胸腔内胃穿孔と続発性気胸を合併した
遅発性先天性横隔膜ヘルニアの 1 例
橘高 弘忠1,a, 秋元 寛1, 福田 真樹子1, 筈井 寬1,
岡本 雅雄1, 小畑 仁司1, 大石 泰男1
A case of late-presenting congenital diaphragmatic hernia complicated with intrathoracic gastric perforation and secondary pneumothorax
Hirotada Kittaka1, Hiroshi Akimoto1, Makiko Fukuda1, Hiroshi Hazui1,
Masao Okamoto1, Hitoshi Kobata1, Yasuo Ohishi1
要旨 遅発性先天性横隔膜ヘルニアに胸腔内胃穿孔と続発性気胸を合併した閉塞性ショック症例を経験した ので報告する。症例は 14 歳の女児である。某日より心窩部痛・嘔気・嘔吐が出現し持続した。その 5 日後に 突然呼吸苦が出現したため前医を受診し,緊張性気胸の疑いで当センターへ紹介搬送となった。搬入後,ただ ちに左胸腔ドレーンを挿入したところ,エアー排出とともに茶褐色排液を認めた。造影 CT では,腹腔内臓器 の左胸腔内への嵌入と左気胸および腹腔内 free air を認め,縦隔は右方へ偏位していた。以上より,横隔膜ヘ ルニアに胸腔内消化管穿孔を合併した閉塞性ショックを疑い緊急開腹術を行った。開腹すると,左横隔膜背側 に 10cm 大の欠損孔を認め,同部より胃・横行結腸・脾臓が胸腔内へ脱出していた。さらに,胸腔内に脱出し ていた胃体部後壁に 15mm 大の穿孔を認めた。外傷の既往がなかったことから Bochdalek 孔ヘルニアと診断し, 穿孔部を大網充填被覆術で閉鎖後,ヘルニア門を結節縫合で閉鎖した。横隔膜閉鎖後より頻脈が出現し横隔膜 閉鎖部間隙よりエアーの漏出を認めたこと,術前の CT でブラを認めなかったことから,続発性気胸の合併と 診断し,胸腔ドレナージを追加したところ脈拍数は低下した。術後,集中治療により全身状態は改善し,第 49 病日転院となった。本例は胸腔内脱出臓器,胸腔内胃穿孔および続発性気胸によって閉塞性ショックを合 併した症例で,緊張性気胸と同様に迅速な診断と治療開始が求められた症例であった。 (日救急医会誌. 2015; 26: 111-5) キーワード:Bochdalek 孔ヘルニア,閉塞性ショック,緊張性気胸
A-14-year-old female, who complained of continuous nausea and sudden dyspnea, was transferred to our institution. We diagnosed as a tension pneumothorax based on her dynamic state and the findings of X-rays taken at the prior hospital. When a chest tube was inserted, a dark brown-colored fluid with air was drained. Enhanced computed tomography revealed a collection of air in both the abdominal and thoracic cavities, and the herniation of the abdominal organs into the left thoracic cavity. We suspected of a diaphragmatic hernia complicated with intrathoracic intestinal perforation, and performed emergency laparotomy. The intraoperative findings showed the prolapse of the stomach, transverse colon and spleen into the left thoracic cavity through the defect of the left diaphragm. Moreover, a perforation of the stomach was observed. She had no past history of trauma; therefore we diagnosed as Bochdalek hernia complicated with intrathoracic gastric perforation. Although we closed the gastric perforation and the diaphragmatic defect, there was persistent leakage of air from the left thoracic cavity. We diagnosed as a complicated secondary pneumothorax, and inserted an additional chest tube. After the operation she gradually recovered and was then transferred to another hospital on day 49 of hospitalization. (JJAAM. 2015; 26: 111-5)
Keywords: Bochdalek hernia, obstructive shock, tension pneumothorax Received on November 4, 2014 (14-078) はじめに 先天性横隔膜ヘルニア(Congenital Diaphragmatic Hernia: CDH)のうち,生後 30 日以降に診断される ものを遅発性 CDH と呼び,全 CDH の 5〜25%を占 める 1-3)。一般的には新生児発症 CDH と比較して重 1 大阪府三島救命救急センター
Osaka Mishima Emergency Critical Care Center
a 〒651-0073 兵庫県神戸市中央区脇浜海岸通 1-3-1 兵庫県災害医療センター
症化することは少ないとされているが,稀に胸腔内 に脱出した消化管に穿孔を合併して重篤化すること がある。 我々は,胸腔内脱出臓器,胸腔内胃穿孔および続 発性気胸による閉塞性ショックを合併した遅発性 CDH の 1 例を経験したので報告する。 症 例 患 者:14 歳の女児。 主 訴:呼吸苦。 既往歴:特記事項なし。 家族歴:特記事項なし。 現病歴:某月 8 日より心窩部痛・嘔気が出現し近 医を受診した。腹膜刺激症状は認められず,急性胃 炎の診断で H2-blocker の処方を受けたが,その後も 嘔気・嘔吐が持続した。同月 13 日 0 時,胸痛をとも なわない呼吸苦が突然出現したため前医を受診した ところ,橈骨動脈の触知は微弱で脈拍数 160 台/分と
ショック状態であり,SpO2 90%(room air)と低下し
ていた。胸部 X 線レントゲン検査で左気胸を認め, 理学的所見から緊張性気胸と診断され,同日 3 時当 センターへ紹介搬送となった。 搬入時現症:血圧 90/60mmHg,脈拍数 172/分, 呼吸回数 24/分,SpO2 99%(10L/分リザーバー付き 酸素マスク下),体温 36.0°C,意識レベル Japan Coma Scale 0 であった。頸部・胸部の皮下気腫や気管偏位 はなかったが,頸静脈は軽度怒張し,左胸郭の挙上 不良と同側呼吸音の減弱および胸部打診で鼓音を認 めた。腹部全体に筋性防御・反跳痛をともなう強い 圧痛を認めた。 搬入時血液検査結果:白血球数 16,000/μL(後骨髄 球 3%,桿状核球 25%)と著明な左方移動を認めた。 また,BUN 58mg/dL,Cr 2.30mg/dL と腎機能障害をと もなっており,血糖値は 432mg/dL と著明に上昇して いた。血小板数は 38.7×104/μL と正常範囲内であっ たが,PT-INR 1.52,D-dimer 7.8μg/mL と凝固障害を 認め,急性期 DIC スコアは 3 点であった。 動脈血液ガス検査結果(経鼻 3L/分酸素投与下):
pH7.11,PaCO2 23.2mmHg,PaO2 99.1mmHg,HCO3
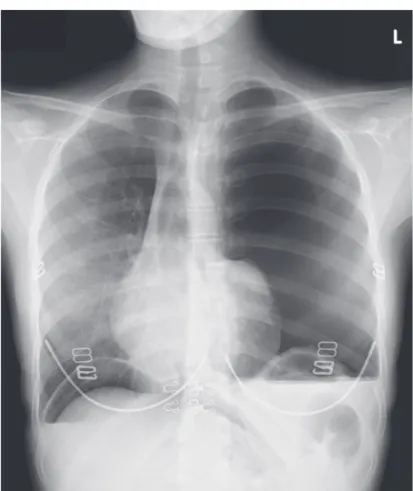
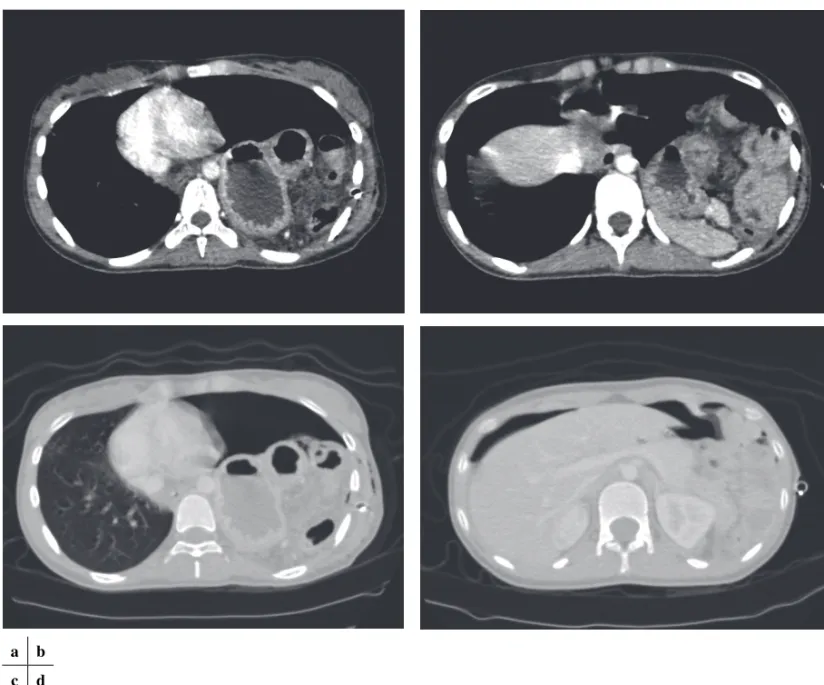
7.2mmol/L,Base excess 20.4,Lactate 7.45mmol/L と 代謝性アシドーシスを認めた。 前医胸部 X 線レントゲン所見(Fig. 1):左肺内に 大量のエアーと心陰影の狭小化および縦隔の右方偏 位を認めた。右横隔膜下に腹腔内遊離ガスを認めた。 理学的所見・画像所見より左緊張性気胸と診断し, 左第 5 肋間腋窩中線より 16 Fr.トロッカーを挿入した ところ,エアー排出とともに 900mL の茶褐色排液を 認めた。その後も収縮期血圧 90mmHg 台,脈拍数 130 回台 /分とショック状態の改善が得られなかったた め,ただちに造影 CT 撮影を行った。 胸腹部造影 CT 検査所見(Fig. 2):左胸腔内に胃・ 脾臓・横行結腸が嵌入しており,腹腔内の free air と 左気胸を認めた。縦隔は右方へ偏位していた。 過去に外傷の既往がなかったことより,CDH に胸 腔内消化管穿孔を合併した閉塞性ショックを疑い, 搬入から 3 時間後に緊急開腹術を行った。 術中所見(Fig. 3):左横隔膜の左背側に 10cm 大の
Fig. 1. A chest X-ray showed a massive air collection in the left
Fig. 2. Enhanced computed tomography revealed a prolapse of the stomach, transverse colon and spleen into the left thoracic cavity (a / b), and a collection of air in both the abdominal and left thoracic cavities, with displacement of the mediastinum to the right (c /d).
a b c d
Fig. 3. The intraoperative findings showed a defect located in the left-back position of the left diaphragm measuring 10cm in diameter
(white arrow), through which the stomach, transverse colon and spleen prolapsed into the thoracic cavity (a). A perforation in the posterior wall of the stomach measuring 15mm in diameter was observed (white arrow head) (b).
裂孔を認め,Bochdalek 孔ヘルニアと診断した。同部 より胃・脾臓・横行結腸脾彎曲部が左胸腔内へ脱出 し嵌頓していたが,胸腔内臓器との癒着はなく用手 的還納は容易であった。胸・腹腔内には茶褐色の腸 液様腹水が多量に貯留していた。胸腔内に脱出して いた胃体上部後壁に虚血・壊死性変化をともなわな い 15mm 大の穿孔を認めたため,大網充填被覆にて 閉鎖した。横隔膜欠損部を吸収糸にて結節縫合で閉 鎖後より頻脈が出現した。横隔膜縫合部の間隙より エアーの漏出を認めたことから,続発性気胸の合併 と診断し,左第 4 肋間腋窩中線より 24 Fr. 胸腔ド レーンを追加挿入したところ,air の排出とともに頻 脈は改善した。左横隔膜下にドレーンを 1 本留置し て手術を終了した。手術時間は 2 時間 56 分で搬入 から手術終了までの 6 時間で細胞外液 6,200mL を投 与した。 術後経過:気管挿管のまま ICU へ入室し人工呼吸 器管理を継続した。術直後の胸部 X 線レントゲン検 査で縦隔偏位の改善にもかかわらず循環不全が遷延 していたこと,搬入時の血液検査で腎機能障害と高 血糖を認めていたことから,重症敗血症の合併と診 断し,ノルアドレナリンの持続投与およびヒドロコ ルチゾン(100mg×3 回/日)と乾燥スルホ化人免疫グ ロブリン(0.5g/日×3 日)の投与を開始した。術中に 採取した胸腔内貯留液のグラム染色検査で貪食像を ともなう真菌が検出されたため,抗菌薬には BIPM (0.3g×3 回/日)と F-FLCZ(0.2g×1 回/日)を選択し た。また,PaO2/ FIO2比が 220 と低値であったため急 性呼吸促迫症候群と診断し,シべレスタットナトリ ウム(250mg/日)の持続投与も行った。その後,呼 吸状態・循環動態は徐々に改善し,第 4 病日に人工 呼吸器から離脱し,同日より飲水・食事を開始した。 術前に採取した血液培養検査で Candida albicans が検 出された。胸腔ドレーンは,エアーリーク・排液と もに認められなくなったため,第 4・第 9 病日に各々 抜去した。その後左膿胸を合併し再ドレナージ・⻑ 期抗生剤投与を要したが,徐々に改善し,第 49 病日 に転院となった。 考 察 遅発性 CDH には,平常時はヘルニア門からの臓 器脱出がなくヘルニア嚢の破裂もしくは腹腔内臓器 が急激に胸腔内に脱出して発症するものと,元々脱 出していた臓器に穿孔・絞扼などが合併して発症す るものと 2 つのタイプがある 2)。自験例は,過去の胸 部 X 線レントゲン写真が入手できなかったためいず れのタイプかは確定できないが,術中所見で慢性的 脱出を示唆する脱出臓器とヘルニア門や胸腔内臓器 との癒着を認めなかったことから,前者のタイプで あった可能性が高いと考えた。急激な腹腔内臓器脱 出の誘因として啼泣 3),イレウス 4),妊娠 5)による腹 圧上昇が報告されているが大部分は原因不明である。 自験例でも外傷など含めて腹圧上昇を来すような病 歴はなかったが,咳嗽や排便時の怒責などの軽微な 腹圧上昇が関与した可能性は否定できない。胃・脾 臓・結腸が急激に胸腔内へ脱出・牽引されて初発症 状の心窩部痛・嘔気が生じ,さらに胃の通過障害と それによって生じた持続性嘔吐が著明な胃内圧上昇 を誘発して穿孔に至ったものと考えた。 CDH や外傷性横隔膜損傷に胸腔内消化管穿孔を合 併して閉塞性ショックとなった報告は散見されるの みである 6-10)。いずれも脱出腸管と穿孔部からリー クした消化管ガスが縦隔圧排の原因であり,自験例 も手術前は同様の機序による閉塞性ショックを疑っ た。しかし,胃穿孔部閉鎖後も胸腔内からのエアー リークが持続したこと,術前の CT でブラを認めな かったことから続発性気胸と診断し,これも閉塞性 ショックの大きな一因と考えた。医学中央雑誌で検 索したところ,本邦における遅発性 CDH に胸腔内胃 穿孔合併した症例は 6 例のみ 11-16)で,肺への穿通に より肺瘻を生じた報告 13)はあるが,続発性気胸を合 併した報告はなかった。自験例では胃穿孔部と肺の 癒着がなかったことから穿通による気胸発生は否定 的であり,Bini ら 17)が報告しているように,胸腔内 で漏出した胃液の腐食作用が続発性気胸の原因と考 えた。
遅発性 CDH が劇症化する原因として,胸腔内消化 管穿孔のほかに,大量の脱出腸管が縦隔を圧排して閉 塞性ショックを呈し短時間のうちに死に至る tension gastrothorax が挙げられる 3)。tension gastrothorax の胸
部 X 線レントゲン写真所見は胸腔内の腸管ガスに よって気胸と類似した所見を呈するため,自験例と 同様に CT 前に胸腔ドレナージが行われることも少 なくない 2, 3, 6, 7, 10, 18)。tension gastrothorax に対する治療 は経鼻胃管挿入による胃内減圧が第一選択であるが, ヘルニア門での狭窄のため胃管挿入が困難なことも 多く,古川ら 3)は切迫した症例では胸腔穿刺時に胃壁 を貫通させて胃内減圧を図ることもやむをえないと している。自験例は典型的な tension gastrothorax で はないが,胸腔内脱出臓器,穿孔部から漏出した胃 ガスおよび続発性気胸による胸腔内圧上昇から閉塞 性ショックを合併した症例であり,緊張性気胸と同 様に迅速な診断と治療開始が求められた症例であっ た。 結 語 遅発性 CDH は稀な疾患であるが,胸腔内消化管穿 孔や続発性気胸の合併によって急激に重症度・緊急 度ともに高くなるため,迅速な診断と治療が必要で ある。 利益相反なし。 文 献
1) Baglaj M: Late-presenting congenital diaphragmatic hernia in children: a clinical spectrum. Pediatr Surg Int. 2004; 20: 658-69.
2) Berman L, Stringer D, Ein SH, et al: The late-presenting pediatric Bochdalek hernia: a 20-year review. J Pediatr Surg. 1988; 23: 735-9. 3) 古川泰三, 木村修, 樋口恒司, 他: 当院における遅発性 先天性横隔膜ヘルニア症例の検討. 日小外会誌. 2013; 49: 975-80. 4) 勝原和博, 高野信二, 上田重春, 他: 胸腔内で大腸穿孔 を来した横隔膜ヘルニアの 1 例. 日臨外会誌. 2008; 69: 2518-22. 5) 陳祝労, 高宮淑子, 根来孝夫, 他: 先天性横隔膜ヘルニ ア合併妊娠 2 症例からの考察. 産と婦. 1987; 54: 413-6. 6) Granier V, Coche E, Hantson P, et al: Intrathoracic caecal
perforation presenting as dyspnea. Case Rep Med. 2010; 2010: 296730.
7) Maa J, Lubbock C, Harrison M, et al: Perforated ulcer mimicking a spontaneous pneumothorax in a patient with congenital diaphragmatic hernia. Am Surg. 2009; 75: 354-6. 8) Roberts CM, Gelder CM, Goldstraw P, et al: Tension
pneumothorax and empyema as a consequence of gastro-pleural fistulae. Respir Med. 1990; 84: 253-4.
9) Schwab RJ, Jarvik JG: Tension pneumothorax secondary to a gastropleural fistula in a traumatic diaphragmatic hernia. Chest. 1991; 99: 247-9.
10) Yutaka Y, Katakura H, Noguchi S, et al: Tension pneumothorax with empyema from gastric ulcer perforation. Postgrad Med J. 2012; 88: 113-4. 11) 吉田秀明, 枝澤寛, 野納邦昭, 他: 結腸の完全断裂をき たした成人 Bochdalek 孔ヘルニアの 1 例. 日臨外会誌. 2001; 62: 929-33. 12) 吉敷智和, 志田晴彦, 根岸真人, 他: 脱出胃の穿孔によ り気胸・膿胸を呈した横隔膜ヘルニアの 1 例. 日臨外会 誌. 2006; 67: 1533-6. 13) 児玉泰一, 太田裕之, 塚山正市, 他: 胸腔内で胃穿孔し た成人 Bochdalek 孔ヘルニアの 1 例. 日臨外会誌. 2013; 74: 52-6. 14) 小倉淳司, 井上昌也, 岡田禎人, 他: Bochdalek 孔に嵌頓 した胃の穿孔によると思われた膿胸の 1 例. 日臨外会誌. 2014; 75: 1532-6. 15) 諏訪宏和, ⻑堀優, 高橋徹也, 他: 胃穿孔による汎発性 胸・腹膜炎を伴った成人 Bochdalek 孔ヘルニアの 1 救命 例. 日消外会誌. 2010; 43: 1212-7. 16) 服部正興, 玉内登志雄, 久世真悟, 他: 胸腔内で胃穿孔 をおこした成人 Bochdalek 孔ヘルニアの 1 例. 日臨外会 誌. 2006; 67: 1537-40.
17) Bini A, Grazia M, Petrella F, et al: Spontaneous biliopneumothorax (thoracobilia) following gastropleural fistula due to stomach perforation by nasogastric tube. Ann Thorac Surg. 2004; 78: 339-41.
18) Hamid R, Baba AA, Shera AH, et al: Late-presenting congenital diaphragmatic hernia. Afr J Paediatr Surg. 2014; 11: 119-23.