この総説は,第46 回日本磁気共鳴医学会大会シンポジウム「小児領域の MRI の適応」での講演を中心にまと めたものである.
キーワード
fetus, amniotic ‰uid, HASTE, True-FISPFig. 1. Fetus at 33 weeks of gestation with inien-cephaly. Sagittal T2WI shows the short cervical spine with marked hyperextension of the neck and macrocephaly. Note the hydrocephalus, kyphosis and thoracic myelocele.
doi:10.2463/jjmrm.20191674
総 説
胎児 MRI の適応と安全
桑 島 成 子
獨協医科大学放射線医学講座は じ め に
胎児画像診断の第一選択は現在も超音波検査
で あ る . MRI は 超 音 波 検 査 で 診 断 に 至 ら な
かった場合,分娩体制や治療方針決定に更なる
情報が必要な場合に施行される.高速撮像法の
進歩により動きのアーチファクトが少ない鮮明
な画像が取得可能となり MRI の適応は拡大
し,今や胎児診断に欠かせない画像診断となっ
ている.
本稿では MRI が診断に有用な症例について
概説するとともに胎児に対する安全性について
最近の知見を示す.
胎児
MRI の利点
MRI は超音波検査と比較していくつか利点
がある
1),2).胎盤の位置や胎児の位置,母親の
肥満が検査の妨げにならない.超音波検査ほど
術者の技量の差が問題にはならない.広い撮影
野を得られることで超音波検査では指摘されて
いない胎児の異常所見の追加や母親の異常所見
も指摘できる.胎児の全体を 1 枚で見ること
ができ胎児の体型や,脊椎の配列(Fig. 1),
双胎の位置関係(Fig. 2)などが把握できる.
骨からのアーチファクトがないので妊娠後期で
も後頭蓋窩が評価できる(Fig. 3).そして,
最大の利点は羊水過少が検査の妨げにならない
ことである(Fig. 4).羊水過少をきたす疾患
は致死的な疾患が多く,胎児診断は分娩時体制
や分娩時期,両親へのカウンセリングに重要で
ある.
撮
影
法
基本は羊水とのコントラストが良好な T
2WI
の高速撮像法である.Half-fourier acquisition
2019 年 3 月 26 日受理
Fig. 2. Fetuses at 27 weeks of gestation. Coronal T2WI shows size discrepancy. The smaller fetus has a congenital diaphragmatic hernia (arrow). The larger fetus shows normal development.
Fig. 3. Fetus at 33 weeks of gestation with rhombenceph-alosynapsis. (a) Axial T2WI shows transverse cerebellar fo-lia (arrow) and absence of the midline vermis. (b) Sagittal T2WI shows a narrow fourth ventricle and absent primary ˆssure.
Fig. 4. Fetus at 21 weeks of gestation with Potter sequence and severe oligohydramnios. Coronal T2WI shows bilateral large bright intensity in the kidneys (arrow) that represent multiple micro cysts due to autosomal recessive polycystic kidney dis-ease. The normal bladder is not identiˆed. Note the presence of oligohydramnios.
腎は拡散強調像で高信号を示すので異所性腎
や小さな腎,無形成腎の評価に役立つ
1).
Fig. 5. Normal fetus at 30 weeks of gestation. Coronal T1WI shows high intensity in the thyroid (arrow), liver, and meconium.
Fig. 6. Fetus at 38 weeks of gestation with Chiali malformation. Sagittal T2WI demonstrates small posterior fossa with cerebellum herniating through the foramen magnum (arrow), and lumbosacral my-elocele (double arrow).
はどのような場合に推奨されるか」という問
いに対し,頭部,頭頸部,体幹部病変(心臓を
除く)とある
3).ISUOG(International
Socie-ty of Ultrasound in Obstetrics and Gynecology)
の 2017 年度 Practice Gridlines では胎児 MRI
の適応を 0 : not at all indicated から 7 :
deˆ-nitely indicated
に score している
4).
胎児 MRI の適応に関しては 1.5T と 3.0T で
違いはない
4).
1. 脳
MRI が行われる最も頻度が高い目的が脳室
拡大の原因精査である.2 次元の脳室拡大の判
定は通常横断像で側脳室三角部の幅を測定す
る.週数にかかわらず 10 mm 未満が正常とさ
れている.10 mm 以上でも経過観察で自然に
軽快する症例もある.超音波と MRI での測定
誤差は約 2 mm である.MRI では脳室拡大の
有無,脳室拡大の原因やシャントの適応がある
か,脳の破壊性変化か,他に中枢神経に奇形が
ないか,中枢神経以外に異常所見がないか診断
する
5).
1)Chiali 奇形
後頭蓋窩が小さく,小脳や脳幹の大後頭孔へ
の下垂がある.ほぼ全例に脊髄髄膜瘤と水頭症
を認める(Fig. 6).超音波検査では髄膜瘤が
指摘しにくい症例がある(Fig. 1).MRI では
下位髄膜瘤や脊椎奇形合併髄膜瘤の診断が可能
である.
2)X 連鎖性遺伝性水頭症
原因遺伝子が神経接着因子 L1CAM 遺伝子
と同定された先天性水頭症である.患児は男児
のみである.男児の中脳水道狭窄症の 25と
いわれている
6).特徴的な臨床症状として著明
な水頭症と母指の内転屈曲がある(Fig. 7).
早期に脳室腹腔シャント術を行うことで,進行
性の頭囲拡大は軽快するが,重度の精神運動発
達遅滞は免れない.
3)脳梁形成不全
完全欠損,部分欠損,低形成がある.矢状断
像で完全欠損は脳梁構造を認めない.完全欠損
では横断像や冠状断像で後角優位の脳室拡大,
前角を含めた左右側脳室の相互開離が見られ
る.半球間裂嚢胞(Fig. 8),脂肪腫や Chiari
型奇形が認められることがある.
Fig. 7. Fetus at 26 weeks of gestation with X-linked hydrocephalus. Axial (a) and sagittal (b) T2WI show dilata-tion of the lateral ventricles, agenesis of the corpus callosum and adducted thumbs (arrow).
Fig. 8. Fetus at 32 weeks of gestation with absent corpus callosum and interhemispheric cyst. Axial T2WI (a) shows dilatation of the posterior lateral ventricles. Sagittal T2WI (b) shows absent corpus callosum with cyst (ar-row).
4)出血
上衣下出血や脳室内出血により脳室拡大をき
たす(Fig. 9).T
2が出血の描出に有用であ
る
7).
2.
頸部
頸部病変に対しては発生部位,広がり,食道
や気道の圧排や狭窄の有無を MRI で評価す
る
1)(Fig. 10).さらに,気道病変による肺低
形成や肺の過膨脹や腹水を呈する先天性胎児気
道閉鎖症候群(CHAOS : congenital high
air-way obstruction syndrome)の有無を確認す
る.
3.
胸部
肺の形成は妊娠 17 週頃までに気管支が形成
され,24 週から 40 週にかけて肺胞嚢が形成さ
れる.胎児の肺が正常に発育するには十分な肺
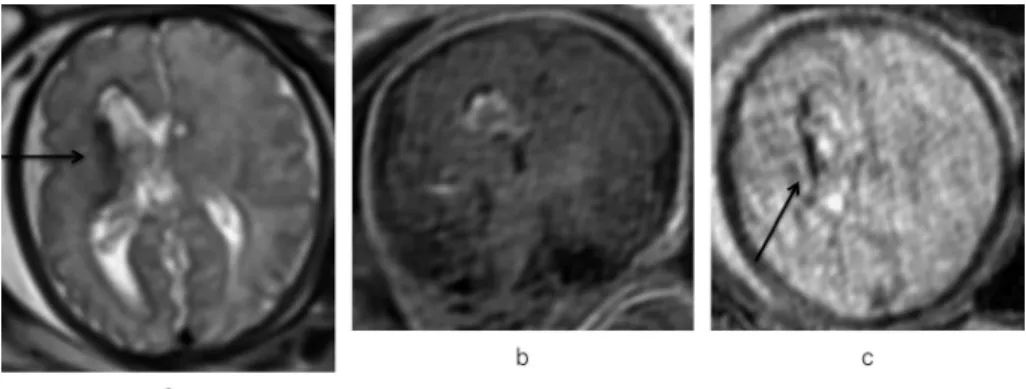
Fig. 9. Fetus at 34 weeks of gestation with germinal matrix hemorrhage. T2WI (a) demonstrates abnormal hypointensity lining the germinal matrix (arrow), consistent with right germinal matrix hemorrhage. Coronal T1WI (b) demonstrates high intensity in the right germinal matrix. Axial T2(c) demonstrates more deˆnitive hypointensity in the right germinal matrix (arrow).
Fig. 10. Fetus at 28 weeks of gestation with neck mass. Coronal (a) and axial (b) T2WI showing left cystic lymph-atic malformation of the neck with extension to the midline. The air way is displaced but patent (arrow).
液と呼吸様運動が必要である.T
2WI では肺の
成熟を反映して正常の肺は 28 週頃に低信号か
ら高信号へと変化していく
8),9).
1)先天性横隔膜ヘルニア
横隔膜の先天的欠損部から腹腔臓器が胸腔内
に脱出する奇形である.欠損孔の大きさは小さ
なものから全欠損に至るまで幅広い.胃が胸腔
内に脱出し正中を超える所見や肝が脱出してい
る所見は予後不良とされているが,必ずしも致
死 的 で は な い . MRI で は 脱 出 臓 器 , 縦 隔 偏
位,胎児水腫の有無,合併奇形を確認する.胎
便を含む腸管は T
1WI で高信号を示すので腸
管脱出の評価に有用である.
予後を大きく左右するのは肺低形成と肺高血
圧である.患側肺は低形成であり,重要なのは
健側肺の低形成の程度である.MRI による肺
低形成評価法は肺の体積測定と信号強度があ
る
8)~11)(Fig. 11).
arrow). Radiograph (b) shows mul-tiple air-ˆlled bowel loops in the left hemithorax with cardiomediastinal shift to the right and paucity of bowel gas in the abdomen.
4. 腹部
腹部腫瘤に対しては原発部位,大きさ,広が
りの評価が必要である.腹壁異常である腹壁破
裂や臍帯ヘルニアでは 2 者の鑑別が必要であ
る.T
1WI で軽度高信号を示す肝の位置が,腹
腔内に存在しているか脱出しているかは鑑別に
役立つ.臍帯ヘルニアではヘルニア嚢があり,
脱出した肝が T
1WI で軽度高信号を示す(Fig.
12).さらに合併奇形の有無を確認する(Fig.
13).腎疾患では羊水過少により超音波検査で
評 価 が 難 し い 場 合 が あ る . MRI で は 腎 の 有
無,大きさ,左右差,嚢胞の有無を確認する
(Fig. 4).片側腎の異常を認めた場合は対側腎
に異常がないか確認する.同時に,肺の評価,
腎以外の合併奇形の評価も行う.
5. 消化管
羊 水 過 多 の 原 因 の 1 つ に 消 化 管 閉 鎖 が あ
る.消化管閉鎖部より口側の腸管に拡張を認め
る.週数にもよるが,拡張空腸は T
2WI で高
信号(Fig. 14),回腸は胎便により T
1WI で高
信号を示す.食道閉鎖の MRI 診断は胃が認め
られない A 型は容易であるが,最も頻度の高
い C 型 は 胃 の 大 き さ か ら は 診 断 が 難 し い .
MRI では消化管閉鎖の有無,閉鎖部位の診断
と同時に他の消化管奇形,腎奇形,脊椎奇形も
確認する.
6. 羊水量異常
羊水過少が検査の妨げにならいないことが
MRI の大きな利点である.羊水が少ないと胎
児の動きが少なく,かえってモーションアーチ
ファクトのない画像が撮影できる.ただし,
Potter sequence のように羊水がほとんどない
場合は,胎児が著明に屈曲しているため 1 画
面で体幹全体の冠状断像は得られない(Fig.
4).同一画面上に肺と腎,頭部と胸部を撮像
することは難しい.同一画面に左右の肺を正確
に描出するのも難しい場合もある.
羊水過多の原因は主に消化管閉鎖や中枢神経
異常である.超音波検査で原因を特定できない
場合に MRI が施行される.気道狭窄や,小顎
症で嚥下が困難な疾患も羊水過多となる.
胎児
MRI の安全
妊婦が硬い検査台に仰臥位で長時間静止する
のは苦痛である.検査時間は短ければ短いほど
検査の侵襲性は低くなる.検査時間は 15 から
30 分が目安である.検査時間を短くするため
には検査前に産科医と放射線科医で適応,目的
の確認が必須である.撮影画像を見ながら撮影
法の変更や撮影順位の変更はあり得るが,検査
前に放射線科医と放射線技師で撮影範囲,必要
な撮影シーケンス,撮影順位をあらかじめ決め
ておく必要がある.何ら前処置は行わない.仰
臥位がつらい場合は左側臥位を試みる.
こ れ ま で の 報 告 で は 妊 娠 の ど の 時 期 で も
Fig. 12. Fetus at 25 weeks of gestation with omphalocele. Sagittal T2WI (a) shows an anterior abdomi-nal wall defect with herniation of abdominal contents, covered by peritoneum (arrow), within the am-niotic cavity. (b) The liver is hyperintence on T1WI (arrow).
Fig. 13. Fetus at 30 weeks of gestation with omphalocele and con-genital diaphragmatic hernia. Coronal (a) and sagittal (b) T2WI show omphalocele and left diaphrag-matic hernia. In addition, MRI shows skin edema, pleural eŠusion, ascites, and hydrops fetalis.
MRI 検 査 に よ る 胎 児 の 障 害 報 告 は な い
12).
3.0T
に関しても胎児 MRI を行うべきではない
と す る 報 告 は な い
1). 1.5T で も 3.0T で も
SAR(speciˆc absorption rate)に注意を払う
必要がある.米国 FDA(Food and Drug
Ad-ministration) で は 妊 婦 の SAR 上 限 を 全 身 4
W/Kg としており,JIS 規格による日本国内の
規定も同様である.胎児 MRI 施行時にはいず
れの磁場強度でも SAR を確認しながら検査を
行う
13),14).胎児 MRI 目的で造影剤は施行すべ
きではない.
Fig. 14. Fetus at 37 weeks of gestation with jejunal atresia. Coronal T2WI shows dilated bowel loops with high intensity (arrow).
胎児
MRI の撮影時期
胎児 MRI の最善の撮影時期は症例ごとに異
なる.妊娠 18 週以前では胎児が小さく超音波
所見以上の情報が得にくい.妊娠がすすむにつ
れ超音波検査では後頭蓋窩の評価が難しくなる
が,MRI では妊娠後期ほど画像のコントラス
トが良好になり後頭蓋窩評価を含め診断が容易
となり,付加情報も増える.特に 26 週から 32
週の間に臓器発育が進み MRI による評価も容
易になる
4).MRI による付加情報は 24 週以前
では約 43.8, 30 週以降では約 77.8という
報告もある
15).しかし,胎児 MRI の目的は胎
児の QOL の向上である.臨床的に必要と判断
した時点で行うのが最善の時期と考える.
お わ り に
胎児 MRI は超音波検査を補完する画像診断
として重要性は増している.機器の進歩ととも
に診断のステップアップが必要である.臨床に
有用な検査とするために検査前後で産科医,小
児科医,外科医,放射線科医,放射線技師の十
分なカンファレンスが必須である.
4) Prayer D, Malinger G, Brugger PC, et al. : ISUOG practice guidelines : performance of fetal magnetic resonance imaging. Ultrasound Obstet Gynecol 2017 ; 49 : 671680 5) 桑島成子胎児の画像診断.画像診断 2014 ; 34 : 16441655 6) 山崎麻美,脳室拡大を主な所見とする水頭症, 編集委員会,胎児期水頭症ガイドライン2 版. 京都,日本金芳堂,2010 ; 95103
7) Robinson AJ, Ederies MA : Fetal neuroimaging : an update on technical advances and clinical ˆnd-ings. Pediatr Radiol 2018 ; 48 : 471485 8) Kuwashima S, Nishimura G, Iimura F :
Low-in-tensity fetal lung on MRI may suggest the diag-nosis of pulmonary hypoplasia. Pediatr Radiol 2001 ; 31 : 669672
9) Moshiri M, Mannelli L, Richardson ML, Bhargava P, Dubinsky TJ : Fetal lung maturity assessment with MRI fetal lung-to-liver signal-in-tensity ratio. AJR Am J Roentgenol 2013 ; 201 : 13861390
10) Deshmukh S, Rubesova E, Barth R : MR assess-ment of normal fetal lung volumes : a literature review. AJR Am J Roentgenol 2010 ; 194 : W212217
11) Walleyo A, Debus A, Kehl S, Weiss C, Sch äonberg SO, Schaible T, B äusing KA, NeŠ KW : Peridic MRI lung volume assessment in fetuses with congenital diaphragmatic hernia : prediction of survival, need for ECMO, and de-velopment of chronic lung disease. AJR Am J Roentgenol 2013 ; 201 : 419426
12) Ray JG, Verneulen MJ, Bharatha A, Montanera WJ, Park AL : Association between MRI ex-posure during pregnancy and fetal and childhood outcomes. JAMA 2016 ; 316 : 952961
13) Krishnamurthy U, Neelavalli J, Mody S, et al. : MR imaging of the fetal brain at 1.5T and 3.0T ˆeld strengths : comparing speciˆc absorption
rate (SAR) and image quality. J Perinat Med 2015 ; 43 : 209220
14) Weisstanner C, Gruber GM, Brugger P, Mitter C, Diogo MC, Kaspian G, Prayer D : Fetal MRI at 3T-ready for routine use? Br J Radiol 2017 ; 90 : 20160362
15) Twickler DM, Magee KP, Caire J, et al. : Second-opinion magnetic resonance imaging for suspected fetal central nervous system abnor-malities. Am J Obstet Gynecol 2003 ; 188 : 492 496
Indication and Safety for Fetal MR Imaging
Shigeko KUWASHIMA
Department of Radiology, Dokkyo Medical University 880 Kita-kobayashi, Mibu-machi, Shimotsuga-gun, Tochigi 3210293