2019/3/8
1
埼玉動物医療センター 腫瘍科 林宝謙治
犬のリンパ腫アップデート
2019
講演内容
◼
犬のリンパ腫の概要
◼
リンパ腫の分類
◼
発生部位別分類
◼
高悪性度リンパ腫と低悪性度リンパ腫
◼
T細胞性リンパ腫とB細胞性リンパ腫
◼
リンパ腫各論
◼
多中心型
B vs T
◼
消化器型
◼
皮膚型
好発犬種とリスクの少ない犬種
(欧米)
◼
好発犬種
◼
ボクサー,ブルマスティフ,バセット・ハウンド, ブルドック,
セントバーナード,S・テリア,
E・テリア, G・シェパード,G・レトリーバー
,
L・レトリーバー,バーニーズ・MD
◼
リスクの少ない犬種
◼
ダックスフンド
,ポメラニアン,チワワ,Y・テリア,
プードル(ミニュチュア/トイ)
Zandvliet , VETERINARY QUARTERLY, 2016
1999−2007 n=156 2008−2018 n=25
日本では…
埼玉動物医療センター
リンパ腫の分類
リンパ腫の分類
◼
解剖学的分類:発生部位
◼
組織学的悪性度による分類:
腫瘍細胞の大きさ
◼低悪性度(高分化型,Low Grade,
小細胞型
)
◼中間悪性度(中分化型,Intermediate Grade ,
中細胞型
)
◼高悪性度(低分化型,未分化型,High Grade,
大細胞型
)
◼
免疫学的な分類
◼Bリンパ球の腫瘍
◼Tリンパ球の腫瘍
◼どちらにも分類できない腫瘍(NON-T,NON-B)
1
2
3
4
5
6
2
解剖学的部位による分類
Madewell BR, Vet Cancer Med 2nd ed., 1987 SAMEC 2007-2018
解剖学的部位による分類
多中心型 80% 消化器型 16% その他 4%Madewell BR, Vet Cancer Med 2nd ed., 1987
SAMEC 2007-2018
悪性度分類
低悪性度(小細胞型)
高悪性度(大細胞型)
悪性度による
進行速度,生存期間の違い
高悪性度
低悪性度
病期進行
急速
緩慢
治療反応
高い
低い
生存期間
短い
長い
リンパ腫の悪性度の比率
埼玉AMC
(1999-2015)
欧米の報告
低悪性度
6% (6/99)
5~10%
中間悪性度
5% (5/99)
20~30%
高悪性度
89% (88/99) 60~70%
Carter,Can J Vet Res,1986 Appelbaum,Hematol Onco ,1984 Taske,Exp Hematol,1994 K Rimpo VCS Proc 2008
リンパ腫の分類
(
悪性度とT,B分類)
B細胞型
高悪性度
T細胞型
高悪性度
B細胞型
低悪性度
T細胞型
低悪性度
※発生部位位によって高悪性度しかないリンパ腫もある
※中間悪性度の多くは,高悪性度と同様の治療を行う?
7
8
9
10
11
12
2019/3/8
3
発生部位によるリンパ腫の各論
多中心型リンパ腫
多中心型リンパ腫
◼
犬のリンパ腫で最も多いタイプ
◼抗がん治療に最も反応する腫瘍
体表リンパ節腫大の鑑別診断
◼
腫瘍性疾患
◼リンパ腫
◼リンパ性白血病
◼組織球性肉腫
◼様々な悪性腫瘍のリンパ節転移
体表リンパ節腫大の鑑別診断
◼
非腫瘍性疾患
◼
感染症
◼
免疫介在性疾患
◼
全身性エリテマトーデス,慢性関節リウマチなど
◼
アレルギー性疾患
◼
ノミアレルギー(特に猫)など
多中心型リンパ腫の臨床症状
◼
リンパ節腫大,通常は痛み伴わない
◼
その他は,無症状の事も多い
◼
20-40%の症例に非特異的な症状
◼
体重減少
◼
無気力,元気,食欲低下
◼
発熱
◼
多飲多尿
◼
腹囲膨満(肝脾腫大)
◼
嘔吐,下痢
◼
咳(肺浸潤)
13
14
15
16
17
18
4
埼玉動物医療センターでは!
◼
眼科でリンパ腫が見つかることが度々あります
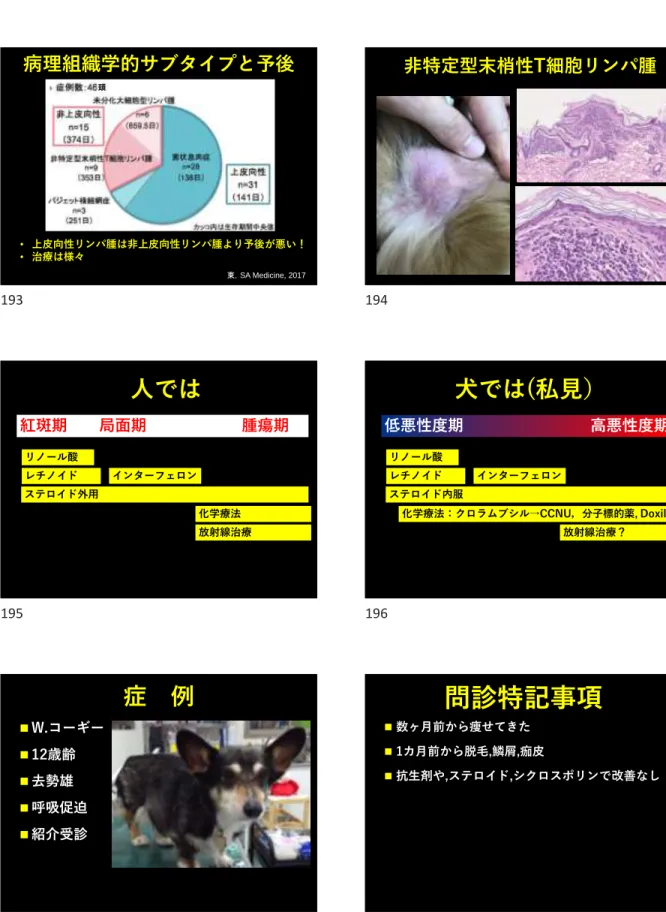
リンパ腫@眼の症状
◼
免疫異常→ぶどう膜炎
◼
DIC→前眼房出血
ぶどう膜炎で失明した
リンパ腫の犬
19
20
21
22
23
24
2019/3/8
5
診 断
◼
多くは細胞診で診断可能
◼
下顎リンパ節は避ける
◼
低悪性度リンパ腫は,リンパ節の切除生検
(病理組織検査)が必要
低悪性度 と高悪性度 の違い
(細胞診)
低悪性度 リンパ腫
高悪性度 リンパ腫
リンパ節の切除生検へ進む 確定診断進行度の把握:ステージング
◼
身体検査
◼
CBC,血液化学検査
◼
尿検査
◼
胸部,腹部X線検査
◼
超音波検査
◼
肝臓,脾臓の細胞診
◼
骨髄検査
◼
T,B分類(PCR,免疫染色)
進行度の把握:臨床ステージ
(WHO)
ステージ I :
単独のリンパ節,リンパ器官に限局
ステージ II :
局所の複数のリンパ節の腫脹
ステージ III : 全身のリンパ節腫脹
ステージ IV : 肝臓・脾臓にリンパ腫が波及
ステージ V : 末梢血や骨髄に腫瘍細胞が出現
リンパ腫がリンパ器官以外の臓器に波及
リンパ腫のサブステージ
(WHO)
サブステージ a :臨床徴候なし
サブステージ b :臨床徴候あり
※高Ca血症がある場合臨床徴候に関わらずサブステージ b
B B B B B B B B B T T T T T B B B B 反応性(感染,炎症) B細胞性リンパ腫 T T T T T T T T T Tクローナリティー検査のイメージ
T細胞性リンパ腫25
26
27
28
29
30
6
多中心型リンパ腫の治療
◼
悪性腫瘍の治療
◼
化学療法(抗がん治療)
◼
外科手術
◼
放射線療法
◼
免疫療法
◼
光線力学療法
◼
温熱療法
◼
栄養療法
高悪性度多中心型リンパ腫
(大細胞型)
高悪性度リンパ腫の治療で
用いられる代表的な抗がん剤
第1選択薬:CHOPベースプロトコール(L-CHOP)
(C): シクロホスファミド
(H): ドキソルビシン(ハイドロキシダウノロビシン)
(O): ビンクリスチン(オンコビン)
(P) : プレドニゾロン
(L) : L-アスパラギナーゼ
もし治療をしなかったら?
◼
無治療のリンパ腫の予後
◼
ほとんどの犬が4-6週間後に死亡
UW25プロトコール
1 2 3 4 5 6 7 8 9 10 11 13 15 17 19 21 23 25 L-ASP ⚫️ VCR ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ CPA ⚫️ ⚫️ ⚫️ ⚫️ DOX ⚫️ ⚫️ ⚫️ ⚫️ Pre ⚫️ ⚫️ ⚫️ ⚫️ L-アスパラギナーゼ:400IU/kg SC ビンクリスチン:0.7mg/m2IV シクロホスファミド:250mg/m2IV ドキソルビシン:30mg/m2 プレドニゾン: 2mg/kg PO SID × 7日→1.5mg/kg × 7日→1mg/kg × 7日→0.5mg/kg × 7日Garret LD et al. J Vet Intern Med,2002
UW19プロトコール
1 2 3 4 6 7 8 9 11 12 13 14 16 17 18 19 L-アスパラギナーゼ ⚫️ ️ ビンクリスチン ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ シクロフォスファミド ⚫️ ⚫️ ⚫️ ⚫️ ドキソルビシン ⚫️ ⚫️ ⚫️ ⚫️ プレドニゾン ⚫️ ⚫️ ⚫️ ⚫️ L-アスパラギナーゼ:400IU/kg IM ビンクリスチン:0.5-0.7mg/m2IV シクロフォスファミド:200mg/m2IV ドキソルビシン:30mg/m2(10kg<)または1mg/kg(10kg>) プレドニゾン: 2mg/kg PO SID × 7日→1.5mg/kg × 7日→1mg/kg × 7日→0.5mg/kg × 7日 Hosoya, JVIM, 200731
32
33
34
35
36
2019/3/8
7
CHOP 12weeks
1 2 3 4 5 6 7 8 9 10 11 12 L-アスパラギナーゼ ⚫️ ️ ビンクリスチン ⚫️ ⚫️ ⚫️ ⚫️ シクロフォスファミド ⚫️ ⚫️ ⚫️ ⚫️ ドキソルビシン ⚫️ ⚫️ ⚫️ ⚫️ プレドニゾン ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ ⚫️ L-アスパラギナーゼ:400IU/kg SC (デキサメサゾン前処置) ビンクリスチン:0.7mg/m2IV シクロフォスファミド:200mg/m2IV ドキソルビシン:30mg/m2 プレドニゾン:50mg/m2 PO 毎週day1-3のみ Simon, JVIM, 2006CHOP 15
Burton, Vet Comp Oncol, 2013 Curran, Vet Comp Oncol, 2015
高悪性度 多中心型リンパ腫
多剤併用プロトコールの治療成績
◼
完全寛解率:80%以上
◼
生存期間の中央値:1年
◼
2年生存率:25%
◼
完治率:?
その他の化学療法
◼
ドキソルビシン単剤
◼
5回投与(30mg/m
23週間毎)
◼
完全寛解率 50 - 70%
◼
生存期間の中央値 6 – 8 カ月
◼
プレドニゾロン単独
◼
経済的な事情などで化学療法が行えない場合の緩和治療
◼
生存期間は約1 – 2 カ月(延命効果なし)
◼
※プレドニゾロンの単独治療を行うとその後の抗がん剤
の効果は低下する可能性あり!
犬リンパ腫多剤併用導入プロトコールの比較
CHOPベースのまとめ
症例数 奏功率 (%) 完全 寛解率 (%) 完全寛解期 間 (中央値) 引用 VEL-CAP-S(Short)15W 56 ND 68 140 Moore (2001) UW25 53 94.2 92.3 287 Garrett (2002) L-CHOP 12 76 89 76 243 Simon (2006) UW19 30 100 77 174 Hosoya (2007) ※ND:データの記載なし犬リンパ腫の治療成績
まとめ
CR率 CR期間 生存期間 1年生存率 2年生存率 無治療 4-6週間 ステロイド 1-2カ月 DOX単独 65-75% 4-6カ月 COP 70-80% 6カ月 10-20% CHOP(L) 85-95% 9カ月 12-13カ月 25-50% 約25%37
38
39
40
41
42
8
犬のリンパ腫
全部CHOPで治療してませんか?
高悪性度 多中心型リンパ腫
CHOPプロトコールの治療成績
◼
完全寛解率:80%以上
◼
生存期間の中央値:1年
◼
2年生存率:25%
◼
完治率:???
※でもこれは,T細胞性リンパ腫に
当てはまる????
多中心型リンパ腫
T vs B
寛解期間
生存期間
T細胞型
1.7-5カ月
5-5.3カ月
B細胞型
5-11カ月
11-13カ月
• 犬の多中心型リンパ腫
• TとBでは予後が違う!
• 20-30%はT細胞性リンパ腫
Vail DM, Exp Hematol, 1996 Ruslander DA, In Vivo, 1997 Chun R, JVIM, 2000
埼玉動物医療センター
@多中心型リンパ腫
2007-2018
n=43DOXはT細胞性リンパ腫
にあまり効かない!
症例数
奏功率
(%)
CR率
(%)
B cell
29
100
86
T cell
12
50
17
Beaver et al. JAVMA 2010
高悪性度
T細胞性リンパ腫の治療
43
44
45
46
2019/3/8
9
高悪性度リンパ腫の治療で
用いられる代表的な抗がん剤
第2選択薬
アクチノマイシン-D
ミトキサントロン
クロラムブシル
メトトレキセート
プロカルバジン
ダカルバジン
イホスファミド
シトシンアラビノサイト
ロムスチン
◼
T細胞性リンパ腫の犬50頭
◼
完全寛解率は78%
◼
無進行生存期間の中央値:189日
L-MOPPプロトコール
2009年の報告
MOPPプロトコール
※メクロレタミンは,日本での入手は困難!Treatment of canine non-indolent T cell lymphoma
using the VELCAP-TSC protocol: A retrospective
evaluation of 70 dogs (2003–2013)
Ingrid H. Goodman a,b, Antony S. Moore a,c,*, Angela E. Frimberger a,cThe Veterinary Journal 211 (2016) 39–44
➢
T細胞性リンパ腫の犬70頭
➢
L-アス,VCR,CTX,DOX,Pre
➢
アクチノマイシンD
➢
プロカルバジン
➢
CCNU
L-CHOP AOPP CCNU + +VELCAP-TSP プロトコール
2016年の報告
AOPPプロトコール(変更型MOPP)
Day0
アクチノマイシD
0.5mg/m
2IV(10分かけて投与)
ビンクリスチン
0.7mg/m
2IV
プロカルバジン
50mg/m
2PO SID × 7日
プレトドニゾン
20mg/m
2PO SID × 7日
Day7:上記と同様の治療
Day14 CBCのみ(休薬)
Day21 休薬
Day28 上記サイクルを繰り返す
VELCAP-TSP プロトコール
49
50
51
52
53
54
10
Progression Free Survival
(PFS)
CR群 PR群 CR群(45) : 299日 PR群(6) : 113日 NR群(19) : 53日 完全寛解率:64.3%生存期間
Substage a MST 283日 Substage b 186日 CR:MST 362日 PR:177日 NR:53日 1年生存率 2年生存率 CR群(n=45) 45.5% 28.6% PR群(n=6) 20% 20% No Response(n=19) 0本プロトコールの有害事象
n=70
◼胃腸障害:90%(63頭)
◼発 熱 :41%(29頭)
◼薬剤減量:57%(40頭)
◼投与延期:66%(46頭)
◼死亡なし
有害事象のグレード
GRADE
0
1
2
3
4
消化器障害 6 (8%) 13 (19%) 26 (37%) 16 (23%) 8 (11%) 好中球減少症 7 (10%) 9 (13%) 15 (21%) 23 (33%) 15 (21%)L-CHOP-CCNU-MOPP
L-CHOP-CCNU-MOPP for canine lymphoma 245
cyclophosphamide (Baxter H ealthcareCorporation, Deerfi eld, IL, USA), doxorubicin (Bedford Labo-ratories, Bedford, OH , USA), vincristine (M ayne Pharma, Paramus, NJ, USA), prednisone (Roxane Laboratories, Columbus, OH , USA), CCNU (Bristol Laboratories, Princeton, NJ, USA), mechlorethamine (Ovation Pharmaceuticals, Deer-fi eld, IL, USA), vincristine and procarbazine (Sigma-Tau, Gaithersburg, M D, USA), pred-nisone] protocol is depicted in Table 1. A CBC was performed before each treatment, and a chem-istry panel was performed prior to treatment with CCNU. Scheduled treatments were delayed 2–5 days if the pre-treatment neutrophil count was < 1500 cellsmL− 1or if GI toxicity ≥ grade 219 was observed upon presentation for treatment. H owever, at week 7,L-asparaginase was given regardless of the neutrophil count. If adminis-tration of a chemotherapy drug resulted in neu-tropenia or GI toxicity ≥ grade 3,19subsequent treatments with that drug were administered at a 25% reduced dosage. After treatment with CCNU, dogs received prophylactic antibiotics [trimetho-prim –sulfadiazine (Interpharm, H auppauge, NY, USA), 15 mg kg− 1orally every 12 h for 14 days)]. If administration of CCNU on week 6 resulted in grade 4 neutropenia, the subsequent dosage given on week 16 was reduced to 70 mg m− 2. Dogs were removed from the study for the following reasons: progressive disease (defi ned below) at any time, no response by week 4 of the protocol or no CR by week 14 of the protocol. Dogs in CR at week 25 had chemotherapy discontinued and received a complete physical examination every month until relapse.
Historical treatment group
TheL-CH OP protocol used in the historical group of dogs is depicted in Table 2. Dogs in CR at week 24 discontinued chemotherapy and received a complete physical examination every month until relapse.
Assessment of remission
CR was defi ned as the resolution of all clinical signs and disappearance of all clinical evidence of dis-ease based on physical examination, radiography
Table 1.L-CH OP-CCN U-M OPP chemotherapy protocol administered to 66 dogs with lymphoma Induction phase
Week 1 L-asparaginase (400 U kg− 1SQ) Vincristine (0.5 m g m− 2IV) Prednisone (30 m g m− 2daily ×7 days) W eek 2 Cyclophosphamidea(200 m g m− 2IV)
Prednisone (20 m g m− 2daily ×7 days) W eek 3 Doxorubicin (1 mg kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2) Prednisone (10 m g m− 2daily ×7 days) W eek 4 Vincristine (0.7 m g m− 2IV) W eek 6 CCNU (90 mg m− 2orally) Week 7 L-asparaginaseb(400 U kg− 1SQ) W eek 8 Vincristine (0.7 m g m− 2IV) W eek 9 Doxorubicin (1 mg kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2) W eek 11 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV) Procarbazine (50 m g m− 2daily ×14 days) Prednisone (40 m g m− 2daily ×14 days) W eek 12 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV) Maintenance phase
W eek 14 Doxorubicin (1 m g kg− 1IV if < 1 m2or 30 m g m− 2IV if ≥ 1 m2) W eek 16 CCNU (90 m g m− 2orally) W eek 18 Vincristine (0.7 m g m− 2IV) W eek 20 Cyclophosphamidea(200 m g m− 2IV) W eek 22 Doxorubicin (1 m g kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2) W eek 20 Cyclophosphamidea(200 m g m− 2IV) W eek 22 Vincristine (0.7 m g m− 2IV) W eek 24 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV) Procarbazine (50 m g m− 2daily ×14 days) Prednisone (40 m g m− 2daily ×14 days) W eek 25 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV) aFurosemide (2 mg kg− 1IV) was given immediately before each cyclophospham ide treatm ent.
bDiphenhydram ine (2 m g kg− 1IM) was given 20 m in before theL-asparaginase treatm ent.
and ultrasonography. Partial remission (PR) was defi ned as ≥ 50% but < 100% reduction in size of all measurable disease. No response was defi ned as < 50% reduction in the size of measurable disease, increase in size of measurable disease or appear-ance of new lesions. Dogs that died (regardless of cause) or were lost to follow-up before the week 2 evaluation were considered to have not responded. After completion of both protocols, dogs were rechecked on a monthly basis to evaluate remission status. Relapse was defi ned as recurrence of lymph node or organ enlargement after CR or
ã 2010 Blackwell Publishing Ltd, Veterinary and ComparativeOncology, 8, 4, 243 –253
L-CHOP-CCNU-MOPP for canine lymphoma 245
cyclophosphamide (Baxter H ealthcareCorporation, Deerfi eld, IL, USA), doxorubicin (Bedford Labo-ratories, Bedford, OH , USA), vincristine (M ayne Pharma, Paramus, NJ, USA), prednisone (Roxane Laboratories, Columbus, OH , USA), CCNU (Bristol Laboratories, Princeton, NJ, USA), mechlorethamine (Ovation Pharmaceuticals, Deer-fi eld, IL, USA), vincristine and procarbazine (Sigma-Tau, Gaithersburg, M D, USA), pred-nisone] protocol is depicted in Table 1. A CBC was performed before each treatment, and a chem-istry panel was performed prior to treatment with CCNU. Scheduled treatments were delayed 2–5 days if the pre-treatment neutrophil count was < 1500 cellsmL− 1or if GI toxicity ≥ grade 219 was observed upon presentation for treatment. H owever, at week 7,L-asparaginase was given regardless of the neutrophil count. If adminis-tration of a chemotherapy drug resulted in neu-tropenia or GI toxicity ≥ grade 3,19subsequent treatments with that drug were administered at a 25% reduced dosage. After treatment with CCNU, dogs received prophylactic antibiotics [trimetho-prim –sulfadiazine (Interpharm, H auppauge, NY, USA), 15 mg kg− 1orally every 12 h for 14 days)]. If administration of CCNU on week 6 resulted in grade 4 neutropenia, the subsequent dosage given on week 16 was reduced to 70 mg m− 2. Dogs were removed from the study for the following reasons: progressive disease (defi ned below) at any time, no response by week 4 of the protocol or no CR by week 14 of the protocol. Dogs in CR at week 25 had chemotherapy discontinued and received a complete physical examination every month until relapse.
Historical treatment group
TheL-CH OP protocol used in the historical group of dogs is depicted in Table 2. Dogs in CR at week 24 discontinued chemotherapy and received a complete physical examination every month until relapse.
Assessment of remission
CR was defi ned as the resolution of all clinical signs and disappearance of all clinical evidence of dis-ease based on physical examination, radiography
Table 1.L-CH OP-CCN U-M OPP chemotherapy protocol administered to 66 dogs with lymphoma Induction phase
Week 1 L-asparaginase (400 U kg− 1SQ) Vincristine (0.5 m g m− 2IV) Prednisone (30 m g m− 2daily ×7 days) W eek 2 Cyclophosphamidea(200 m g m− 2IV)
Prednisone (20 m g m− 2daily ×7 days) W eek 3 Doxorubicin (1 mg kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2) Prednisone (10 m g m− 2daily ×7 days) W eek 4 Vincristine (0.7 m g m− 2IV) W eek 6 CCNU (90 mg m− 2orally) Week 7 L-asparaginaseb(400 U kg− 1SQ) W eek 8 Vincristine (0.7 m g m− 2IV) W eek 9 Doxorubicin (1 mg kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2) W eek 11 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV) Procarbazine (50 m g m− 2daily ×14 days) Prednisone (40 m g m− 2daily ×14 days) W eek 12 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV) Maintenance phase
W eek 14 Doxorubicin (1 m g kg− 1IV if < 1 m2or 30 m g m− 2IV if ≥ 1 m2) W eek 16 CCNU (90 m g m− 2orally) W eek 18 Vincristine (0.7 m g m− 2IV) W eek 20 Cyclophosphamidea(200 m g m− 2IV) W eek 22 Doxorubicin (1 m g kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2) W eek 20 Cyclophosphamidea(200 m g m− 2IV) W eek 22 Vincristine (0.7 m g m− 2IV) W eek 24 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV) Procarbazine (50 m g m− 2daily ×14 days) Prednisone (40 m g m− 2daily ×14 days) W eek 25 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV) aFurosemide (2 mg kg− 1IV) was given immediately before each cyclophospham ide treatm ent.
bDiphenhydram ine (2 m g kg− 1IM) was given 20 m in before theL-asparaginase treatm ent.
and ultrasonography. Partial remission (PR) was defi ned as ≥ 50% but < 100% reduction in size of all measurable disease. No response was defi ned as < 50% reduction in the size of measurable disease, increase in size of measurable disease or appear-ance of new lesions. Dogs that died (regardless of cause) or were lost to follow-up before the week 2 evaluation were considered to have not responded. After completion of both protocols, dogs were rechecked on a monthly basis to evaluate remission status. Relapse was defi ned as recurrence of lymph node or organ enlargement after CR or
ã 2010 Blackwell Publishing Ltd, Veterinary and ComparativeOncology, 8, 4, 243 –253
Rassnick , Vet Comp Oncol, 2010
L-CHOP-CCNU-MOPP
導入期
L-CHOP-CCNU-MOPP for canine lymphoma 245
cyclophosphamide (Baxter H ealthcareCorporation, Deerfi eld, IL, USA), doxorubicin (Bedford Labo-ratories, Bedford, OH , USA), vincristine (M ayne Pharma, Paramus, NJ, USA), prednisone (Roxane Laboratories, Columbus, OH , USA), CCNU (Bristol Laboratories, Princeton, NJ, USA), mechlorethamine (Ovation Pharmaceuticals, Deer-fi eld, IL, USA), vincristine and procarbazine (Sigma-Tau, Gaithersburg, M D, USA), pred-nisone] protocol is depicted in Table 1. A CBC was performed before each treatment, and a chem-istry panel was performed prior to treatment with CCNU. Scheduled treatments were delayed 2–5 days if the pre-treatment neutrophil count was < 1500 cellsmL− 1or if GI toxicity ≥ grade 219
was observed upon presentation for treatment. H owever, at week 7,L-asparaginase was given regardless of the neutrophil count. If adminis-tration of a chemotherapy drug resulted in neu-tropenia or GI toxicity ≥ grade 3,19subsequent
treatments with that drug were administered at a 25% reduced dosage. After treatment with CCNU, dogs received prophylactic antibiotics [trimetho-prim –sulfadiazine (Interpharm, H auppauge, NY, USA), 15 mg kg− 1orally every 12 h for 14 days)].
If administration of CCNU on week 6 resulted in grade 4 neutropenia, the subsequent dosage given on week 16 was reduced to 70 mg m− 2. Dogs were
removed from the study for the following reasons: progressive disease (defi ned below) at any time, no response by week 4 of the protocol or no CR by week 14 of the protocol. Dogs in CR at week 25 had chemotherapy discontinued and received a complete physical examination every month until relapse.
Historical treatment group
TheL-CH OP protocol used in the historical group of dogs is depicted in Table 2. Dogs in CR at week 24 discontinued chemotherapy and received a complete physical examination every month until relapse.
Assessment of remission
CR was defi ned as the resolution of all clinical signs and disappearance of all clinical evidence of dis-ease based on physical examination, radiography
Table 1.L-CH OP-CCN U-M OPP chemotherapy protocol administered to 66 dogs with lymphoma
Induction phase
Week 1 L-asparaginase (400 U kg− 1SQ)
Vincristine (0.5 m g m− 2IV)
Prednisone (30 m g m− 2daily ×7 days)
W eek 2 Cyclophosphamidea(200 m g m− 2IV)
Prednisone (20 m g m− 2daily ×7 days)
W eek 3 Doxorubicin (1 mg kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2)
Prednisone (10 m g m− 2daily ×7 days)
W eek 4 Vincristine (0.7 m g m− 2IV)
W eek 6 CCNU (90 mg m− 2orally)
Week 7 L-asparaginaseb(400 U kg− 1SQ) W eek 8 Vincristine (0.7 m g m− 2IV) W eek 9 Doxorubicin (1 mg kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2) W eek 11 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV) Procarbazine (50 m g m− 2daily ×14 days)
Prednisone (40 m g m− 2daily ×14 days)
W eek 12 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV)
Maintenance phase
W eek 14 Doxorubicin (1 m g kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2)
W eek 16 CCNU (90 m g m− 2orally)
W eek 18 Vincristine (0.7 m g m− 2IV)
W eek 20 Cyclophosphamidea(200 m g m− 2IV)
W eek 22 Doxorubicin (1 m g kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2)
W eek 20 Cyclophosphamidea(200 m g m− 2IV)
W eek 22 Vincristine (0.7 m g m− 2IV)
W eek 24 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV) Procarbazine (50 m g m− 2daily ×14 days) Prednisone (40 m g m− 2daily ×14 days) W eek 25 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV) aFurosemide (2 mg kg− 1IV) was given immediately before
each cyclophospham ide treatm ent.
bDiphenhydram ine (2 m g kg− 1IM) was given 20 m in before
theL-asparaginase treatm ent.
and ultrasonography. Partial remission (PR) was defi ned as ≥ 50% but < 100% reduction in size of all measurable disease. No response was defi ned as < 50% reduction in the size of measurable disease, increase in size of measurable disease or appear-ance of new lesions. Dogs that died (regardless of cause) or were lost to follow-up before the week 2 evaluation were considered to have not responded. After completion of both protocols, dogs were rechecked on a monthly basis to evaluate remission status. Relapse was defi ned as recurrence of lymph node or organ enlargement after CR or
ã 2010 Blackwell Publishing Ltd, Veterinary and ComparativeOncology, 8, 4, 243 –253
Rassnick , Vet Comp Oncol, 2010
L-CHOP MOPP CCNU L-ASP
55
56
57
58
59
60
2019/3/8
11
L-CHOP-CCNU-MOPP for canine lymphoma 245cyclophosphamide (Baxter H ealthcareCorporation,
Deerfi eld, IL, USA), doxorubicin (Bedford
Labo-ratories, Bedford, OH , USA), vincristine (M ayne
Pharma, Paramus, NJ, USA), prednisone (Roxane
Laboratories, Columbus, OH , USA), CCNU
(Bristol
Laboratories,
Princeton,
NJ,
USA),
mechlorethamine (Ovation Pharmaceuticals,
Deer-fi eld, IL, USA), vincristine and procarbazine
(Sigma-Tau, Gaithersburg, M D, USA),
pred-nisone] protocol is depicted in Table 1. A CBC
was performed before each treatment, and a
chem-istry panel was performed prior to treatment
with CCNU. Scheduled treatments were delayed
2–5 days if the pre-treatment neutrophil count
was < 1500 cells
mL
− 1or if GI toxicity ≥ grade 2
19was observed upon presentation for treatment.
H owever, at week 7,
L-asparaginase was given
regardless of the neutrophil count. If
adminis-tration of a chemotherapy drug resulted in
neu-tropenia or GI toxicity ≥ grade 3,
19subsequent
treatments with that drug were administered at a
25% reduced dosage. After treatment with CCNU,
dogs received prophylactic antibiotics
[trimetho-prim –sulfadiazine (Interpharm, H auppauge, NY,
USA), 15 mg kg
− 1orally every 12 h for 14 days)].
If administration of CCNU on week 6 resulted in
grade 4 neutropenia, the subsequent dosage given
on week 16 was reduced to 70 mg m
− 2. Dogs were
removed from the study for the following reasons:
progressive disease (defi ned below) at any time,
no response by week 4 of the protocol or no CR
by week 14 of the protocol. Dogs in CR at week
25 had chemotherapy discontinued and received a
complete physical examination every month until
relapse.
Historical treatment group
The
L-CH OP protocol used in the historical group
of dogs is depicted in Table 2. Dogs in CR at
week 24 discontinued chemotherapy and received
a complete physical examination every month until
relapse.
Assessment of remission
CR was defi ned as the resolution of all clinical signs
and disappearance of all clinical evidence of
dis-ease based on physical examination, radiography
Table 1.L-CH OP-CCN U-M OPP chemotherapy protocol administered to 66 dogs with lymphoma
Induction phase
Week 1 L-asparaginase (400 U kg− 1SQ)
Vincristine (0.5 m g m− 2IV)
Prednisone (30 m g m− 2daily ×7 days)
W eek 2 Cyclophosphamidea(200 m g m− 2IV)
Prednisone (20 m g m− 2daily ×7 days)
W eek 3 Doxorubicin (1 mg kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2)
Prednisone (10 m g m− 2daily ×7 days)
W eek 4 Vincristine (0.7 m g m− 2IV)
W eek 6 CCNU (90 mg m− 2orally)
Week 7 L-asparaginaseb(400 U kg− 1SQ)
W eek 8 Vincristine (0.7 m g m− 2IV)
W eek 9 Doxorubicin (1 mg kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2)
W eek 11 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV)
Procarbazine (50 m g m− 2daily ×14 days)
Prednisone (40 m g m− 2daily ×14 days)
W eek 12 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV)
Maintenance phase
W eek 14 Doxorubicin (1 m g kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2)
W eek 16 CCNU (90 m g m− 2orally)
W eek 18 Vincristine (0.7 m g m− 2IV)
W eek 20 Cyclophosphamidea(200 m g m− 2IV)
W eek 22 Doxorubicin (1 m g kg− 1IV if < 1 m2or
30 m g m− 2IV if ≥ 1 m2)
W eek 20 Cyclophosphamidea(200 m g m− 2IV)
W eek 22 Vincristine (0.7 m g m− 2IV)
W eek 24 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV)
Procarbazine (50 m g m− 2daily ×14 days)
Prednisone (40 m g m− 2daily ×14 days)
W eek 25 Mechlorethamine (3 m g m− 2IV)
Vincristine (0.7 m g m− 2IV) aFurosemide (2 mg kg− 1IV) was given immediately before each cyclophospham ide treatm ent.
bDiphenhydram ine (2 m g kg− 1IM) was given 20 m in before
theL-asparaginase treatm ent.
and ultrasonography. Partial remission (PR) was
defi ned as ≥ 50% but < 100% reduction in size of
all measurable disease. No response was defi ned as
< 50% reduction in the size of measurable disease,
increase in size of measurable disease or
appear-ance of new lesions. Dogs that died (regardless
of cause) or were lost to follow-up before the
week 2 evaluation were considered to have not
responded. After completion of both protocols,
dogs were rechecked on a monthly basis to evaluate
remission status. Relapse was defi ned as recurrence
of lymph node or organ enlargement after CR or
ã 2010 Blackwell Publishing Ltd, Veterinary and ComparativeOncology, 8, 4, 243 –253
Rassnick , Vet Comp Oncol, 2010
維持期
L-CHOP-CCNU-MOPP 317日
L-CHOP 298日
第一寛解期間の比較
Rassnick , Vet Comp Oncol, 2010
L-CHOP-CCNU-MOPP 317日
L-CHOP 298日
第一寛解期間の比較
35%の犬が3年以上寛解を維持
Rassnick , Vet Comp Oncol, 2010
埼玉動物医療センターでは
L-CHOP-CCNU-AOPP
導入期
維持期
61
62
63
64
65
66
12
LOPP導入プロトコール
2017年の報告
ロムスチン
(L),
オンコビン
(O),
プロカルバジン
(P),
Pre
(P)
変更型LOPP導入プロトコール
2018年の報告
O R I G I N A L A R T I C L ECanine T cell lymphoma treated w ith lomustine, vincristine, procarbazine, and prednisolon e chemotherapy in 35 dogs
E. M organ | K. O'Connell | M . Thomson | A. Griffin D epartment of Oncology, Animal Referral
H ospital Brisbane, Brisbane, Australia Corresp ondence E. M organ, D epartment of Oncology, Animal Referral H ospital Brisbane, 532 Seventeen M ile Rocks Road, Sinnamon Park, Queensland, 4073, Brisbane, Australia. Email: elizabeth.m organ1@ uq connect.edu. au
Canine T cell lymphoma has previously been found to be a poor prognostic indicato r compared w ith its B cell counterpart. The cyclopho sphamide, doxorubicin, vincristine, and prednisolon e protoco l is w idely accepted as a first line treatment for canine lymphoma. There have been sev-eral studies investigatin g alternative protoco ls for T cell lymphoma. This study investigated the use of a modified lomustine, vincristine, procarbazin e and prednisolo ne protocol as a first line treatm ent in 35 dogs w ith T Cell lymphoma. M edian progression free survival (PFS) time for all 35 dogs w as 431 days w ith a 6-month, 1-year, 2-year, and 3-year PFS of 69% , 54% , 29% , and 12% . M edian survival time (M ST) w as 507 days. Tw enty-nine dogs attained a complete response and had a median PFS time of 509 days. Thirty dogs experienced adverse events dur-ing the protoco l, w ith 73% of these bedur-ing grade 1 or 2. This protocol has show n increased median PFS time and M ST compared w ith previous studies and suggests its use as a first line chemotherapy protocol against canine T cell lymphoma.
K E Y W O R D S
canine, chemotherapy, LOPP, oncology, T cell lymphoma
1 | I N TR O D U C TI O N
Lymphoma is one of the most common neoplasm s in the dog w ith the reports of an annual incidence range of 13 to 24 per 100 000 dogs at risk.1The incidence of T cell lymphoma has been reported to range from 13% to 39% .2–10M any studies have investigated the treatment of lymphoma, w ith T cell lymphoma having a poorer prognosis w hen compared w ith B cell lymphoma, w hen treated w ith the same protocol.4–6,8,11Patients w ith T cell lymphoma have a low er complete response (CR) rate, median progression free survival (PFS) time, and median survival time (M ST) in many studies.
Studies using chemotherapy protocols, including cyclophosp ha-mide, doxorubicin, vincristine and prednisolon e (CH OP), modified CH OP, mechloreth amine, vincristine, prednisolone and procarbazine (M OPP), vincristine, L-asparaginase, cyclophosp hamide, doxorubicin and prednisolo ne (VELCAP-L), and single agent protocols, have found that dogs w ith T cell lymphoma did poorly w hen compared w ith dogs w ith B cell lymphoma. In these studies, M ST for dogs w ith T cell lym-phoma ranged from 120 to 237 days and median PFS ranged from 104 to 200 days.4–6,8,11
In 2010, Beaver et al7found w hen treated w ith a single dose of doxorubicin there w as an overall response rate of 50% in dogs w ith T cell lymphoma compared w ith 100%in the dogs w ith B cell
lymphoma. Zandvliet et al12found that drug resistance occurred in 55.6% of dogs w ith lymphoma. Chemotherapy resistance has been associated w ith active efflux of cytotoxic drugs by transporter pro-teins of the ATP-binding cassette (ABC) family. They found that dogs w ith T cell lymphoma had higher intrinsic drug resistance than dogs w ith B cell lymphoma and dogs w ith drug resistant T cell lymphoma had increased ABCG2 mRN A expression. ABCG2 plays a role in trans-port and cellular sensitivity to doxorubicin and has been associated w ith doxorubicin resistance in humans.12These findings suggest that dogs w ith T cell lymphoma are less sensitive to doxorubicin and require non-doxo rubicin-based protoco ls for the treatment of this disease.
Ow ing to the poor response to standard chemotherapy protocols, several studies investigating the responses of T cell lymphoma to alternate chemotherapy protocols have been performed. Protocols investigated include L-asparaginase and M OPP, vincristine, L-aspara-ginase, cyclophosp hamide, lomustin e, doxorubicin, prednisolo ne, pro-carbazine andmechlorethamine(VELCAP-TSC) andlomustine, vincristine, procarbazin e and prednisolo ne (LOPP). These studies found improved overall M ST ranging from 237 to 323 days.13–16
The poor response of T cell lymphoma to the commonly used chemotherapy protoco ls and the high incidence of the disease justify further research into treatment options for this disease. This study Received : 10 M ay 2018 Revised: 2 July 2018 Accepted : 4 July 2018
D OI: 10.1111/vco.12430
Vet Comp Oncol. 2018;1 –8. w ileyonlinelibrary.com /journal/vco © 2018 John W iley & Sons Ltd 1
Vet Comp Oncol. 2018
2017年のLOPP
2018年の変更型LOPP
5.5サイクル(23週間)
変更型LOPP
多中心型 vs それ以外
Morgan,Vet Comp Oncol 2018
多中心型:512日 多中心型以外:76日
無進行生存期間
T細胞性多中心型リンパ腫の
導入プロトコールのまとめ
症例数 奏功率 (%) CR率 (%) CR期間 中央値 引用 LOPP 25 96 92 168 Brown, Vet Comp Oncol2017
変更型LOPP 24 (35)
94 83 512 Morgan,
Vet Comp Oncol 2018
VELCAP-TSC 70 73 64 175 Goodman, The Vet J 2016 L-MOPP 50 98 78 ND Brodsky,
J Vet Inter Med 2009
L-CHOP-CCNU-MOPP
16 126 Rassnick
Vet Comp Oncol 2010 L-CHOP 24 96 88 104 Rebhun,
Vet Comp Oncol 2010 ※ ※ ※多中心型以外のリンパ腫が11例含まれている
クローナリティー検査の意義
◼犬の多中心型リンパ腫では,TとBを識
別する意義はある
◼T細胞性リンパ腫の治療はCHOPでは
不十分
◼
T細胞性リンパ腫ではプロトコールも
変えるべきかも!
67
68
69
70
71
72
2019/3/8
13
ボクサーの予後は悪い?
Morgan,Vet Comp Oncol 2018 ボクサー ボクサー以外 ボ ク サ ー ボクサー以外 Goodman,The Vet J 2016 変更型LOPP VELCAP-TSC
犬多中心型リンパ腫の
レスキュープロトコール
DMACプロトコール
薬用量 投与経路 Day1 Day8 アクチノマイシンD 0.75mg/m2 10分かけてIV○
シトシンアラビノシド 300mg/m2 4時間かけてIV またはSC○
デキサメサゾン 1.0mg/kg IV○
○
※ メルファラン 20mg/m2 PO○
血液検査 CBC 血液化学検査 CBC ※ 5サイクル目以降はクロラムブシル20mg/m2に変更変更型DMAC (小嶋ら)
薬用量 投与経路 Day 1 Day 8 Day 15
アクチノマイシンD 0.56mg/m2 10分かけて IV
○
シトシンアラビノシド 225mg/m2 4時間かけて IV○
デキサメサゾン 1.0mg/kg IV○
○
メルファラン 20mg/m2 PO○
血液検査 CBC 血液化学検査 CBC CBC ※ 5サイクル目以降はクロラムブシル20mg/m2に変更 小嶋,動物臨床医学会年次大会, Proc, 2011DOX・DITCプロトコール
Week1 ドキソルビシン:30mg/㎡ 10mgのドキソルビシンを生食5mlで溶解(2mg/ml) 計算量を生理食塩水50-100mlに溶解して20分以上かけて点滴 デキサメサゾン1mg/kg IV,ブトルファノール0.4mg/kg IM ダカルバジン :800 mg/㎡ 8時間以上かけて点滴静注 メトクロプラミド0.5mg/kg BID 7日間 Week2 CBC Week3 CBC,心エコー *治療に対する反応(CR or PR)が維持され、有害反応から回復していれば上記を繰り返す Vechten, JVIM, 1990LOPP-UFとLOPP
Drug Dose Day
ロムスチン 50-60mg/m2 0 VCR 0.5-0.6mg/m2 0 and 14 プロカル バジン 50mg/m2 0-14 Pre 40mg/m2 0-14 Dose Day 60-70mg/m2 0 0.7mg/m2 0 and 7 50mg/m2 0-14 30mg/m2 0-14
LOPP-UF 2011
LOPP 2007
73
74
75
76
77
78
14
AOPPプロトコール(変更型MOPP)
Day0
アクチノマイシD
0.5mg/m
2IV(10分かけて投与)
ビンクリスチン
0.7mg/m
2IV
プロカルバジン
50mg/m
2PO SID × 7日
プレトドニゾン
20mg/m
2PO SID × 7日
Day7:上記と同様の治療
Day14 CBCのみ(休薬)
Day21 休薬
Day28 上記サイクルを繰り返す
犬リンパ腫レスキュープロトコールまとめ
症例数 奏功率 % CR % 完全寛解期間 (中央値) 引用 MOPP 117 65 31 63日 Rassnick,JVIM, 2002 ミトキサントロン 34 15 41 47 26 47 126日 84日 Moore, JAVMA, 1994 Lucroy, JVIM, 1998 ドキソルビシン+ダカルバジン アントラサイクリン+ダカルバジン 15 42 53 71 33 63 記載なし 85日(CR+PR) Vechten, JVIM, 1990 Dervisis,JAVMA,2007 CCNU 43 27 7 110日 Moore, JVIM, 1999アクチノマイシンD 12 25 83 0 42 0 63日 0日 Hammer, JVIM, 1994 Moore, JVIM, 1994 DMAC (Franciscoら) DMAC (小嶋ら) 54 16 72 43.7 44 31.2 112日 21日 Alvarez, JVIM, 2006 小嶋, 動臨研Proc, 2011 LOPP LOPP-UF 23 33 52 61 27 36 112日 記載なし LeBlanc,Vet Comp, 2006 Fahey, JAVMA, 2011 LAP 1※ LAP 2(変更型) 31 48 87 77 52 65 111日 90日 Saba, JVIM, 2007 Saba, JVIM, 2009 ダカルバジン+CCNU 57 35 23 83日 Flory, JVIM, 2008
ダカルバジン 40 35 2.5 43日(CR+PR) Griessmayr, JVIM, 2009 ※LAP1は,L-アスパラギナーゼを2サイクルで終了
LPPプロトコール
◼
ロムスチン(L)
◼
プロカルバジン(P)
◼
プレドニゾロン(P)
• LOPPからオンコビンを抜いたプロトコール
• CHOPが効かない=オンコビンはもう効かない
副作用が増すだけ
Tanis, Vet Comp Oncol, 2018
LPPプロトコール
◼
41例の再発した多中心型リンパ腫
◼
奏功率:61%(CR 12例,PR 13例)
Tanis, Vet Comp Oncol, 2018
治療開始から中止までの日数
Tanis, Vet Comp Oncol, 2018
CR(中央値84日) PR(58日) SD +PD (21日)
低悪性度 多中心型リンパ腫
(小細胞型)
79
80
81
82
83
84
2019/3/8
15
低悪性度 多中心型リンパ腫の治療
◼
症状の軽いものは無治療
◼クロラムブシル+プレドニゾロン
◼メルファラン+プレドニゾロン
辻本元,高分化型リンハ腫治療のガイドライン,2008 K. E. Flood-Knapik, Vet Comp Oncol,2012 Fujino, JSAP,2006低悪性度 多中心型リンパ腫の
治療ガイドライン
◼
リンパ節の腫脹によって臨床症状が発現している場合
(呼吸困難など)
◼
著しい臓器腫大が認められる場合
◼
血球減少症が認められる場合
◼
単クローン性高ガンマグロブリン血症が認められる場合
◼
食欲低下・衰弱・体重減少などの全身症状が存在する時
辻本元,高分化型リンハ腫治療のガイドライン,2008低悪性度 多中心型リンパ腫の
治療成績
◼
報告が少ない
◼
国内の報告:16頭の犬
◼
生存期間の中央値:938日(約2年半)
◼
治療途中で高悪性度リンパ腫を発症した犬が存在
Takahashi, Veterinary Oncology, 2014
Clinical, histopathological and
immunohistochemical characterization of
canine
indolent lymphoma
◼
75頭のindolent lymphoma についての回顧的研究
◼
T-zoneリンパ腫61.7%,Marginal zoneリンパ腫25%
◼
生存期間の中央値
◼
全体:4.4年
◼
CHOP:21.6カ月
◼
クロラムブシル+Pre:中央値に達せず
◼
T-zone(33.5カ月)とMarginal-zone(21.2カ月)の生
存期間に有意差なし
K. E. Flood-Knapik, Vet Comp Oncol,2012
CHOP vs クロラムブシル+Pre
クロラムブシル+Pre CHOP症 例
◼
ラブラドール・レトリーバー
◼
11歳齢
◼
雄(去勢済み)
◼
食欲不振,下痢,腹囲膨満(3日前から)
◼
多飲多尿
85
86
87
88
89
90
16
初診時一般身体検査
◼
体重 38.1 kg
◼
体温 38.8 ℃
◼
腹囲膨満
◼
体表リンパ節腫脹なし
CBC
RBC(×10
6/μl)
4.92
Hb(g/dl)
12.3
PCV(%)
33
MCV(fl)
70.3
MCHC(g/dl)
35.5
Plat(×10
3/μl) 111
TP(g/dl)
6.4
WBC(/dl)
90 300
Band
0
Seg
19 415
Lym
69 983
Mono
903
Eos
0
血液塗抹
成熟リンパ球の増加
血液化学検査
TP(g/dl)
5.5
Alb(g/dl)
2.4
Glb(g/dl)
3.1
Glu(mg/dl)
96
ALT(U/l)
284
AST(U/l)
98
ALP (U/l)
467
GGT (U/l)
9
TCho(mg/dl)
100
NH
3(μg/dl)
81
TBil (mg/dl)
0.3
BUN(mg/dl)
26.7
Cre(mg/dl)
0.7
Ca(mg/dl)
10.4
Na(mmol/l)
146.1
K(mmol/l)
3.67
Cl(mmol/l)
112.6
血液凝固・線溶系検査
PT
10.9
sec
(7.4‐8.8)
APTT
21.3 sec
(12.0‐28.0)
Fibrinogen
93
mg/dl
(150 ‐350)
FDP
50
μg/ml ( <5 )
AT活性
80
%
( >95 )
参照値
DICと判断
◼ 腹腔内コントラストの低下 ◼ 脾腫 ◼ 胸部特異所見なし91
92
93
94
95
96
2019/3/8
17
◼腹部
◼腹水貯留あり ◼脾臓に腫瘤性病変(2ヵ所) 脾臓 ◼心臓
◼ 特異所見なし腹水検査
多数の成熟リンパ球の出現
沈渣塗抹 高倍治療・経過
暫定診断:高分化型リンパ腫/CLL
第1病日
低分子へパリンCRI
Lアスパラギナーゼ(400U/kg)
デキサメサゾン(1mg/kg)
第2病日
血漿輸血 低分子へパリンCRI
骨髄穿刺
骨髄検査
正~過形成髄
軽度なリンパ球の増殖
(20‐30%)
T細胞性のクローナリティあり(末梢血)
診 断
◼
T細胞性高分化型リンパ腫
/慢性リンパ性白血病
◼
DIC併発
治療経過①
治療開始後1ヵ月の推移
0 20000 40000 60000 80000 1 3 5 7 9 11 13 15 17 19 21 23 25 27 Lym 血漿輸血 L AS デキサメサゾン プレドニゾロン クロラムブシル 20mg/m2SID 6.2mg/m2SID 15mg/m2SID リンパ球数 (/μL) (日) 腹水貯留改善 骨髄穿刺 一般状態安定 退院 入院治療97
98
99
100
101
102
18
治療経過②
月ごとの推移
0 500 1000 1500 2000 1 2 3 4 5 6 7 8 lym リンパ球数 (/μL) 病月 プレドニゾロン クロラムブシル 10mg/m2EOD 2mg/m2EOD 2mg/m23日に1回 一般状態良好 再発兆候なし 休薬症例まとめ
◼
T細胞性高分化型リンパ腫/CLL
◼
腹水貯留,DIC併発,一般状態の低下
◼
L-アスパラギナーゼが著効
◼
クロラムブシルにより良好に維持
教訓
◼
低悪性度リンパ腫(CLL)でもDICを発症する
◼
エマージェンシードラッグとしてL-アスは有効
症
例
12歳齢,ゴールデン・レトリーバー,去勢雄
主訴:顔が腫れている
下顎リンパ節腫脹
下顎リンパ節細胞診⇒低悪性度リンパ腫を疑う低悪性度リンパ腫
病理組織学的診断書
病理組織検査/ノ ース ラ ボ 札幌市厚別区厚別西2 条4 丁目 2 -1 0 -2 F 〒0 0 4 -0 0 6 2 TEL(0 1 1 )8 9 2 -4 6 6 7 FA X (0 1 1 )8 9 2 -4 6 7 0 0 3 7 3 4 BP1 1 -2 6 9 0 2 0 1 1 /0 3 /1 0 2 0 1 1 /0 3 /1 5 受付番号 受付日 報告日 《 》2 4 7 3 5 8 -0 0 0 2 埼玉県入間市東町7 -2 -7 埼玉動物医療セン タ ー 御中 口腔内粘膜側、 皮膚側、 下顎リ ン パ節: リ ン パ腫 lym p h o m a 結腸、 直腸: 著変認めず 病理組織診断 口腔粘膜側、 皮膚側から 採取さ れたいずれの検査 組織でも 、 粘膜浅層から 深部にかけて 、 シ ート 状に 配列する 異型な 円形細胞の腫瘍性増殖が認めら れま す。 下顎リ ン パ節でも 同様の細胞形態を 示す異型細 胞のびま ん性増殖が起こ っ て いま すが。 皮膚側の真 皮には異型細胞の増殖は認めら れま せん。 こ れら の 円形細胞は中型から やや小型で 、 少量の細胞質と 結 節状のク ロ マチン と 小型核小体を 有する 類円形核を 有し 、 軽度な大小不同を 示し て いま す。 結腸、 直腸の粘膜構造はいずれも 良好に保たれて いま す。 直腸で は、 粘液分泌の軽度な 亢進が起こ っ て いま す。 口腔内腫瘤 送付組織: タ ケムラ 飼い主: イ ヌ 動物種: 種類:ゴ ールデ ンレトリバ ー 年齢: 1 2 Y 性別:♂C ペッ ト 名: サブ ロ ウ 様 カ ルテ N o : 診断医 担当医: 福島 先生 〒 ち ゃ ん 口腔粘膜およ び下顎リ ン パ節には、 中程度分化から 高分化なリ ン パ腫の病変が確認さ れま す。 採取さ れた皮膚にリ ン パ腫の病変は認めら れま せん。 今後、 全身性に病変が波及する 可能 性が否定でき ないため、 予後には注意が必要です。 直腸、 結腸に腫瘍性病変は認めら れま せ ん。 肉眼写真の送付:p h o to @ n o rth la b .n et 診断内容: 賀川由美子、 山上哲史 n o rth la b @ m e.co m *診断書を 学会な ど で使用さ れる 場合は、 事前にご 連絡く ださ い。 *ホルマリ ン 組織は、 受付後3 0 日間保存し て いま す。 返却が必要な場合は、 連絡し て く ださ い。 *組織ブ ロ ッ ク の返却は行っ て いま せんので 、 ご 了承お願いいたし ま す。 下顎リンパ節切除生検 口唇粘膜切開生検 ⬇ T細胞型低悪性度リンパ腫低悪性度リンパ腫
クロラムブシル+プレドニゾロンで治療後約1ヵ月後
⇩
治療開始後約2年生存
症
例
◼
10歳8カ月齢
◼
雌
◼
ゴールデン・レトリーバー
103
104
105
106
107
108
2019/3/8
19
主
訴
皮膚のただれ
身体検査所見
◼
体重:38.95kg
◼
体温:39.6℃
◼
聴診:LevineⅡ/Ⅵ
◼
所見:体表リンパ節腫脹
右 左 下顎 4.0×3.7×4.0 5.0×5.2×5.0 5.2×3.5×5.3 8.0×6.0×7.0 4.5×2.8×3.2 3.6×3.6×3.0 7.7×4.5×6.5 浅頚 4.0×5.5×4.0 4.0×4.0×4.0 腋窩 触知できず 1.0×1.0×1.0 鼠径 3.5×4.5×4.5 1.7×3.5×1.7 膝窩 3.5×3.5×3.8 3.0×3.5×4.0体表リンパ節(単位:cm)
CBC(第1病日)
RBC(×10
6/μl)
5.41 WBC(/dl)
97 400
Hb(g/dl)
13.6 Band-N
0
PCV(%)
34
Seg-N
6 493
MCV(fl)
73 Lym
88 309
MCHC(%)
34.5 Mono
2 164
Plat(×10
3/μl)
40.2 Eos
432
TP(g/dl)
7.6 Bas
0
×400 ×1000血液塗抹
血液化学検査(第1病日)
TP(g/dl)
6.9 Glu(mg/dl)
100
Alb(g/dl)
3.0 BUN(mg/dl)
13.7
ALT(U/l)
14 Cre(mg/dl)
0.9
AST(U/l)
22 Ca(mg/dl)
10.4
ALP(U/l)
238 Na(mmol/l)
154.9
TCho(mg/dl)
273 K(mmol/l)
4.60
CK(U/l)
138 Cl(mmol/l)
102.1
臨床検査所見
◼
画像検査:肝臓,脾臓腫大
◼
皮膚検査:毛包虫(+)
◼
血液凝固系検査:正常
109
110
111
112
113
114
20
×400 ×1000体表リンパ節FNA
T細胞性のクローなりティー有り
×400 ×1000脾臓FNA
肝臓FNA
暫定診断
T細胞性高分化型リンパ腫/CLL
※
リンパ節生検は未実施
家族の希望
麻酔のリスク高い
治 療
◼
クロラムブシル
6mg/m2 sid 14日間
→6mg/m2 eod 維持
◼
プレドニゾロン
30mg/m2 sid 7日間
→20mg/m2 sid 7日間
→10mg/m2 eod 維持
◼
イベルメクチン
本例の教訓
◼
毛包虫を見つけたら高分化型リンパ腫は鑑別
に入れる
◼
生検ができない場合は総合的に診断する
115
116
117
118
119
120
2019/3/8
21
消化器型リンパ腫
高悪性度
消化器型リンパ腫
高悪性度
消化器型リンパ腫
◼
慢性消化器症状
◼
体重減少,無気力,元気,食欲低下,嘔吐,下痢
◼
低タンパク血症
◼
B 細胞性も T 細胞性もある
高悪性度
消化器型リンパ腫
診断のピットホール
◼
超音波所見で異常がなくてもリンパ腫は否定で
きない!
◼
内視鏡診断の重要性
犬の消化器型リンパ腫 vs 超音波検査
15頭の消化器型リンパ腫の回顧的研究
◼
26.7%が超音波所見に異常なし
◼
異常が見られた犬も所見はバラバラ
Frances M, JSAP , 2013犬の消化器型リンパ腫
超音波検査
1.
腫瘤形成型(串団子型)→外科検討
2.
びまん性肥厚型(きりたんぽ型)
3.
腸間膜リンパ節腫大型
4.
異常所見があまり出ないタイプ
5.
121
122
123
124
125
126
22
串団子型
高悪性度 消化器型リンパ腫
予後
◼
抗がん治療の成績(18頭の犬の研究)
◼
多剤併用プロトコール(VELCAP-SC)
◼
奏功率56%(CR 9頭,PR 1頭)
◼
寛解期間の中央値 86日
◼
生存期間の中央値 77日
◼
T細胞性とB細胞性との生存期間に有意差なし
◼
T細胞性:10頭
◼
B細胞性:6頭
◼
2頭は未実施
Rassnick KM , JVIM , 2009L-ASPの連続投与
◼
大細胞性胃腸管型リンパ腫の犬45症例
◼
L-ASPを連続投与:中央値6回(範囲:1-
30
)
◼
治療効果の判定は32例で実施
◼
奏功率:56%(CR15例,PR3例)
◼
無進行生存期間:中央値50日(範囲:11-400日)
◼
生存期間の中央値:131日(範囲:2-431日)
◼
全症例で有害事情なし
Kojima, JCVIM Proc, 2019
ニムスチンを初期治療に用いた
消化器型リンパ腫の回顧的研究
◼
31例の消化器型リンパ腫の犬
◼
奏功率:31%
◼
生存期間の中央値63日
◼
CHOPより消化器毒性は少ない
◼
注射なのでロムスチンより使いやすい
Harada, JCVIM Proc, 2019
猫では
無憎悪生存期間の中央値:357日
Gouldin, Vet Comp Oncol 2017
外科切除後に化学療法を行うと長期生存
127
128
129
130
2019/3/8
23
犬の消化器型リンパ腫の
予後は厳しい…
だが,しかし…
M・ダックスフンドの
高悪性度 消化器型リンパ腫
◼
若齢で発症するケースが多い(平均約3歳齢)
◼
長期生存例が多い?
◼
抗がん剤の反応比較的良好
◼
予後の悪いものもいるが理由は?
◼
まとまった報告はない!
◼
日本だけ??
M・ダックスの
リンパ腫の特徴 ?
◼
少し前は・・・
<M・ダックスのリンパ腫38症例の報告>
➢
若齢での発症が多い
➢
平均年齢3.6歳,63%が3歳未満
➢
雄に多い(75%)
➢
消化器型が多い
➢
長期生存が多い:中央値 868日
Setoguchi,VCS Proc, 2005M・ダックスのリンパ腫@
埼玉動物医療センター
◼
調査期間:2007−2018年
◼
リンパ腫と診断したM・ダックス
23例
◼
平均年齢:9.8歳
◼
3歳以下は4例(18%)
◼3例がMott cell様変化を伴う消化器型
◼1例が脊髄
◼
消化器型は11例
,多中心型4例,皮膚型3例,
肝脾型2頭
◼
性差:雄12例(4),雌11例(3)
Mott cell様の変化を伴う
B細胞性リンパ腫
WHO組織分類で未分類の腫瘍 動物での報告はわずか → 治療法や予後が不明Mott cell
ラッセル小体(免疫グロブリン の蓄積)を細胞質に大量に含む細胞 • 慢性炎症 • 多発性骨髄腫 • 一部のB細胞性リンパ腫Cazzini P et al., Vet Clin Pathol. 2013.
Snyman HN et al., J. Comp. Path. 2013.