Duration of androgen deprivation therapy and nadir of testosterone at 20 ng/dL predict testosterone recovery to supracastrate level in prostate cancer patients who received external beam radiotherapy
(放射線治療後前立腺癌患者においてホルモン治療期間およびテス トステロン最低値 20ng/dL がテストステロン値の去勢域以上への回 復を予測する) 千葉大学大学院 医学薬学府 先端医学薬学専攻 (主任:市川 智彦 教授) 武井 亮憲
Objectives: To determine the predictors of testosterone recovery after
termination of androgen deprivation therapy in high/intermediate-risk prostate cancer patients receiving external beam radiation therapy with neoadjuvant and adjuvant androgen deprivation therapy.
Methods: A total of 82 patients who underwent external beam radiation
therapy with androgen deprivation therapy for prostate cancer were retrospectively analyzed. Serum testosterone levels after androgen deprivation therapy terminations were studied. Cox proportional hazard models and the Kaplan–Meier method were used for statistical analysis.
Results: Median age, baseline testosterone, nadir testosterone and duration
of androgen deprivation therapy were 73 years, 456 ng/dL, 16 ng/dL and 26 months, respectively. Androgen deprivation therapy duration of 33 months (hazard ratio 0.13; P = 0.0018), nadir testosterone of 20 ng/dL (hazard ratio 0.35; P = 0.0112) and testosterone >50 ng/dL at 6 months after androgen deprivation therapy termination (hazard ratio 0.21; P = 0.0075) were significantly associated with testosterone recovery to normal levels (200 ng/dL) on multivariate analysis. Androgen deprivation therapy duration of 33 months (hazard ratio 0.31; P = 0.0023) and nadir testosterone of 20 ng/dL (hazard ratio 0.38; P = 0.0012) were significantly associated with testosterone recovery to the supracastrate level (50 ng/dL) on multivariate analysis. After dividing patients into three risk groups, the rate of testosterone recovery to the normal level after 2 years of androgen deprivation therapy termination was 100% in the low-risk group versus 20.8% in the high-risk group (P < 0.0001); the rate of testosterone recovery to the supracastrate level was 100% in the low-risk group versus 51.5% in the high-risk group (P < 0.0001).
Conclusions: Duration of androgen deprivation therapy and achievement
of nadir testosterone 20 ng/dL both predict testosterone recovery to the supracastrate level in prostate cancer patients undergoing external beam radiation therapy with androgen deprivation therapy.
Key words: androgen deprivation therapy, nadir testosterone, prostate cancer, radiation therapy, testosterone recovery
Introduction
ADT is a well-established therapy for patients with metastatic PC. (1, 2) ADT is used in radiotherapy for the management of PC. Past studies showed that the use of ADT with EBRT improved overall survival or cancer-specific survival of patients with PC compared with EBRT alone. A total of 4–6 months of ADT combined with EBRT was an effective treatment for intermediate-risk PC, (3–6) whereas 2–3 years of ADT combined with EBRT was recommended to manage high-risk PC. (7–9) With regard to ADT, we have recently reported the clinical significance of attaining a TST level of 20 ng/dL during combined androgen blockade. (10) Klotz et al. also reported that a low nadir testosterone (<20 ng/dL) within the first year of ADT correlated with improved cause-specific survival. (11) These data showed the clinical significance of monitoringTST levels during ADT in PC patients.
Although combined ADT with EBRT is standard therapy in intermediate and high-risk PC patients, we have limited evidence related to the shift of TST levels during and after treatment. (6) For instance, in assessing biochemical recurrencefree survival in patients who received combined ADT with EBRT, it is desirable to discriminate patients who do not relapse after recovery of TST or patients who do not relapse due to the supracastrated level of TST. If we can predict the recovery of TST in individual patients, we might be able to more objectively assess biochemical recurrence in patients who received ADT with EBRT. In addition, recovery of the TST level is critical in those who receive intermittent ADT. Furthermore, we might even temporarily terminate long-term ADT in those who are expected to remain castrate, especially in those with low-performance status or elderly patients.
In the current study, the predictors of TST recovery were assessed after termination of ADT in high/intermediate-risk PC patients receiving EBRT with neoadjuvant and adjuvant ADT. The current data might provide evidence of not only TST recovery, but also when to terminate long-term ADT without harming castration levels in PC patients.
Methods
A total of 82 Japanese patients who received EBRT with ADT using a LHRH agonist for high- and intermediate-risk PC at Chiba University Graduate School of Medicine Hospital, Chiba City, Chiba, Japan, from 2003 to 2016 were retrospectively enrolled in this study. Intermediate-risk patients received neoadjuvant ADT only, and high-risk patients received both neoadjuvant and adjuvant ADT. Neoadjuvant ADT was given for 6 months, and adjuvant ADT was given for 2 years. Some of the very high-risk PC patients received over 3 years of ADT based on their doctor’s decision. Leuprorelin or goserelin was used as the LHRH agonist. A total of 76 patients took bicalutamide 80 mg every day with the LHRH agonist. The EBRT dose was 72 Gy by 3DCRT. The serum TST levels were mainly measured every 3 months, with some exception based on the individual follow-up periods and follow-up protocol. We studied TST levels after termination of ADT in association with other clinical factors, including ADT duration, age, PSA level and nadir TST level. A TST of >50 ng/dL was defined as the supracastrate level, and a TST of >200 ng/dL was defined as the normal level. We used receiver operating characteristic analysis for the cut-off point of other predictive factors.
Architect Testosterone II (Abbot Diagnostics, Lake Forest, IL, USA) was used to determine serum testosterone levels. We evaluated TST recovery to the supracastration level (TST >50 ng/dL) and normal level (TST >200 ng/dL) according to the risk criteria based on the independent predictive factors.
Compliance with ethical standards
The current study was approved by the institutional review board (approval number 2252).
Statistical analysis
The Kaplan–Meier method was used for statistical analysis, and the log– rank test was used to compare these estimates. Univariate and multivariate Cox proportional hazard models were used to estimate the cumulative incidence of TST recovery. P-values <0.05 were considered significant. JMP pro 12.0.1 software (SAS Institute, Cary, NC, USA) was used for all analyses.
Results
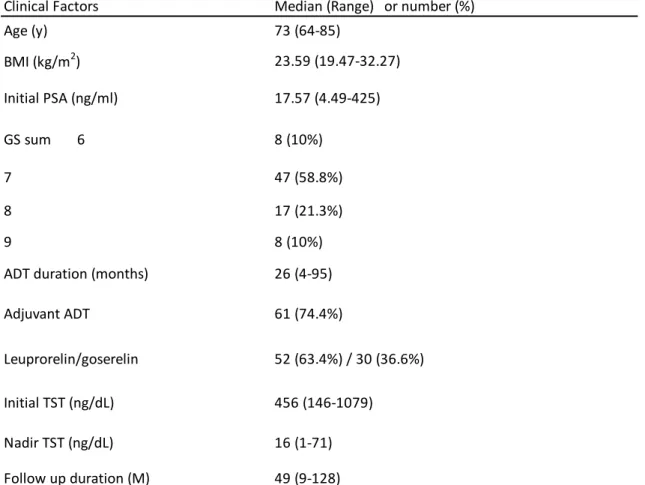
The median (range), age, initial PSA, initial TST and nadir TST were 73 years (64–85 years), 17.57 ng/mL (4.49–425 ng/mL), 456 ng/mL (146– 1079 ng/mL) and 16 ng/mL (1–71 ng/mL), respectively. The median dose of radiation therapy was 72 Gy. As the LHRH agonists, leuprorelin and goserelin were used by 52 patients (63.4%) and 30 patients (36.6%), respectively. The median duration of ADT was 26 months (4–95 months), and follow-up duration was 49 months (9–128 months; Table 1).
Figure 1 shows the TST levels of each patient after termination of ADT. This figure shows that there were two patterns of TST recovery. One was rapid recovery to a normal TST level by 6–12 months. The other was non-recovery to a normal TST level over the long term.
On univariate Cox proportional hazard analysis, ADT duration≥33 months (ADT ≥33 months; HR 0.16; P < 0.0001), TST nadir level ≤20 ng/dL (HR 0.22; P < 0.0001), TST ≤50 ng/dL 6 months after termination of ADT (TST 6 months ≤50 ng/dL; HR 0.18; P < 0.0001) and age >70 years (HR 0.42; P = 0.0048) were significant factors associated with TST recovery to the normal level (200 ng/dL). On multivariate analysis, ADT ≥33 months (HR 0.13; P = 0.0018), nadir TST level ≤20 ng/dL (HR 0.35; P = 0.0112) and TST 6 months ≤50 ng/dL (HR 0.21; P = 0.0075) were significant factors associated with TST recovery (Table 2). ADT ≥33 months, TST nadir level ≤20 ng/dL and TST 6 months ≤50 ng/dL were also significant factors in the log–rank test (P < 0.0001; Fig. 2a–c).
Next, ADT ≥33 months, TST nadir level ≤20 ng/dL and TST 6 months ≤50 ng/dL were defined as the risk factors, and TST recovery to normal levels was analyzed based on the number of risk factors. Figure 3 shows the Kaplan–Meier analysis of TST recovery to the normal level (200 ng/dL) after termination of ADT by the risk factor values, low risk = score 0, intermediate risk = score 1 and high risk = score 2–3. The TST recovery rates to the normal level 2 years after termination of ADT in the low-, intermediateand high-risk groups were 100%, 78.8% and 20.8%, respectively, and 5 years after termination of ADT they were 100%, 89.4% and 26.9%, respectively (low vs intermediate risk P = 0.0049; intermediate vs high risk P < 0.0001;Fig. 3).
On univariate Cox proportional hazard analysis, ADT ≥33 months (HR 0.22; P < 0.0001), TST nadir level ≤20 ng/dL (HR 0.28; P < 0.0001) and
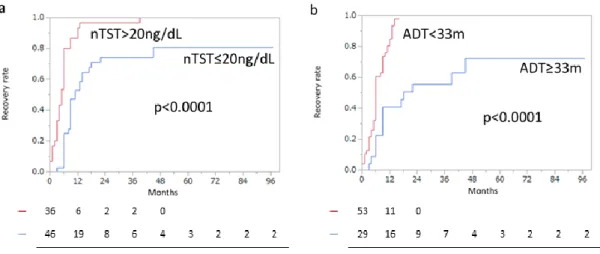
initial PSA >36.16 ng/mL (HR 0.52; P = 0.0364) were significant factors associated with TST recovery to supracastrate level (TST >50 ng/dL). On multivariate analysis, ADT ≥33 months (HR 0.31; P = 0.0023) and TST nadir level ≤20 ng/dL (HR 0.38; P = 0.0012) were significant factors associated with TST recovery to the supracastrate level (Table 3). ADT ≥33 months and TST nadir level ≤20 ng/dL were also significant factors in the log–rank test (P < 0.0001; Fig. 4a,b).
Androgen deprivation therapy ≥33 months and TST nadir level ≤20 ng/dL were defined as the risk factors, and TST recovery to supracastrate level was analyzed by the number of risk factors. Figure 3 shows the Kaplan–Meier analysis of TST recovery to supracastrate level (50 ng/dL) after termination of ADT by the number of risk factors, low risk = score 0, intermediate risk = score 1 and high risk = score 2. The TST recovery rates to the supracastrate level 2 years after termination of ADT in the low-, intermediate- and high-risk groups were 100%, 90.9%, and 51.5%, respectively, and 5 years after termination of ADT, they were 100%, 100% and 63.4%, respectively (low vs intermediate risk P = 0.0014; intermediate vs high risk P < 0.0001; Fig. 5).
Between leuprorelin and goserelin, there were no significant differences in TST recovery to both the supracastrate level (>50 ng/dL; P = 0.8581) and the normal level (>200 ng/dL; P = 0.6661; Fig. 6).
Discussion
The present study identified that a nadir TST of ≥20 ng/dL and ADT duration of ≤33 months were useful as markers for predicting TST recovery to the supracastrate level in PC patients that received EBRT with ADT. Furthermore, TST of <50 ng/dL at 6 months after termination of ADT predicted reduced TST recovery to the normal level (>200 ng/dL). Based on three factors, (i) nadir TST, (ii) duration of ADT and (iii) TST 50 ng/dL at 6 months after ADT, it might also be possible to assess the trends of TST recovery in PC patients who receive EBRT with ADT.
Past studies showed that the predictive factors of TST recovery after termination of ADT were ADT duration and age. (12–14) By carrying out testicular biopsies in PC patients who received long-term ADT, Giberti et al. reported that long-term ADT impaired Leydig cell masses with tubular derangement and fibrosis. (15) Long-term ADT induces not only functional inhibition of testicular androgenesis, but also anatomical testicular damage that is likely irreversible. Egawa et al. reported that patients who maintained castrate TST levels after termination of long-term ADT had above normal luteinizing hormone levels. (13) This is considered to occur because the feedback system of the hypothalamic–pituitary axis responded normally to the low TST levels after termination of ADT. Past studies reported that older age was a significant factor associated with slower TST recovery. (14, 16, 17) Other studies showed that the production of TST decreases with age. (18, 19) This decline might be related to later TST recovery in older men treated with ADT. In the present study, age was a significant predictive factor in the univariate analysis. Even if we confirm age as a continuous variable, the result was consistent (Table S1). However, age failed to remain as an independent factor in multivariate analysis. This result might indicate that the predictive ability of other variables including nadir TST and duration of ADT had more significant predictive ability compared with that of age, in the case of TST recovery after termination of ADT.
With regard to the direct effect of radiation on TST levels, some studies showed the impact of scatter radiation on TST levels and Leydig cell function. (20–22) Zagars et al. reported that the mean percentage decrease of TST after 68-Gy EBRT for localized PC was 9%. (21) Pickles et al. reported that the mean percentage decrease of TST 6 months after 68-Gy
EBRT for localized PC was 17% and recovery of TST typically
occurred 18 months after EBRT. (22) Tsumura et al. reported TST recovery after termination of long-term ADT with prostate brachytherapy, and they found that TST at the termination of ADT predicted TST recovery. (16) It is not clear how brachytherapy influences TST levels, but TST recovery after termination of ADT depends mainly on ADT duration, independent of the type of radiation therapy.
ADT has significant adverse effects, including hot flushes, decreased libido, loss of bone density and muscles, and possible cardiovascular events. The decrease in testosterone due to ADT results in both loss of libido and a decrease in erectile function. Erectile dysfunction was reported to be induced by venous leakage, decreased arterial flow and impaired nitric oxide under the reduced TST environment. (23)
The European Organization for Research and Treatment of Cancer carried out a non-inferiority trial of radiation plus 6 versus 36 months ADT in men with high-risk to locally advanced PC. They found a significant improvement in sexual function and activity with the shorter course of ADT (P < 0.001), but there was also a significant increase in mortality (HR for death 1.42; 95.71% CI 1.09–1.85). (9) Although there was no direct quality of life comparison between 18 and 36 months of ADT, the TROG03-04 trial randomized men to 6 versus 18 months of ADT and found that, in the 18-month arm of ADT, sexual activity was worse at 18 months, but not significantly worse by 36 months. (24) In the present data, the TST recovery rate to normal level 2 years after termination of ADT was 100% in low-risk patients, whereas that of high-risk patients was 20.8%. Although the rate of TST recovery is low in high-risk patients, the present study provided novel evidence showing that, by examining TST recovery to 50 ng/dL at 6 months after termination of ADT, one can predict the recovery of TST to the normal level. In contrast, when we examined the patients that received >3 years of ADT, TST recovery at 6 months and nadir TST failed to predict the TST recovery to a normal level (Table S2). This evidence might indicate serious damage in the testicular function of TST production after >3 years of ADT.
With regard to the limitations of the present study, first, it only analyzed a small number of patients in a retrospective manner. A large number of patients need to be studied prospectively to accurately determine the
predictors for TST recovery after ADT. Second, serum TST levels were mainly measured every 3 months; however, the intervals were different for some of the patients. The difference in measurement time-point might affect the result of TST recovery. The current result will need to confirmed in a prospective manner. Third, the type of EBRT was only 3DCRT. Recently, the number of PC patients who receive intensity-modulated radiation therapy has been increasing. We are currently investigating the difference in TST recovery between 3DCRT and intensity-modulated radiation therapy. Fourth, only LHRH agonists were used for ADT in the present study. We are currently investigating the difference in TST recovery between LHRH agonist and LHRH antagonist treatment.
In conclusion, nadir TST of 20 ng/dL and duration of ADT predict TST recovery to the supracastrate level in PC patients who received EBRT. The current data described the significance of not only the duration of hormonal therapy, but also monitoring the nadir TST level to predict TST recovery in patients receiving combined EBRT with ADT.
Acknowledgments
The current work is supported by the Chiba University Grant aid program A 2016 and a Grant-in-Aid for Scientific Research C 17K11125. We acknowledge Haruhito Uchida, Department of Vascular Biology, Graduate School of Medicine, Dentistry and Pharmaceutical Sciences for statistical advice. We thank Hisayo Karahi for management of the data and documentary work.
Conflict of interest
References
[1] Sakamoto S. Editorial Comment to Androgen receptor targeted therapies in castration-resistant prostate cancer: Bench to clinic. Int J Urol. 2016; 23: 666.
[2] Sakamoto S. Editorial Comment to Androgen receptor splice variant 7 in castration-resistant prostate cancer: Clinical considerations. Int J Urol. 2016; 23: 653.
[3] D'Amico AV, Chen MH, Renshaw AA, Loffredo M, Kantoff PW. Androgen suppression and radiation vs radiation alone for prostate cancer: a randomized trial. JAMA. 2008; 299: 289-95.
[4] Denham JW, Steigler A, Lamb DS et al. Short-term neoadjuvant androgen deprivation and radiotherapy for locally advanced prostate cancer: 10-year data from the TROG 96.01 randomised trial. Lancet Oncol. 2011; 12: 451-9.
[5] Jones CU, Hunt D, McGowan DG et al. Radiotherapy and short-term androgen deprivation for localized prostate cancer. N Engl J Med. 2011; 365: 107-18.
[6] Yamada Y, Sakamoto S, Sazuka T et al. Validation of active surveillance criteria for pathologically insignificant prostate cancer in Asian men. Int J Urol. 2016; 23: 49-54.
[7] Bolla M, Van Tienhoven G, Warde P et al. External irradiation with or without long-term androgen suppression for prostate cancer with high metastatic risk: 10-year results of an EORTC randomised study. Lancet Oncol. 2010; 11: 1066-73.
[8] Horwitz EM, Bae K, Hanks GE et al. Ten-year follow-up of radiation therapy oncology group protocol 92-02: a phase III trial of the duration of elective androgen deprivation in locally advanced prostate cancer. J Clin Oncol. 2008; 26: 2497-504.
[9] Bolla M, de Reijke TM, Van Tienhoven G et al. Duration of androgen suppression in the treatment of prostate cancer. N Engl J Med. 2009; 360: 2516-27.
[10] Kamada S, Sakamoto S, Ando K et al. Nadir Testosterone after Long-Term Followup Predicts Prognosis in Patients with Prostate Cancer Treated with Combined Androgen Blockade. J Urol. 2015; 194: 1264-70. [11] Klotz L, O'Callaghan C, Ding K et al. Nadir testosterone within first year of androgen-deprivation therapy (ADT) predicts for time to
castration-resistant progression: a secondary analysis of the PR-7 trial of intermittent versus continuous ADT. J Clin Oncol. 2015; 33: 1151-6.
[12] Nejat RJ, Rashid HH, Bagiella E, Katz AE, Benson MC. A prospective analysis of time to normalization of serum testosterone after withdrawal of androgen deprivation therapy. J Urol. 2000; 164: 1891-4. [13] Egawa S, Okusa H, Matsumoto K, Suyama K, Baba S. Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer. Prostate Cancer Prostatic Dis. 2003; 6: 245-9.
[14] Kaku H, Saika T, Tsushima T et al. Time course of serum testosterone and luteinizing hormone levels after cessation of long-term luteinizing hormone-releasing hormone agonist treatment in patients with prostate cancer. Prostate. 2006; 66: 439-44.
[15] Giberti C, Barreca T, Martorana G et al. Hormonal pattern and testicular histology in patients with prostatic cancer after long-term treatment with a gonadotropin-releasing hormone agonist analogue. Eur Urol. 1988; 15: 125-7.
[16] Tsumura H, Satoh T, Ishiyama H et al. Recovery of serum testosterone following neoadjuvant and adjuvant androgen deprivation therapy in men treated with prostate brachytherapy. World J Radiol. 2015;
7: 494-500.
[17] Wilke DR, Parker C, Andonowski A et al. Testosterone and erectile function recovery after radiotherapy and long-term androgen deprivation with luteinizing hormone-releasing hormone agonists. BJU Int. 2006; 97: 963-8.
[18] Plymate SR, Tenover JS, Bremner WJ. Circadian variation in testosterone, sex hormone-binding globulin, and calculated non-sex hormone-binding globulin bound testosterone in healthy young and elderly men. J Androl. 1989; 10: 366-71.
[19] Morley JE, Kaiser FE, Perry HM, 3rd et al. Longitudinal changes in testosterone, luteinizing hormone, and follicle-stimulating hormone in healthy older men. Metabolism. 1997; 46: 410-3.
[20] Izard MA. Leydig cell function and radiation: a review of the literature. Radiother Oncol. 1995; 34: 1-8.
[21] Zagars GK, Pollack A. Serum testosterone levels after external beam radiation for clinically localized prostate cancer. International
journal of radiation oncology, biology, physics. 1997; 39: 85-9.
[22] Pickles T, Graham P. What happens to testosterone after prostate radiation monotherapy and does it matter? J Urol. 2002; 167: 2448-52. [23] Nguyen PL, Alibhai SM, Basaria S et al. Adverse effects of androgen deprivation therapy and strategies to mitigate them. Eur Urol. 2015; 67: 825-36.
[24] Denham JW, Wilcox C, Joseph D et al. Quality of life in men with locally advanced prostate cancer treated with leuprorelin and radiotherapy with or without zoledronic acid (TROG 03.04 RADAR): secondary endpoints from a randomised phase 3 factorial trial. Lancet Oncol. 2012;
Table 1. Patients’ characteristics (n=82)
Clinical Factors Median (Range) or number (%)
Age (y) 73 (64-85) BMI (kg/m2) 23.59 (19.47-32.27) Initial PSA (ng/ml) 17.57 (4.49-425) GS sum 6 8 (10%) 7 47 (58.8%) 8 17 (21.3%) 9 8 (10%)
ADT duration (months) 26 (4-95)
Adjuvant ADT 61 (74.4%)
Leuprorelin/goserelin 52 (63.4%) / 30 (36.6%)
Initial TST (ng/dL) 456 (146-1079)
Nadir TST (ng/dL) 16 (1-71)
Follow up duration (M) 49 (9-128)
BMI: Body mass index, PSA: Prostate specific antigen, GS: Gleason score, ADT: Androgen deprivation therapy, TST: Testosterone
Figure1
Fig. 1 TST levels after termination of ADT. There are two patterns of TST recovery. One is rapid recovery to a normal TST level by 6–12 months. The other is non-recovery to a normal TST level over the long term.
Table 2. TST recovery to normal level (200 ng/dL) after termination of ADT on cox proportional hazard analysis.
HR(95% CI) P HR(95% CI) P
ADT total duration≥ 33 months 0.16(0.05-0.35) <0.0001 0.13(0.02-0.50) 0.0018 TST≤ 50 ng/dL (6moths post ADT) 0.18(0.08-0.36) <0.0001 0.21(0.06-0.67) 0.0075
Nadir TST ≤ 20 ng/dL 0.22(0.11-0.43) <0.0001 0.35(0.14-0.79) 0.0112
Age at ADT off> 70 years 0.42(0.23-0.76) 0.0048 0.60(0.22-1.57) 0.3012 Initial PSA> 36.16 ng/ml 0.47(0.21-0.99) 0.0471 0.75(0.21-2.24) 0.6271 Leuprorelin (vs goserelin) 1.22(0.64-2.43) 0.5439
Initial TST≤ 456ng/dL 0.64(0.31-1.31) 0.2219
Gleason score≥ 8 0.69(0.30-1.39) 0.3157
BMI> 23.59 kg/m2 0.70(0.27-1.86) 0.469
Univariate analysis Multivariate analysis
TST > 50 ng/dL (6 months post ADT): TST> 50 ng/dL at 6 months after termination of ADT, Age at ADT off: Age when the patient stopped ADT, ADT: Androgen deprivation therapy, TST: Testosterone, PSA: Prostate specific antigen, BMI: Body mass index
Figure2
Fig. 2 Kaplan–Meier analysis of (a) TST recovery to a normal level (200 ng/dL) after termination of ADT by nadir TST level 20 ng/dL (nTST 20 ng/dL), (b) ADT duration 33 months (ADT 33 m) and (c) TST 50 ng/dL 6 months after termination of ADT (TST 50 ng/dL [6 m post-ADT]).
Figure3
Fig. 3 Kaplan–Meier analysis of TST recovery to a normal level (200 ng/dL) after termination of ADT by the risk factor score (low risk = score 0, intermediate risk = score 1 and high risk = score 2–3). ADT ≥33 months, TST ≤20 ng/dL and TST 6 months ≤50 ng/dL are the risk factors.
Figure4
Fig. 4 Kaplan–Meier analysis of (a) TST recovery to supracastrate level (>50 ng/dL) after termination of ADT by nadir TST level 20 ng/dL (nTST 20 ng/dL) and (b) ADT duration 33 months (ADT 33 m).
Table 3. TST recovery to supracastrate level (50 ng/dL) after termination of ADT on cox proportional hazard analysis.
HR(95% CI) P HR(95% CI) P
ADT total duration≥33M 0.22(0.10-0.45) <0.0001 0.31(0.13-0.67) 0.0023
Nadir TST≤20ng/dL 0.28(0.16-0.48) <0.0001 0.38(0.21-0.68) 0.0012
Initial PSA>36.16ng/ml 0.52(0.26-0.96) 0.0364 0.91(0.43-1.82) 0.8141
Age at ADT off>70 0.70(0.42-1.19) 0.184
Leuprorelin (vs Goserelin) 1.12(0.65-1.97) 0.6948
Initial TST≤456ng/dL 0.88(0.49-1.61) 0.6908
Gleason score≥8 0.55(0.28-1.01) 0.0542
BMI>23.59 1.22(0.56-2.75) 0.6129
Univariate analysis Multivariate analysis
Age at ADT off: Age when the patient stopped ADT, ADT: Androgen deprivation therapy, TST: Testosterone, PSA: Prostate specific antigen, BMI: Body mass index
Figure5
Fig. 5 Kaplan–Meier analysis of TST recovery to the supracastrate level (>50 ng/dL) after termination of ADT by the number of risk factors (low risk = score 0, intermediate risk = score 1 and high risk = score 2). ADT ≥33 months and TST nadir level ≤20 ng/dL are the risk factors.
Figure6
Fig. 6 Kaplan–Meier analysis by type of LHRH agonist (leuprorelin and goserelin). TST recovery rates to (a) the supracastrate level (TST >50 ng/dL) and (b) normal level (TST >200 ng/dL) after termination of ADT.