慈恵
ICU勉強会
2016.8.23
奥井 聖子
Crit Care Med. 2016 Jul;44(7):1395-405.
1.過去
ストレス性潰瘍予防の歴史
2.現在
頻度
PPI vs. H2RA
(
RCT、メタ解析、大規模観察研究)
有害作用(
C.D.感染、肺炎、血小板減少症)
危険因子
コスト
ガイドライン
3.未来
進行中の研究
4.まとめ、私見
目次
1842年 Thomas Blizard Curlingが小児の熱傷患者12例の消化管穿孔を報告
1841年 Carl Rokitanskyにより小児頭蓋内腫瘍患者の消化管穿孔を報告
1932年 Harvey Cushingが脳腫瘍手術後患者の消化管穿孔を報告
ストレス潰瘍予防の歴史
中枢神経系と消化性潰瘍との関係を病理学の観点からも考察
↓
ストレス潰瘍の概念を提唱
Neurosurgery 68:1695–1698, 2011
2011年7月12日勉強会「ストレス性潰瘍予防」改変
1969年
Stress ulcer, acute erosive gastritis and the gastric mucosal barrier
surgical ICUおける呼吸不全, 低血圧, sepsis, 黄疸に関連した胃潰瘍症例8例
を報告。生存者は
8例中1例のみ
Am J Surg 1969; 117(4): 523-53
1978年
Antacid titration in the prevention of acute gastrointestinal bleeding: a
controlled, randomized trial in 100 critically ill patients
NEJM 1978
May 11;298(19):1041-5
同グループによる
RCT 制酸薬の有無と消化管出血との関係を検証
制酸薬
(+) vs. (-):: 2/51(4%) vs. 12/49 (25%) (p<0.005)
→ 制酸薬により消化管出血が減少
1969~1989年
SUPに関するRCT44件
ストレス潰瘍予防の歴史
2011年7月12日勉強会「ストレス性潰瘍予防」参照
Stress ulcer prophylaxis in the critically ill: A meta-analysis
D J Cook et al, Am J Med 1991 Dec;91(6): 670
SUPに関するRCT42件のメタ分析
重症患者における
SUPの効果(消化管出血,死亡率)を検証
明らかな消化管出血発生率
制酸薬
vs. no prophylaxis OR 0.40 (95%CI: 0.20-0.79),
H2RA vs. no prophylaxis
OR 0.29 (95% CI 0.17-0.45)
制酸薬
vs. 胃粘膜保護薬 OR 0.65 ( 95%CI 0.16-2.49)
H2RA vs.制酸薬
OR 0.56 (95% CI 0.33-0.97)
制酸薬,胃粘膜保護薬,
H2RAの使用により消化管出血の発生率低下
死亡率
明らかな減少は認められなかった
1980年代にはSUPが広く行われ,消化管出血を予防
2011年7月12日勉強会「ストレス性潰瘍予防」参照
Stress Ulcer Prophylaxis(SUP)
SUP
出血の頻度
危険因子
比較効果
有害作用
コスト
.
・重症患者での粘膜障害の頻度は
75−100%、顕性出血は
約
5-25%で起こる。
Alhazzani W et al:Pol Arch Med Wewn 2012; 122:107–114
・
1980年代のRCTではcritically important bleeding(CIB)は
全体の
1.5−8.5%、予防を行わない患者では15%に生じていた。
・
1999年以前の研究ではCIBの頻度は2−6%
Am J Health Syst Pharm 1999; 56: 347–379.
・
2000年以降では、CIBの頻度は0.1−4%程度とされる。
Intensive Care Med 2003; 29: 1306–1313
消化管出血の頻度
ここ
20年ほどで、ICU管理などにより
ストレス性潰瘍の発生率は減少してきている。
危険因子
・大規模観察研究、
2252人のICU患者。
48時間以上の人工呼吸器管理、凝固異常がCIBの危険因子
Cook DJ : N Engl J Med 1994; 330:377–381
・
1077人、人工呼吸器患者を対象にしたRCT。
リスク因子は血清
Cr > 5.68 mg/dl。(RR:1.16; 95%CI, 1.02-1.32 )
【
Design】多施設、前向きコホート研究
【
Patients】11カ国97ICUに入室した18歳以上の患者1034名
【
outcome】
・
primary outcome :臨床的に重要な消化管出血
・
secondary outcome:顕性消化管出血、90日以内の死亡率
重症患者の消化管出血の頻度、危険因子について検討
臨床的に重要な消化管出血:
27/1034(2.6%)
顕性出血:
49/1034(4.7%)
73%が制酸剤の投与をうけていた PPI(55%)vsH2RA(17%)
調整オッズ比では臨床的消化管出血は
90日死亡率と有意な関係なし。
Adjusted OR1.70(0.64-4.28)
結果
CIBの発生日時
死亡率
CIBは27人/1037人(2.6%)
そのうち約半数(
13人)が
ICU入室48時間以内に発症
結果 危険因子
臓器不全スコア高値
:
OR 1.4(1.2−1.6)
肝疾患の既往
:
OR 7.6(3.3−17.5)
凝固障害の既往
:
OR 5.2(2.29−11.8)
3つ以上の共存疾患
:
OR 8.9(2.7−28.8)
RRT:OR 6.9(2.7−17.5)
急性凝固機能障害
:
OR 4.2(1.7−10.2)
その他、小規模な研究では・・・
・脊髄損傷、
・外傷性脳損傷(
GCS<10)
・熱傷(面積
>35%)
・敗血症
・肝部分切除、
・肝臓
or腎移植
・アルコール乱用
・
1週間以上のICU滞在、
・
6日以上の潜在性or明らかな出血
・高容量のコルチコステロイド
などを危険因子とする論文も
。
PPI
使用率
コホート研究
PPI
H2RA
1990-91年
0.3%
71.8%
NEJM 1994 ; 330 : 377-381
2004-07年
81%
29%
Arch Intern Med 2011; 171: 991-997
サーベイランス
PPI
H2RA
1998年
3%
77%
Crit Care 1999; 3: 145-49
2002年
26%
64%
Crit Care Med 2004; 32(10): 2008-13
2007年
20%
67%
Anesthesia 2007; 62: 412-23
2014年
59%
25%
J Crit Care 2014; 29:955–960
2011年7月12日勉強会「ストレス性潰瘍予防」改変
PPIの使用頻度
・
USAとカナダの報告ではICU患者の84%にSUPが行なわれてい
る。
J Crit Care 2014; 29:955–960
1990年頃から多くのPPI vs. H2RAのRCTが行なわれてきたが、CIBを
primary endpointにした論文は少ない。
・
67人のICU患者。CIBの頻度はH2RAと比較してPPIで有意に低い
(
6% vs. 31% p<0.05)。
Levy MJ, Seelig CB, Robinson NJ, et al: Dig Dis Sci 1997; 42:1255–1259
・外傷、術後の成人
ICU患者ではSUP群(PPIとH2RA)、非SUP群(スク
ラルファート、プラセボ)に有意差なし。(
1%,3%,4%,1% p>0.05)
Kantorova I, Svoboda P, Scheer P, et al: Hepatogastroenterology 2004; 51:757–761
・
129人ICU患者。PPIとH2RAでCIBの発生率に有意差なし。
(
1.6% vs 5.9%)
Solouki M, Marashian S, Kouchak M: Tanaffos 2009; 8:37–42
Randomized, double-blind comparison of immediate-release omeprazole oral
suspension versus intravenous cimetidine for the prevention of upper
gastrointestinal bleeding in critically ill patients
Crit Care Med 2005 ; 33 : 760-765
PPIとH2RAとで,上部消化管出血予防効果と胃内pHを比較検討
Design: prospective, randomized, double-blinded trial
Setting: アメリカのICU 47施設
Patients: 48時間以上の人工呼吸管理を必要とするICU患者 359人
Intervention: omeprazole; 初回40mgx2, 翌日40mg x1 (oral or N-G)
cimetidine; 300 mg bolus, 50 mg/hr
14日間治療
PPI vs. H2RA
2011年7月12日勉強会「ストレス性潰瘍予防」参照
2011年7月12日勉強会「ストレス性潰瘍予防」改変
PPI群で顕性出血は有意に減少するが
臨床的に重要な消化管出血では有意差なし。
臨床的に重要な消化管出血
PPI vs. H2RA: 7/178
(3.9%) vs. 10/81 ( 5.5%)
→有意差なし
顕性出血
PPI vs. H2RA: 34/178 (19.1%) vs.
58/181 ( 32.0%) (p=0.005)
→PPI群で有意に減少
結果
消化管出血
14RCT、1720名
PPIがCIBを有意に減少させる
RR0.36(0.19−0.68 p=0.002)
13RCT、1587名
PPIがCIBを有意に減少させる
OR0.30( 0.17-0.54)
7RCT、936名
PPI vs. H2RAでCIBに有意差なし
Pooled risk difference -0.04(-0.09-0.1)
3RCT、569名
PPIがCIBを有意に減少させる
OR 0.42(0.20−0.91)
メタ解析
PPI vs. H2RA
Proton Pump Inhibitors Versus Histamine2 Receptor Antagonists for
Stress Ulcer Prophylaxis in Critically Ill Patients: A Systematic Review
and Meta-Analysis
Crit Care Med 2013; 41:693–705
ICU患者において上部消化管出血予防としてのPPIとH2RAを比較した
メタアナリシス
Methods : MEDLINE、EMBASEなどで検索した1200以上の文献から
14のRCTを選択
Patients : 成人のICU入室患者1720例
Outcome :
・
Primary outcome
clinically important upper gastrointestinal bleeding
overt upper gastrointestinal bleeding
・
Secondary outcome
院内肺炎、
CD感染、ICU死亡率、ICU滞在期間
2014年7月22日勉強会「H2ブロッカー vs PPI」参照
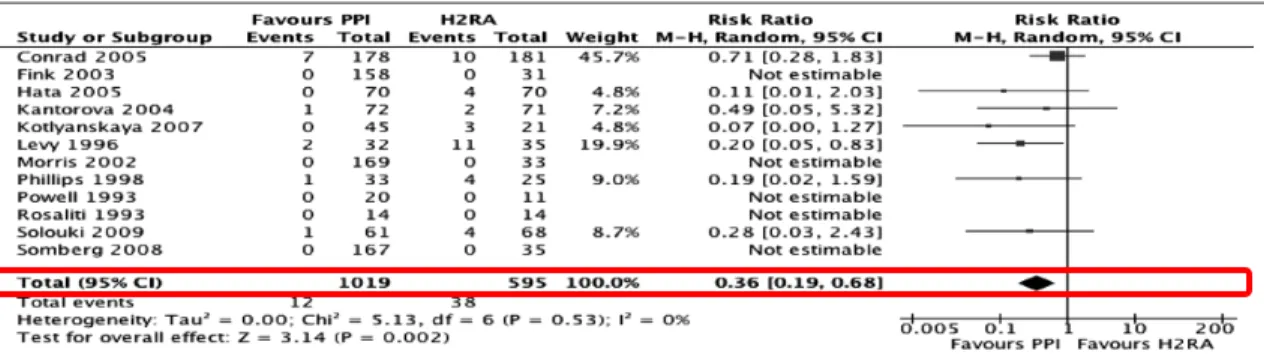
臨床的に重要な消化管出血
→
PPIがbetter (RR:0.36(95%CI:0.19–0.68), p =0.002, I
2
= 0%)
顕性出血
→
PPIがbetter (RR:0.35(95%CI 0.21–0.59), p <0.0001, I
2
=15%)
Proton Pump Inhibitors Versus Histamine2 Receptor Antagonists for
Stress Ulcer Prophylaxis in Critically Ill Patients: A Systematic Review
and Meta-Analysis
Crit Care Med 2013; 41:693–705
Alhazzani et al
700 www.ccmjournal.org -ARCH
Sensitivity Analysis
Sensitivity analysis was conducted examining the effect of
using risk difference as an estimate of effect for clinically
im-portant bleeding (risk difference −0.03; 95% CI −0.05 to 0.00,
p = 0.06, I
2= 52%) and overt bleeding (risk difference −0.06;
95% CI −0.11 to −0.02, p = 0.009, I
2= 80%), although
signifi-cant heterogeneity was present. The second sensitivity analysis
excluded trials pub lished in abstract form (22–25). Clinically
important bleed ing (RR 0.42; 95% CI 0.21–0.84; p = 0.01;
I
2= 0%) and overt bleeding (RR 0.40; 95% CI 0.25–0.67;
p = 0.0004; I
2= 12%) were significantly reduced, consistent
with the main analysis.
DISCUSSION
In this meta-analysis, we found that PPIs were more effective than
H2RAs at preventing clinically important bleeding and overt
gastrointestinal bleeding. The main reservation about using PPIs
Figure 4. Forrest plot for clinically important gastrointestinal bleeding outcome. Data from 12 trials were included in the analysis using random effects
model. The use of proton pump inhibitor (PPI) was associated with a significantly lower risk of clinically important bleeding compared with histamine 2 receptor antagonist (H2RA) (risk ratio [the same as relative risk] [RR] 0.36; 95% confidence interval [CI] 0.19–0.68). M-H = Mantel Haenszel.
TABLE 3. Evidence Profile Using GRADE Approach
Quality Assessment No. of Patients Effect
Quality Impor-tance No. of
Stud-ies Design Risk of Bias Inconsistency Indirectness Imprecision Proton Pump Inhibitor Receptor AntagonistHistamine 2 Confidence Interval)Relative (95% Absolute
Clinically important bleeding 12 Randomized
trials Serious
a No serious
inconsistency indirectnessNo serious imprecisionSerious b 12/1019 (1.2%) 38/595 (6.4%) RR 0.36 (0.19–0.68) 46 fewer per 1000 (from 23 fewer to 58 fewer) Low Critical
Overt upper gastrointestinal bleeding 14 Randomized
trials Serious
a No serious
inconsistency indirectnessNo serious imprecisionNo serious 41/1077 (3.8%) 101/643 (15.7%) RR 0.35 (0.21–0.59) 113 fewer per 1000 (from 72 fewer to 138 fewer) Moderate Important Mortality
8 Randomized
trials Serious inconsistencyNo serious indirectnessNo serious imprecisionNo serious 127/726 (17.5%) 100/470 (21.2%) RR 1.01 (0.83–1.24) 0 fewer per 1000 (from 42 fewer to 51 more) Moderate Critical Nosocomial pneumonia
8 Randomized
trials Serious
a No serious
inconsistency indirectnessNo serious imprecisionNo serious 66/626 (10.5%) 50/474 (10.5%) RR 1.06 (0.73–1.52) 6 more per 1000 (from 28 fewer to 55 more) Moderate Critical
This table is generated using the GRADEprofiler software that summarizes the quality of evidence for individual outcomes based on five main domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. For each outcome, the quality of evidence is presented along with the clinical importance of the outcome.
aDowngraded for risk of bias mainly due to lack of or incomplete blinding.
bDowngraded for low number of events rather than confidence interval. Feature Article
Critical Care Medicine www.ccmjournal.org 701
in the critical care setting rather than H2RAs is the potential to increase the incidence of nosocomial pneumonia (38, 39); how-ever, trials do not suggest such a difference. Mortality and length of ICU stay were not affected. None of the trials reported C. dif-ficile infection, although a systematic review of 12 observational studies evaluating 2,948 patients with C. difficile found an asso-ciation with antisecretory therapy (OR 1.94; 95% CI 1.37–2.75).
The association was present for PPI use (OR 2.05; 95% CI 1.47–2.85) and for H2RA use (OR 1.47; 95% CI 1.06–2.05), with no difference between PPIs and H2RAs (p = 0.17) (40).
There was no heterogeneity of results in this meta-analysis. Subgroup analyses examining dosing and frequency of PPI administration, and specific populations (medical vs. surgical ICU patients, and Asian vs. non-Asian patients) showed no
sig-Figure 5. Forrest plot for overt upper gastrointestinal bleeding outcome. Data from 14 trials were included in the analysis using random effects model.
The use of proton pump inhibitor (PPI) was associated with a significantly lower risk of overt bleeding compared with histamine 2 receptor antagonist (H2RA) (risk ratio [the same as relative risk] [RR] 0.35; 95% confidence interval [CI] 0.21–0.59). M-H = Mantel Haenszel.
TABLE 3. Evidence Profile Using GRADE Approach
Quality Assessment No. of Patients Effect
Quality Impor-tance No. of
Stud-ies Design Risk of Bias Inconsistency Indirectness Imprecision Proton Pump Inhibitor Receptor AntagonistHistamine 2 Confidence Interval)Relative (95% Absolute
Clinically important bleeding 12 Randomized
trials Serious
a No serious
inconsistency indirectnessNo serious imprecisionSerious b 12/1019 (1.2%) 38/595 (6.4%) RR 0.36 (0.19–0.68) 46 fewer per 1000 (from 23 fewer to 58 fewer) Low Critical
Overt upper gastrointestinal bleeding 14 Randomized
trials Serious
a No serious
inconsistency indirectnessNo serious imprecisionNo serious 41/1077 (3.8%) 101/643 (15.7%) RR 0.35 (0.21–0.59) 113 fewer per 1000 (from 72 fewer to 138 fewer) Moderate Important Mortality
8 Randomized
trials Serious inconsistencyNo serious indirectnessNo serious imprecisionNo serious 127/726 (17.5%) 100/470 (21.2%) RR 1.01 (0.83–1.24) 0 fewer per 1000 (from 42 fewer to 51 more) Moderate Critical Nosocomial pneumonia
8 Randomized
trials Serious
a No serious
inconsistency indirectnessNo serious imprecisionNo serious 66/626 (10.5%) 50/474 (10.5%) RR 1.06 (0.73–1.52) 6 more per 1000 (from 28 fewer to 55 more) Moderate Critical
This table is generated using the GRADEprofiler software that summarizes the quality of evidence for individual outcomes based on five main domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. For each outcome, the quality of evidence is presented along with the clinical importance of the outcome.
aDowngraded for risk of bias mainly due to lack of or incomplete blinding. bDowngraded for low number of events rather than confidence interval.
・出血の定義は様々
・
SUPの方法、期間等も様々
・
high qualityの研究では
治療効果が小さい。
Proton Pump Inhibitors Versus Histamine2 Receptor Antagonists for
Stress Ulcer Prophylaxis in Critically Ill Patients: A Systematic Review
and Meta-Analysis
Crit Care Med 2013; 41:693–705
Alhazzani et al
702 www.ccmjournal.org -ARCH
Figure 6. Forrest plot for nosocomial pneumonia outcome. Data from eight trials were included in the analysis using random effects model. The risk of
nosocomial pneumonia was similar in both groups risk ratio [the same as relative risk] [RR] 1.06; 95% confidence interval [CI] 0.73–1.52). H2RA = hista-mine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 7. Forrest plot for ICU mortality outcome. Data from eight trials were included in the analysis using random effects model. The risk of death
dur-ing the ICU stay was similar in both groups (risk ratio [the same as relative risk] [RR] 1.01; 95% confidence interval [CI] 0.83–1.24). H2RA = histamine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 8. Forrest plot for ICU length of stay outcome. Data from five trials were included in the analysis using random effects model. There was no
statistically significant difference between groups (weighted mean difference −0.54; 95% confidence interval [CI] −2.20 to 1.13). H2RA = histamine 2 receptor antagonist; PPI = proton pump inhibitor.
Alhazzani et al
702 www.ccmjournal.org -ARCH
Figure 6. Forrest plot for nosocomial pneumonia outcome. Data from eight trials were included in the analysis using random effects model. The risk of
nosocomial pneumonia was similar in both groups risk ratio [the same as relative risk] [RR] 1.06; 95% confidence interval [CI] 0.73–1.52). H2RA = hista-mine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 7. Forrest plot for ICU mortality outcome. Data from eight trials were included in the analysis using random effects model. The risk of death
dur-ing the ICU stay was similar in both groups (risk ratio [the same as relative risk] [RR] 1.01; 95% confidence interval [CI] 0.83–1.24). H2RA = histamine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 8. Forrest plot for ICU length of stay outcome. Data from five trials were included in the analysis using random effects model. There was no
statistically significant difference between groups (weighted mean difference −0.54; 95% confidence interval [CI] −2.20 to 1.13). H2RA = histamine 2 receptor antagonist; PPI = proton pump inhibitor.