Ⅰ.は じ め に
遠隔モニタリングにより,われわれはデバイスデータを得るのに患者の受診を必要としなくなった.
これにより,デバイス患者の不整脈は早期発見が可能となり,不整脈管理は変化しつつある.本稿では
不整脈管理における遠隔モニタリングの有用性について記載する.
Ⅱ.遠隔モニタリングによる不整脈の早期検出
遠隔モニタリングには,remote interrogation(RI)と remote monitoring(RM)の 2つの管理法がある.
RIは外来受診時のチェックに類似したデバイスデータを定期的にスケジュール送信することをいい,
RMは RIの定期送信に加え,イベント(不整脈やデバイス機能異常)が発生した際にデバイスデータを
自動的にアラート送信するモニタリング機能をいう.これまでに報告されている遠隔モニタリングに関
する研究の多くは RMを用いたものであり,その有用性は AWARE trial
1),TRUST trial
2),COMPAS
trial
3)など,さまざまな臨床研究で証明されている.本稿で述べる遠隔モニタリングは RMを指す.RM
では患者が受診する前に不整脈の情報が得られるため,診察前に治療方針などを検討することも可能で
ある.不整脈管理において早期発見治療ができるこの RMの有用性が特に大きいのは,心房細動(AF)
管理と植込み型除細動器(ICD)管理である.
Ⅲ.遠隔モニタリングを用いた AF管理
1.AFの早期検出の重要性
2030年には我が国の患者数が 100万人を超えるとされる AFは,心原性脳塞栓の最も重要な危険因子
である.心原性脳塞栓の予後は極めて不良であるため,AFの早期発見治療は非常に重要である.AF
既往のないデバイス患者を調査した研究では,デバイス植込み術後 2.5年以内に 10%が AFを新規発症
することがわかっており
4),デバイス患者の管理において AF発症には十分な注意を要する.無症状の
AFは少なからず存在し
5),デバイスの診療期間が数ヵ月ごとである我が国では発見が遅れるため,遠
隔モニタリングが果たす役割は大きい.
2.デバイスによる AFの検出能
デバイスによる心房不整脈の検出は,atrial high rate episode(AHRE)として示される.MOST
studyにて,AHREを認めると高率に AFを発症することがわかっている
6).旧機種では AHREから
国立循環器病研究センター
心臓血管内科部門不整脈科
石橋耕平 岡村英夫
遠隔モニタリングを用いた不整脈管理
タイプ ATPSeq ショック 治療結果 ID# 日付 hh:mm時刻 hh:mm:ss持続時間 平均bpmA/V Max bpmA/V AT/AF AT/AF AT/AF AT/AF AT/AF AT/AF AT/AF 99 98 97 96 95 94 93 14:34:07 :03:31 :04 :03:01 :05 :06 18:13:30 319/97 135/90 109/90 128/95 117/96 104/93 302/93 545/176 250/VP 182/VP 176/VP 176/VP 176/VP 545/182
①
②
①
②
14 分のイベント,EGMでAT/AF
3 分のイベント,EGMでPAC short run
AFを抽出できなかったが,現行機種では可能である.その AF検出能は,Single-chamberシステム
7),
Dual-chamberシステム
8)のいずれも 90%を超える正確性を有する.以上より,デバイスが検出した
AFは基本的に AFとして対応して問題ないが,数分以下の AF検出に関しては期外刺激のショートラ
ンなどを誤認識していることがあるため,注意を要する(図 1).
3.デバイスが検出した AFと抗凝固療法
現在,デバイスが検出した AFに対する我が国における抗凝固療法の取り決めはなく,各医師の判断
に委ねられている.ESCガイドライン 2016では「> 5〜 6分かつ> 180 bpmの AHREを認めた際は
CHA
2DS
2-VASc scoreを使用して oral anticoagulant(OAC)の必要性を検討し,デバイスの心内電位な
どで AFと診断すれば OACを開始する」とされているものの,「OACの有用性に関するすべての情報は
心電図診断に基づいている.AHRE で検出された AF に関する OAC の有用性は不明であり,現在研
究が行われている」とも記載されており,適切な管理法の確立は今後の課題である
9).現時点で参考
と な る基準は,ASSERT trial の CHADS
2score > 2 かつ> 6 分
4),SOS AF project の≧ 1 時間
10),
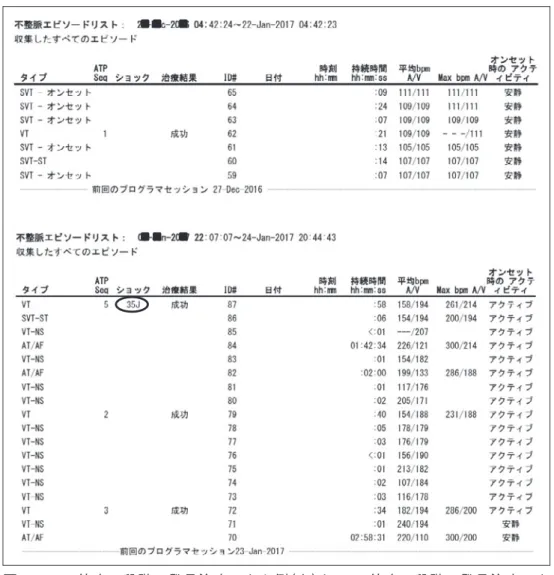
図 2 ATP停止の段階で発見治療できた例(上)と ATP停止の段階で発見治療でき
ずショック治療に至ってしまった例(下)
ASSERT trialサブ解析の> 24時間
11)である.
Ⅳ.遠隔モニタリングを用いた ICD管理
1.VTの早期検出による ICD適切作動の低減
VTはあらゆる心疾患の予後規定因子であるため,早期発見治療は当然のごとく重要であり,遠隔モ
ニタリングが有用であることに異存はない.VTに対する ICD適切作動には抗頻拍ペーシング治療
(ATP)とショック治療があり,ATPは予後に影響しないが,ショック治療は予後不良を起こす
12).
VTの ICD治療設定は,通常,まず初めに ATPを行い,停止しないときにショック治療を行うよう設
ノイズ
図 3 リードノイズによる心室細動検出のアラート送信例
定する.遠隔モニタリングにて ATPで停止した VTを早期発見し介入できれば,ショック作動の低減
につながる(図 2).二次予防植込み患者に対するカテーテルアブレーションは予後を改善するとされて
おり,薬物のみならずアブレーションも選択肢の一つとなる
13).
2.ICD不適切作動の回避
低心機能症例では,ICD不適切作動でショック治療を受けた患者は死亡率が約 2倍になると報告され
ている
14).ICD不適切作動低減の設定(VTの検出 rateを上げる設定や VTの検出を遅らせる設定)の有
用性が報告され
15),一次予防植込み患者を中心に設定されているが,それでもなお不適切作動は年間
数%発生する.主な原因は前述の AFであるが
16),遠隔モニタリングによる AFの早期発見治療は ICD
不適切作動回避にも役立つ.また,リードノイズなども早期発見できれば,ICD不適切作動を回避する
ことができる(図 3).
Ⅴ.ま と め
遠隔モニタリングは,いわば自宅に居ながら不整脈外来診療を受けることのできるシステムであり,
その有用性は疑う余地がない.さらに,通常外来診察時には,不整脈トラブルがほぼ解決済であり,外
来診療の効率化にも役立つ.遠隔モニタリングは今後不整脈管理における必須のシステムとなることが
予想される.
〔文 献〕
1 ) Lazarus A : Remote, Wireless, Ambulatory monitoring of implantable pacemakers, cardioverter defibrillators, and cardiac resynchronization therapy systems : analysis of a worldwide database. PACE, 2007 ; 30 : S2〜 S12
2 ) Varma N, Epstein AE, Irimpen A, Schweikert R, Love C ; TRUST Investigators : Efficacy and safety of automatic remote monitoring for implantable cardioverter-defibrillator follow-up : the lumos-t safely reduces routine office device follow-up (TRUST)trial. Circulation, 2010 ; 122 : 325〜 332
3 ) Mabo P, Victor F, Bazin P, Ahres S, Babuty D, Da Costa A, Binet D, Daubert JC ; COMPAS Trial Investigators : A randomized trial of long-term remote monitoring of pacemaker recipients(the COMPAS trial). Eur Heart J, 2012 ; 33 : 1105〜 1111
4 ) Healey JS, Connolly SJ, Gold MR, Israel CW, Van Gelder IC, Capucci A, Lau CP, Fain E, Yang S, Bailleul C, Morillo CA, Carlson M, Themeles E, Kaufman ES, Hohnloser SH : Subclinical atrial fibrillation and the risk of stroke. N Engle J Med, 2012 ; 366 : 120〜 129
5 ) Lowres N, Neubeck L, Redfern J, Freedman SB : Screening to identify unknown atrial fibrillation. A systematic review. Thromb Haemost, 2013 ; 110 : 213〜 222
6 ) Glotzer TV, Hellkamp AS, Zimmerman J, Sweeney MO, Yee R, Marinchak R, Cook J, Paraschos A, Love J, Radoslovich G, Lee KL, Lamas GA ; MOST Investigators : Atrial high rate episodes detected by pacemaker diagnostics predict death and stroke : report of the atrial diagnostics ancillary study of the mode selection trial(MOST). Circulation, 2003 ; 107 : 1614 〜 1619
7 ) Deshmukh A, Brown ML, Higgins E, Schousek B, Abeyratne A, Rovaris G, Friedman PA : Performance of atrial fibrillation detection in a new single-chamber ICD. PACE, 2016 ; 39 : 1031〜 1037
8 ) Swerdlow CD, Schsls W, Dijkman B, Jung W, Sheth NV, Olson WH, Gunderson BD : Detection of atrial fibrillation and flutter by a dual-chamber implantable cardioverter-defibrillator. For the Worldwide Jewel AF Investigators. Circulation, 2000 ; 101 : 878〜 885
9 ) Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P, Agewall S, Camm J, Baron Esquivias G, Budts W, Carerj S, Casselman F, Coca A, De Caterina R, Deftereos S, Dobrev D, Ferro JM, Filippatos G,
Fitzsimons D, Gorenek B, Guenoun M, Hohnloser SH, Kolh P, Lip GY, Manolis A, McMurray J, Ponikowski P, Rosenhek R, Ruschitzka F, Savelieva I, Sharma S, Suwalski P, Tamargo JL, Taylor CJ, Van Gelder IC, Voors AA, Windecker S, Zamorano JL, Zeppenfeld K : 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J, 2016 ; 37 : 2893〜 2962
10 ) Boriani G, Glotzer TV, Santini M, West TM, De Melis M, Sepsi M, Gasparini M, Lewalter T, Camm JA, Singer DE : Device-detected atrial fibrillation and risk for stroke : an analysis of > 10,000 patients from the SOS AF project(stroke prevention strategies based on atrial fibrillation information from implanted devices). Eur Heart J, 2014 ; 35 : 508〜 516 11 ) Van Gelder IC, Healey JS, Crijns HJGM, Wang J, Hohnloser SH, Gold MR, Capucci A, Lau CP, Morillo CA, Hobbelt AH,
Rienstra M, Connolly SJ : Duration of device-detected subclinical atrial fibrillation and occurrence of stroke in ASSERT. Eur Heart J, 2017 ; 38 : 1339〜 1344
12 ) Sweeney MO, Sherfesee L, DeGroot PJ, Wathen MS, Wilkoff BL : Differences in effects of electrical therapy type for ventricular arrhythmias on mortality in implantable cardioverter-defibrillator patients. Heart Rhythm, 2010 ; 7 : 353〜 360 13 ) Reddy VY, Reynolds MR, Neuzil P, Richardson AW, Taborsky M, Jongnarangsin K, Kralovec S, Sediva L, Ruskin JN,
Josephson ME : Prophylactic catheter ablation for the prevention of defibrillator therapy. N Engle J Med, 2007 ; 357 : 2657〜 2665
14 ) Poole JE, Johnson GW, Hellkamp AS, Anderson J, Callans DJ, Raitt MH, Reddy RK, Marchlinski FE, Yee R, Guarnieri T, Talajic M, Wilber DJ, Fishbein DP, Packer DL, Mark DB, Lee KL, Bardy GH : Prognostic importance of defibrillator shocks in patients with heart failure. N Engle J Med, 2008 ; 359 : 1009〜 1017
15 ) Moss AJ, Schuger C, Beck CA, Brown MW, Cannom DS, Daubert JP, Estes NA 3rd, Greenberg H, Hall WJ, Huang DT, Kautzner J, Klein H, McNitt S, Olshansky B, Shoda M, Wilber D, Zareba W : Reduction in inappropriate therapy and mortality through ICD programming. N Engle J Med, 2012 ; 367 : 2275〜 2283
16 ) Daubert JP, Zareba W, Cannom DS, McNitt S, Rosero SZ, Wang P, Schuger C, Steinberg JS, Higgins SL, Wilber DJ, Klein H, Andrews ML, Hall WJ, Moss AJ : Inappropriate implantable cardioverter-defibrillator shocks in MADIT II : frequency, mechanisms, predictors, and survival impact. J Am Coll Cardiol, 2008 ; 51 : 1357〜 1365