the superficial cerebral artery. This helps to minimize the dural opening (D). After cutting the end of the STA, we usually perform direct marking with a pyoktanin skin-marking pen to identify the anastomosis layer (E).
A B C D E
浅くするように留意した.低出力バイポーラを用いて,
recipient artery の側枝の処理に努めた.可及的に開頭辺
縁での操作は避けるようにして,周辺の硬膜下腔への血液
貯留を防止すべくセレシートにて被覆した.semi-wet な
縫合環境と,完全止血による視認性の向上に努めた.
吻 合 操 作
recipient artery の遮断には,AVM クリップを使用し
た
16).動脈切開に先行して,吻合部の視認性の向上を目的
に pyoktanin blue marking pen を吻合部に直接塗布してか
ら動脈切開を施行した(Fig. 2A).動脈切開には,FUJITA
8027-14 の強弯ハサミを用いて,fish mouse 型で縫合長は
約 3.0 mm(目盛付ラバーシート下)とした.stay suture を
施行後,stay suture 近傍から縫合開始した.縫合は最大
強倍率で針を通し,針を抜きながら弱倍率で針を置き,中
間倍率に戻して糸を結紮切離する操作を繰り返した.鑷子
は先端 0.3 mm REDA(弱弯,直),BONIMED 5XL(18 cm)
を 使 用 し た.rail road 法, あ る い は 連 続 縫 合・ 間 欠 結
紮・待針法を併用した(Fig. 2B, C).使用する 10-0 糸の長
さは 4 cm,針は 2-3 針かけたら新しい針に替えるように
した.double anastomosis においては,1 本目の吻合が終
了後にもう 1 本の STA から ICG 動注にて 1 本目の STA
吻合による灌流域を確認後,1 本目の吻合と異なる灌流域
の recipient artery を選定して可及的に広範囲の血流範囲
を獲得すべく 2 本目の吻合を施行した(Fig. 2D, E).吻合
血管の最終確認は ICG 静注にて確認した(Fig. 2E).髄液
漏出の防止を目的にゼルフォーム(Gelfoam,ファイザー)
とフィブリン糊を用いてくも膜形成を施行した.
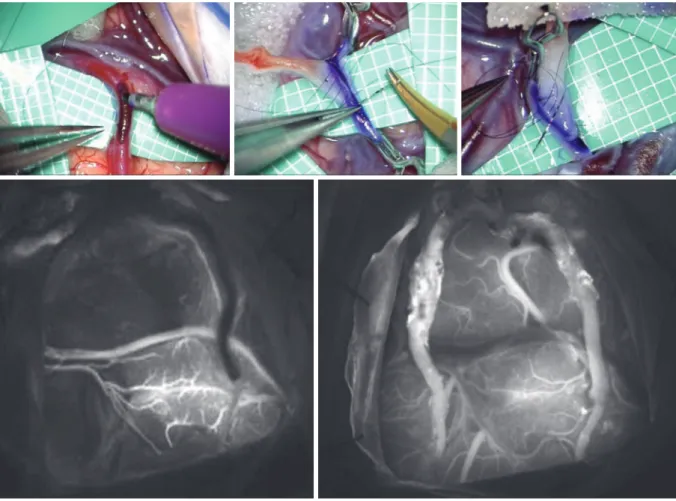
Fig. 2 Wide operative field and avoiding anastomosis at the border site of the craniotomy, and maintenance of the semi-wet condition and complete hemostasis are desirable. Just be-fore arteriotomy of the recipient artery, direct marking using a pyoktanin skin-marking pen is performed to clarify the anastomosis layer (A). Various anastomotic techniques are per-formed, using continuous, running, and intermittent suturing methods (B, C). After com-pleting the first anastomosis, the patency and circulation area are checked with intra-arte-rial indocyanine green injection from another superficial temporal artery branch (D). The second anastomosis should be performed on the area without circulation from the first anastomosis (E), which helps to achieve a wide circulation area.
A B C D E
術 後 処 置
術後は,慢性硬膜下血腫の予防目的に五苓散(ツムラ)を
処方した.術直後は,ハイドロゲル創傷被覆保護剤(カラ
ヤヘッシブ
TM,アルケア)にて創部を被覆し,術後 4 日目
からはアルプロスタジル アルファデクス(プロスタンディ
ン軟膏 0.003%
TM,小野薬品工業)とゲンタマイシン硫酸塩
軟膏(ゲンタシン軟膏 0.1%
TM,MSD)による創部処置に努
めた.術後 10 日目付近の抜糸時に創傷治癒遅延がみられ
た症例については,ただちに高気圧酸素(hyperbaric
oxy-gen:HBO)治療を開始した(Fig. 3A-C).
結
果
2010 年 9 月から 2015 年 3 月までの 4 年半の間に,当院
において慢性期バイパス手術を施行した症例は,計 40
例,43 側〔平均年齢 64.5 歳(39-73 歳),男性 28 例,女性
12 例,右側 25 例,左側 18 例〕であった.責任病型は,
MCA 狭窄 20 例,ICA 狭窄 11 例,ICA 閉塞 13 例,総頚動
脈(common carotid artery:CCA)閉塞 1 例,CCA 閉塞 1
例で両側病変は 6 例であった.発症形式は脳梗塞 23 例,
一過性脳虚血発作 17 例で,運動機能症状はのべ 35 例,失
語症状はのべ 15 例,体性感覚障害は 4 例にみられた.手
術はいずれも donor artery に STA を使用し,double
by-pass が 35 側,single byby-pass が 8 側で施行された.全症例
で術後の吻合血管の血流は開存しており,血管予備能の改
善がみられた.対側病変に carotid endarterectomy(CEA)
を追加施行した症例が 3 例みられた.退院時転帰は good
recovery 38 例,moderate disability 5 例であった.合併
症は創部治癒遅延例が 5 例(11.6%)にみられ 4 例に HBO
治療を施行し,いずれも 3 カ月後には軽快した.慢性硬膜
下血腫が 5 例(11.6%)にみられ,うち 3 例は自然軽快し,
うち 2 例(4.7%)に外科的治療を要し軽快した.周術期脳
梗塞を生じた症例はなく,過灌流症候群を含めた出血性合
併症例はみられなかった.surgical morbidity,mortality
はいずれも 0%で永続的神経学的脱落徴候が残存した症例
はみられなかった.平均観察期間は 36 カ月(9-58 カ月)
で,その間には脳梗塞の再発はみられなかった.
考
察
STA-MCA バイパス術は,Yasargil ら
35)によって初め
て施行された外科的手技であり,その後 30 年以上にわ
たって脳虚血疾患,もやもや病,治療困難な頭蓋内動脈瘤
に対して多くの脳神経外科医によって発展施行されてき
た. 一 方,1985 年 の EC-IC Bypass Study group に よ る
報告では,症候性 ICA,あるいは MCA 狭窄症 1,377 名の
患者において,脳梗塞再発に関して内科的治療に対するバ
イパス術の優位性が得られなかった
5).2010 年には Fluri
ら
9)が Cochrane Stroke Group Trials Register を調査した
結果,症候性 ICA 閉塞症に対して内科治療単独群に比較
して内科治療+EC-IC バイパス群では優劣がみられな
Fig. 3 Hyperbaric oxygen (HBO) therapy is useful for the treatment of skin problems after surgery. This patient underwent right superficial temporal artery (STA)-radial artery (RA)-M3 bypass for middle cerebral artery stenosis and had undergone craniotomy for depressed skull frac-ture and removal of the parietal branch of the STA 10 years prior. Two weeks after the sur-gery, skin fistula and exudative fluid collection appeared (A: red arrow). HBO therapy was immediately started, for about 2 hours per day. One week after initiation of the HBO thera-py, the fistula had disappeared (B). After 2 weeks of therathera-py, the skin condition had almost completely resolved (C).
かったと報告している.しかし,いずれの論文も脳血管予
備能障害に基づく血行再建術の手術適応は考慮されてい
なかった.最近では,COSS において症候性 ICA 閉塞症に
おける 2 年間の脳梗塞再発率に関して血行再建術の非有効
性が示唆された報告もみられる
23).しかし,本報告では内
科的加療による脳梗塞の再発率が低値であることと,バイ
パス加療群において周術期合併症が非常に多いことがバイ
パス術の非優位性につながったものと考えられる
23)24)う
え,あくまでも 2 年間以内の短期再発率しか確認しておら
ず,長期の脳梗塞や一過性脳虚血発作の再発については言
及していないゆえ,標準的治療指針としては不十分である
とする意見もある
2).一方で,脳血管予備能の障害に着目
し て 血 行 再 建 術 の 有 効 性 を 示 唆 し た 論 文 も 散 見 さ れ
る
3)14)19)22)26)28)29).血行再建術自体に伴う合併症を最小限に
軽減させ,安全かつ確実な血管吻合による脳血流増加に伴
う脳血管予備能の改善による脳梗塞の再発率を低下させる
べく努めていく必要がある.手術の低侵襲化を目的に小開
頭によるバイパス術の有用性も報告されている
8)17)37).さ
らに,脳梗塞の再発率の低下のみならず,術後の脳血流増
加に伴い高次脳機能障害の改善も期待し得るとの報告もあ
る
4)7)20)21).今回われわれの治療群においても,認知機能が
改善した症例が 3 例にみられた.今後も症例を重ね,バイ
パス術前後の認知機能における有効性を検証する予定であ
る.
術前の抗血小板薬の休薬開始の時期や,その間の最適な
処置について標準的治療指針はない.休薬すれば外科処置
の際の止血は容易になり,出血性合併症も軽減するものと
思われるが,一方で脳梗塞再発の危険性が危惧される.佐
藤ら
27)は,アスピリンの休薬に要する日数は 7-10 日,シ
ロスタゾールは 2-3 日,硫酸クロピドグレルは 14 日とさ
れるが,アスピリンとシロスタゾールは休薬 3-4 日目で薬
剤効果は消失すると報告している.われわれは,複数の抗
血小板薬を内服している場合には手術 1 週間前から単剤に
休薬し,通常は硫酸クロピドグレル単剤服用を継続しなが
ら周術期も継続している.手術 1 週間前から血管内脱水予
防を目的として低分子デキストラン 250 ml/日の持続点滴
を開始している.
近年,ICG 蛍光脳血管撮影の有用性に関する報告が散見
される.静脈内投与による ICG 造影にて最終的な吻合血
管の血流を確認しているが
6)13)34),硬膜切開直前にも静脈
ICG 造影を施行して,recipient artery としての脳表動脈
を透見しながら pyoktanin blue marking pen にて硬膜上
に脳表血管の走行を直接マーキングすることで硬膜切開線
を最小限にできるように工夫している.また,double by-pass において 2 本目を縫合する recipient artery の選定に
ついては,ICG 動注にて 1 本目に吻合した STA による灌
流域を確認後,1 本目の吻合と異なる灌流域の recipient
artery を選定して可及的に広範囲の血流改善域を獲得す
るようにした.通常,ICG は静脈内投与が原則であるが,
動脈内投与による臨床応用の有用性に関する報告も散見さ
れる
11)18)25).いずれも,通常の静脈内投与の際の 10 倍希
釈濃度で使用しており,安全性も担保されている.
本手術の代表的な併発症として,いずれも開頭手術に関
連した併発症であるが,慢性硬膜下血腫と創部治癒遅延が
挙げられる
36).動脈硬化性病変で糖尿病や脂質異常症など
の創部トラブルの危険性が潜在しているうえ,donor ar-tery としての STA の剝離切離に伴い創部血流障害が大き
な要因である.特に基礎疾患に糖尿病を有しており
dou-ble bypass を施行した症例は重篤な創部トラブルが発生す
る危険性が有意に高く留意すべきである
30).われわれの症
例でも創部治癒遅延例が 5 例(11.6%)にみられ,いずれも
double bypass 施行例であり,3 例に糖尿病の既往があ
り,1 例では幼少期に頭蓋咽頭腫に対する放射線加療の既
往があった.術中注意点としては,閉創時に帽状腱膜を縫
合して可及的に血流阻害の防止に努め,術後の創処置に無
効例に対しては抜糸後,ただちに HBO 治療を開始して良
好な経過を得ている(4 例で治癒).1 例は HBO 治療を導
入前の症例であり,幸いにも形成外科治療を施行するにい
たらなかったが,治癒するまでに外来通院処置を 6 カ月ほ
ど要した.創傷治癒遅延に対する HBO 治療の有効性に関
する報告は散見される
32)ものの,機序については不明であ
る.Wilson ら
33)の報告では,創傷部の治癒過程で重要な
役割を果たす線維芽細胞であり,一方で血行不全のある肉
芽の盛り上がりが不良であるほど酸素分圧が低下している
ことから,HBO 治療により酸素分圧を上昇させることが
線維芽細胞の活性化につながり治癒を促進するとされてい
る.しかし,HBO 治療のみでは限界があることも事実で
あり,あくまでも創傷治癒遅延が疑われた初期段階におい
ては有効であると思われるが,排膿などの感染が明らかに
なった症例では早急に外科的処置を考慮すべきであろ
う.血行再建術後の慢性硬膜下血腫については,抗血小板
薬の内服,慢性動脈硬化に起因する脳萎縮の存在などから
その併発が危惧される
1)10)12).さらに,症候性となり外科
的ドレナージを要する場合には,硬膜下に走行する donor
artery の存在や再開創に伴う皮膚癒着遅延の有無や感染
の併発などが危惧される.ゆえに,術中予防処置とし
て,くも膜切開範囲の可及的縮小,くも膜閉鎖による硬膜
下腔の軽減,さらに術後早期から五苓散内服を開始して慢
性硬膜下血腫併発の軽減に努めている.今後さらなる予防
法の出現に期待したい.
結
語
STA-MCA バイパス術は,厳格かつ適正な手術適応の
もと,術野の展開と手術手順を洗練させることで合併症を
軽減し,安全かつ確実な血管吻合術が可能であると思われ
る.不可避的に生じ得る創部癒着不良症例に対しては,
HBO 治療が有用であり,今後もさまざまな modality を応
用しながら治療成績の向上に努める必要がある.
本論文の要旨は第 44 回日本脳卒中の外科学会(2015 年 3
月,広島)で発表した.
文
献
1) Andoh T, Sakai N, Yamada H, et al: Chronic subdural hema-toma following bypass surgery─report of three cases. Neu-rol Med Chir(Tokyo) 32: 684-689, 1992
2) Bauer AM, Bain MD, Rasmussen PA: Chronic cerebral isch-emia: where “evidence-based medicine” fails patients. World Neurosurg 84: 714-718, 2015
3) Chou CW, Chang JH, Lin SZ, et al: Extracranial-intracranial (EC-IC)bypass of symptomatic middle cerebral artery (MCA)total occlusion for haemodynamic impairment
pa-tients. Br J Neurosurg 26: 823-826, 2012
4) Dong Y, Teoh HL, Chan BP, et al: Changes in cerebral hemo-dynamic and cognitive parameters after external carotid-in-ternal carotid bypass surgery in patients with severe steno-occlusive disease: a pilot study. J Neurol Sci 322: 112-116, 2012
5) EC/IC Bypass Study Group: Failure of extracranial-intracra-nial arterial bypass to reduce the risk of ischemic stroke. Results of an international randomized trial. N Engl J Med 313: 1191-1200, 1985
6) Esposito G, Durand A, Van Doormaal T, et al: Selective-tar-geted extra-intracranial bypass surgery in complex middle cerebral artery aneurysms: correctly identifying the recipi-ent artery using indocyanine green videoangiography. Neu-rosurgery 71(2 Suppl): ons274-284, 2012
7) Fiedler J, Přibáň V, Skoda O, et al: Cognitive outcome after EC-IC bypass surgery in hemodynamic cerebral ischemia. Acta Neurochir(Wien) 153: 1303-1311, 2011
8) Fischer G, Stadie A, Schwandt E, et al: Minimally invasive superficial temporal artery to middle cerebral artery bypass through a minicraniotomy: benefit of three-dimensional vir-tual reality planning using magnetic resonance angiography. Neurosurg Focus 26: E20, 2009
9) Fluri F, Engelter S, Lyrer P: Extracranial-intracranial arterial bypass surgery for occlusive carotid artery disease. Co-chrane Database Syst Rev: CD005953, 2010
10) Houkin K, Ishikawa T, Yoshimoto T, et al: Direct and indirect revascularization for moyamoya disease surgical techniques and peri-operative complications. Clin Neurol Neurosurg 99 (Suppl 2): S142-145, 1997
11) Ichikawa T, Suzuki K, Watanabe Y: Intra-arterial fluores-cence angiography with injection of fluorescein sodium from the superficial temporal artery during aneurysm surgery: technical notes. Neurol Med Chir(Tokyo) 54: 490-496, 2014 12) Inoue T, Ohwaki K, Tamura A, et al: Postoperative transient
neurological symptoms and chronic subdural hematoma after extracranial-intracranial bypass for internal carotid/middle cerebral atherosclerotic steno-occlusive diseases: negative ef-fect on cognitive performance. Acta Neurochir(Wien) 158: 207-216, 2016
13) Januszewski J, Beecher JS, Chalif DJ, et al: Flow-based evalu-ation of cerebral revascularizevalu-ation using near-infrared indo-cyanine green videoangiography. Neurosurg Focus 36: E14, 2014
14) JET Study Group: Japanese EC-IC Bypass Trial(JET study) ─Study design と中間解析結果.脳卒中の外科 30: 97-100, 2002
15) JET Study Group: Japanese EC-IC Bypass Trial(JET study) ─中間解析結果(第二報).脳卒中の外科 30: 434-437, 2002 16) Joo SP, Kim TS, Seo BR, et al: The clinical utility of the
Kopit-nik arteriovenous malformation microclip during STA-MCA bypass surgery. Acta Neurochir(Wien) 152: 547-551, 2010 17) Kikuta K, Takagi Y, Fushimi Y, et al: “Target bypass”: a
method for preoperative targeting of a recipient artery in superficial temporal artery-to-middle cerebral artery anasto-moses. Neurosurgery 59(4 Suppl 2): ONS320-326, 2006 18) Kuroda K, Kinouchi H, Kanemaru K, et al: Intra-arterial
injec-tion fluorescein videoangiography in aneurysm surgery. Neu-rosurgery 72(2 Suppl): ons141-150, 2013
19) Low SW, Teo K, Lwin S, et al: Improvement in cerebral hemo-dynamic parameters and outcomes after superficial temporal artery-middle cerebral artery bypass in patients with severe stenoocclusive disease of the intracranial internal carotid or middle cerebral arteries. J Neurosurg 123: 662-669, 2015 20) Marshall RS, Festa JR, Cheung YK, et al: Cerebral
hemody-namics and cognitive impairment: baseline data from the RECON trial. Neurology 78: 250-255, 2012
21) Marshall RS, Festa JR, Cheung YK, et al: RECON Investiga-tors: Randomized Evaluation of Carotid Occlusion and Neu-rocognition(RECON) trial: main results. Neurology 82: 744-751, 2014
22) Muroi C, Khan N, Bellut D, et al: Extracranial-intracranial bypass in atherosclerotic cerebrovascular disease: report of a single centre experience. Br J Neurosurg 25: 357-362, 2011 23) Powers WJ, Clarke WR, Grubb RL Jr, et al: COSS
Investiga-tors: Extracranial-intracranial bypass surgery for stroke pre-vention in hemodynamic cerebral ischemia: the Carotid Oc-clusion Surgery Study randomized trial. JAMA 306: 1983-1992, 2011
24) Reynolds MR, Grubb RL Jr, Clarke WR, et al: Carotid Occlu-sion Surgery Study Investigators: Investigating the mecha-nisms of perioperative ischemic stroke in the Carotid Occlu-sion Surgery Study. J Neurosurg 119: 988-995, 2013
25) Rodríguez-Hernández A, Lawton MT: Flash fluorescence with indocyanine green videoangiography to identify the re-cipient artery for bypass with distal middle cerebral artery aneurysms: operative technique. Neurosurgery 70(2 Suppl): 209-220, 2012
26) Sandow N, von Weitzel-Mudersbach P, Rosenbaum S, et al: Extra-intracranial standard bypass in the elderly: periopera-tive risk, bypass patency and outcome. Cerebrovasc Dis 36: 228-235, 2013
27) 佐藤雅美,三宅秩代,宇野昌明,ほか:抗血小板薬中止に伴 う血小板凝集能の変化─脳血管障害による手術の場合.脳卒 中の外科 38: 261-265, 2010
re-duce the risk of haemodynamic stroke in cerebroocclusive atherosclerotic disease of the anterior cerebral circulation─a systematic review. Neurol Neurochir Pol 41: 457-471, 2007 29) Schmiedek P, Piepgras A, Leinsinger G, et al: Improvement of
cerebrovascular reserve capacity by EC-IC arterial bypass surgery in patients with ICA occlusion and hemodynamic cerebral ischemia. J Neurosurg 81: 236-244, 1994
30) Takanari K, Araki Y, Okamoto S, et al: Operative wound-re-lated complications after cranial revascularization surgeries. J Neurosurg 123: 1145-1150, 2015
31) Wada K, Nawashiro H, Arimoto H, et al: Usefulness of an ul-trasonic scalpel to harvest and skeletonize the superficial temporal artery for extracranial-intracranial bypass surgery. Neurosurgery 65(6 Suppl): 141-147, 2009
32) 和田孝次郎,大谷直樹,市川直紀:浅側頭動脈を用いた頭蓋 内血行再建術後頭皮創トラブルに対する高気圧酸素療法の効 果.日高気圧環境・潜水医会誌 50: 80-84, 2015
33) Wilson HD, Wilson JR, Fuchs PN: Hyperbaric oxygen treat-ment decreases inflammation and mechanical hypersensitivi-ty in an animal model of inflammatory pain. Brain Res 1098: 126-128, 2006
34) Woitzik J, Horn P, Vajkoczy P, et al: Intraoperative control of extracranial-intracranial bypass patency by near-infrared in-docyanine green videoangiography. J Neurosurg 102: 692-698, 2005
35) Yasargil MG, Krayenbuhl HA, Jacobson JH 2nd: Microneuro-surgical arterial reconstruction. Surgery 67: 221-233, 1970 36) 米川泰弘,半田 肇:STA-MCA bypass においておこりう
る合併症とその対策.脳卒中の外科研会講集 8: 287-294, 1980 37) Yoshimura S, Egashira Y, Enomoto Y, et al: Superficial tempo-ral artery to middle cerebtempo-ral artery double bypass via a small craniotomy: technical note. Neurol Med Chir(Tokyo) 50: 956-959, 2010