成人脊柱変形における重心動揺計を用いた立位バランスの検討
7
0
0
全文
(2) 成人脊柱変形における重心動揺計を用いた立位バランスの検討. 325. total(各ドメインの平均値)の 3 項目とした。 EOS 全脊椎立位正面像の評価項目は胸椎 Cobb 角, 腰椎 Cobb 角,Coronal balance(CB:C7 椎体中心から の鉛直線と仙骨中心からの鉛直線との距離の絶対値)と し,側面像の評価項目は SVA(C7 椎体中央から降ろし た垂線と仙骨後角との距離),Thoracic kyphosis(TK: T4 上縁と Th12 下縁とのなす角度) ,Lumbar lordosis (以下,LL:L1 上縁と S1 上縁のなす角度),Pelvic tilt (以下,PT:大. 骨頭中心と仙骨上縁の中点を結ぶ線と. 垂線のなす角度),Pelvic incidence(PI:S1 終板の垂 直二等分線と,仙骨上縁の中点と大. 骨頭中心とを結ん. だ線とのなす角度),Sacral slope(SS:仙骨上縁と水平 線のなす角度) ,Pelvic incidence minus Lumbar lordosis (以下,PI-LL) ,Knee flex(両膝関節屈曲角度の平均値: 大. 骨頭と大. 骨外側顆の中点を結んだ線と遠位脛骨関. 節面の中点を結んだ線とのなす角度の平均) ,Ankle flex (両足関節背屈角度の平均値:大. 骨外側顆の中心から. 遠位脛骨関節面の中点を結んだ線と遠位脛骨関節面の中. 図 1 重心動揺の測定方法 プラットフォーム上に開眼での両脚立位姿勢 を 60 秒間とり,軌線の揺れを記録する.. 点からの鉛直線とのなす角度の平均)とした た,SRS-Schwab ASD classification. 32)33). 。ま. 34). を用いて Coronal. curve type を 分 類 し た。 内 訳 は T(Thoracic curve type:頂椎が T9 またはそれより頭側に位置し,主胸椎 ≧ 20°または SVA ≧ 50 mm. 21). ず 60 秒以上の立位保持が可能. ,かつ介助を必要とせ. カーブ >30°) ,L(Thoraco lumbar or lumbar curve type:. 27). 頂椎が T10 またはそれより尾側に位置し,主腰椎カー. であった ASD 患者. 46 例を対象とした。ASD 群の平均年齢は 67.4 ± 10.0 歳. ブ >30°),D(Double curve type:胸腰椎カーブ >30°),. (44 ‒ 82),平均 Body mass index(以下,BMI)は 22.5. N(No major coronal deformity:胸腰椎カーブ <30°). 2. ± 3.2 kg/m であった。既往歴にパーキンソン病などの. である。. 神経筋疾患および脳血管疾患などの中枢神経障害,脊椎. 本研究では,まず ASD 群と control 群の重心動揺の. 手術歴,下肢人工関節手術歴を有する症例を除外した。. 測定項目について 2 群比較を行った。さらに,ASD 群. また,下肢神経根症状は重心動揺に影響を与える. 28). た. を SVA <100 mm 群と SVA >100 mm 群の 2 群に分け. め,本研究において除外基準に追加した。対照群として,. 脊椎骨盤および下肢アライメントパラメータ,SRS-22,. 年齢を一致させた健常女性(control 群)21 例(平均年. 重心動揺の測定項目について 2 群比較を行った。統計処. 2 齢 67.4 ± 6.1 歳(55 ‒ 81),平均 BMI 21.6 ± 3.4 kg/m ). 理は Shapiro-Wilk 検定を行ったうえで,対応のない t. を用いた。なお,本研究は名城病院倫理委員会の承認. 検定または Mann-Whitney U 検定を用い,有意水準は. (承認番号 134)を得て実施し,すべての対象者には評. 5% とした。解析ソフトは R2.8.1(CRAN, freeware)を. 価の目的,方法,リスクについて文書,口頭による説明 を十分に行い,同意を得た。 重心動揺検査は重心動揺計(ANIMA 社製,グラビ. 使用した。 結 果. コーダー G620)を用い,外周面積,総軌跡長を測定した。. 対象の基本属性,脊椎骨盤および下肢アライメントパ. 外周面積は重心動揺の軌跡の最外郭によって囲まれる内. ラメータ,SRS-22 の結果を表 1 に示す。ASD 群における. 側の面積であり,総軌跡長は重心点の移動した全長であ. SRS-Schwab ASD classification の内訳は T:2 例(4.3%) ,. 22). 。測定肢位は足長の中央をプラットフォームの中. L:19 例(41.3%) ,D:9 例(19.6%) ,N:16 例(34.8%). 央に置いた開眼閉脚立位とし,200 cm 前方に設置した. であり,L と N の合計は 35 例(76%)と多数を占めた。. る. 指標を注視させ. 29). ,60 秒間の立位保持を行った(図 1) 。. 重心動揺の結果は,外周面積の平均値は ASD 群が 5.3 ±. 測定する環境は無音状態になるよう留意して行った。. 2 2 3.9 cm に対し,control 群が 3.3 ± 1.1 cm であり,ASD. 臨床的評価は,HRQOL として Scoliosis research soci-. 群の重心動揺は有意に大きかった(P = 0.001) 。また,総. 30)31). を用. 軌 跡 長 の 平 均 値 は ASD 群 が 115.7 ± 44.1 cm に 対 し て. いた。評価項目はサブドメインである function,pain と. control 群が 85.3 ± 19.8 cm であり,ASD 群は control 群. ety-22 patient questionnaire(以下,SRS-22).
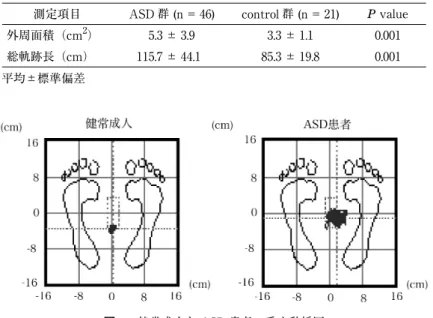
(3) 326. 理学療法学 第 47 巻第 4 号. 表 1 ASD 群と control 群の基本属性,脊椎骨盤および下肢アライメントパラメータと SRS-22 基本属性 SRS-Schwab ASD classification. ASD 群 (n = 46). control 群 (n = 21). 年齢 ( 歳 ). 67.4 ± 10.0 (44 ‒ 82). 67.4 ± 6.1 (55 ‒ 81). BMI (kg/m2). 22.5 ± 3.2 (15.0 ‒ 28.7). 21.6 ± 3.4 (14.7 ‒ 29.6). Curve type. T:2 例 L:19 例 D:9 例 N:16 例. 脊椎骨盤アライメント. 下肢アライメント SRS-22. 胸椎 Cobb 角 (°). 23.4 ± 21.5 (2 ‒ 85). 5.4 ± 3.1 (1 ‒ 11). 腰椎 Cobb 角 (°). 36.7 ± 18.2 (1 ‒ 82). 4.6 ± 2.6 (1 ‒ 9). CB (mm). 29.7 ± 31.1 (2.3 ‒ 70.5). SVA (mm). 86.2 ± 59.9 (4 ‒ 258). 21.3 ± 17.8 (‒3.1 ‒ 48.0). TK (°). 30.9 ± 21.3 (2 ‒ 66). 27.2 ± 13.5 (7 ‒ 53). LL (°). 19.9 ± 23.6 (‒56 ‒ 47). 41.4 ± 14.1 (14 ‒ 61). PT (°). 31.1 ± 10.3 (10 ‒ 56). 21.6 ± 8.8 (9 ‒ 39). PI (°). 50.9 ± 11.2 (27 ‒ 71). 52.6 ± 11.2 (30 ‒ 71). SS (°). 19.8 ± 11.1 (‒5 ‒ 46). 31.5 ± 9.4 (6 ‒ 42). PI-LL (°). 31.0 ± 24.7 (8 ‒ 74). 11.2 ± 13.9 (‒9 ‒ 49). Knee flex (°). 10.7 ± 9.9 (‒5 ‒ 49). 2.7 ± 4.4 (‒4 ‒ 17). Ankle flex (°). 10.3 ± 12.6 (0 ‒ 27). 5.3 ± 3.4 (‒2 ‒ 13). function. 3.2 ± 0.9 (1.8 ‒ 4.6). pain. 3.1 ± 0.8 (1.4 ‒ 4.6). total. 2.9 ± 0.7 (1.0 ‒ 4.4). 8.1 ± 5.2 (1.3 ‒ 20.3). 平均値±標準偏差(範囲) BMI: body mass index,T: thoracic curve type,L: thoracolumbar or lumbar curve type,D: double curve type, N: no major coronal deformity CB: coronal balance,SVA: sagittal vertical axis,TK: thoracic kyphosis,LL: lumbar lordosis,PT: pelvic tilt,PI: pelvic incidence,SS: sacral slope,PI-LL: pelvic incidence minus lumbar lordosis.. 表 2 ASD 群と control 群における重心動揺の比較 測定項目. ASD 群 (n = 46) 2. control 群 (n = 21). P value. 外周面積(cm ). 5.3 ± 3.9. 3.3 ± 1.1. 0.001. 総軌跡長(cm). 115.7 ± 44.1. 85.3 ± 19.8. 0.001. 平均±標準偏差. 図 2 健常成人と ASD 患者の重心動揺図 健常成人は軌線の揺れはほとんどないが,ASD 患者では軌線の揺れが大きくなっている.. よりも有意に大きな値を示した(P = 0.001) (表 2) 。健常. 盤 お よ び 下 肢 ア ラ イ メ ン ト パ ラ メ ー タ の 比 較 で は,. 成人と ASD 患者の代表的な重心動揺図を示す(図 2) 。. SVA >100 mm 群 は SVA <100 mm 群 に 比 し PT,PI-. ASD 群 に お い て SVA >100 mm 群 は 17 例,SVA. LL,Knee flex が有意に大きな値を示した(P < 0.05). <100 mm 群は 29 例であった。ASD 群における脊椎骨. が,他のパラメータに有意差はなかった。SRS-22 の値.
(4) 成人脊柱変形における重心動揺計を用いた立位バランスの検討. 327. 表 3 ASD 群の SVA 分類による脊椎骨盤および下肢アライメントパラメータと SRS-22 の比較 SVA >100 mm (n= 17) 脊椎骨盤アライメント. 胸椎 Cobb 角 (°). SRS-22. 25.2 ± 22.4 (2 ‒ 85). 0.473. 腰椎 Cobb 角 (°). 36.5 ± 18.8 (1 ‒ 66). 36.8 ± 18.2 (1 ‒ 82). 0.959. CB (mm). 44.2 ± 45.6 (2.3 ‒ 180). 21.3 ± 12.7 (2.3 ‒ 50.1). 0.140. 50.2 ± 25.2 (4 ‒ 91). < 0.001. TK (°). 147.6 ± 51.3 (102 ‒ 258) 35.1 ± 23.4 (3 ‒ 92). 28.5 ± 20.1(2 ‒ 66). 0.318. LL (°). 14.5 ± 24.0 (‒47 ‒ 62). 23.1 ± 23.1 (‒35 ‒ 68). 0.232. PT (°). 37.7 ± 6.4 (27 ‒ 48). 27.3 ± 10.2 (10 ‒ 56). < 0.001. PI (°). 54.6 ± 8.6 (43 ‒ 71). 48.7 ± 12.1 (27 ‒ 76). 0.086. SS (°). 16.8 ± 10.5 (‒5 ‒ 32). 21.6 ± 11.3 (‒5 ‒ 46). 0.160. PI-LL (°). 40.1 ± 27.5 (‒19 ‒ 118). 25.6 ± 21.6 (‒5 ‒ 77). 0.036. Knee flex (°). 17.9 ± 10.3 (6 ‒ 49). 6.7 ± 6.8 (‒5 ‒ 25). < 0.001. Ankle flex (°). 10.6 ± 5.8 (3 ‒ 27). 7.4 ± 3.9 (0 ‒ 17). 0.099. SVA (mm). 下肢アライメント. P value. SVA <100 mm (n= 29). 20.2 ± 20.1 (2 ‒ 85). function. 3.0 ± 0.9 (1.8 ‒ 4.5). 3.4 ± 0.9 (1.8 ‒ 4.6). 0.146. pain. 2.8 ± 0.6 (1.6 ‒ 4.0). 3.2 ± 0.9 (1.4 ‒ 4.6). 0.115. total. 2.8 ± 0.6 (1.5 ‒ 3.5). 3.0 ± 0.8 (1.0 ‒ 4.1). 0.120. 平均値±標準偏差(範囲) CB: coronal balance,SVA: sagittal vertical axis,TK: thoracic kyphosis,LL: lumbar lordosis,PT: pelvic tilt,PI: pelvic incidence,SS: sacral slope,PI-LL: pelvic incidence minus lumbar lordosis.. 表 4 ASD 群における SVA と重心動揺との関係 SVA < 100 mm (n = 29). > 100 mm (n = 17). P value. 2 外周面積(cm ). 4.6 ± 2.7. 6.5 ± 5.3. 0.015. 総軌跡長(cm). 98.7 ± 28.6. 144.6 ± 51.4. 0.002. 測定項目. 平均±標準偏差. は SVA >100 mm が function 3.0 ± 0.9, pain 2.8 ± 0.6,. ASD における立位バランスの報告は少ない。Yagi ら. total 2.8 ± 0.6 であった。一方,SVA <100 mm は func-. は ASD 女性患者 40 例と年齢を一致させた健常女性成. tion 3.4 ± 0.9, pain 3.2 ± 0.9, total 3.0 ± 0.8 であり,両. 人 33 例を対象に,長さ 10.8 m のフォースプレートを床. 群に有意差を認めなかった(P < 0.05) (表 3) 。また,. 上に設置し,耳垂と第 7 頸椎から第 1 仙椎までの棘突起. 2. 外周面積の平均値は SVA >100 mm 群 6.5 ± 5.3 cm に 2. および上下肢の各関節にマーカーを貼付け,開眼した状. 対 し SVA <100 mm 群 が 4.6 ± 2.7 cm で あ り,SVA. 態で自然立位を 60 秒間保持させた立位バランスを測定. >100 mm 群は有意に動揺が大きかった(P = 0.015) 。総. し た。 そ の 結 果, 外 周 面 積 は 健 常 女 性 成 人 が 1.0 ±. 軌跡長の平均値は SVA >100 mm 群が 144.6 ± 51.4 cm. 2 2 0.8 cm /min に対し ASD 群は 2.4 ± 2.6 cm /min であり,. に 対 し て SVA <100 mm 群 が 98.7 ± 28.6 cm で あ り,. ASD 群は有意に立位バランスが悪化することを報告し. SVA >100 mm 群は SVA <100 mm 群よりも有意に大. た. きな値を示した(P = 0.002)(表 4)。. ンクショナルリーチや片足立ち,歩行など 36 項目から. 考 察. 21). 。また,Moke らは動的バランス評価としてファ. なる BESTest を用い,コントロール群 94.96 ± 6.26% に対し ASD 患者は 81.82 ± 10.38% と低値を示し,ASD 5). 。本. 本研究は,我々が渉猟しうる限りでは ASD に対し重. 患者は動的バランスが有意に悪化すると報告した. 心動揺を用いて立位バランスを評価したはじめての報告. 研究の結果は過去の報告と同様に ASD 群は立位バラン. である。ASD 群は脊柱変形を有しない健常成人と比べ. スが悪化する結果となった。一般に筋力低下は筋反応時. 外周面積と総軌跡長は有意に大きく,重心動揺は悪化し. 間に遅延を生じさせることや,筋反応のタイミングに変. た。また,ASD 群の中でも SVA が 100 mm を超える. 化が生じることが報告されている. 群は 100 mm 未満の群に比べ立位バランスが悪化した。. 比べ傍脊柱起立筋の萎縮や脂肪変性を有する割合が多. 35). 。ASD は健常人に.
(5) 328. 理学療法学 第 47 巻第 4 号. ‒8). く6. ,サルコペニアの有病率が高い 9) ことが認めら. 使用した 9 種類の脊柱伸展運動プログラムを 50 ∼ 59 歳. れている。ASD 群における体幹筋の減少が立位バラン. の女性に実施し,体幹前傾化の進行を遅らせることがで. ス保持に必要な筋活動に遅延を生じさせるために重心動. きると述べている. 揺が大きくなったかもしれない。. 高齢者 34 例を対象に,10 週間の Pilates 運動を実施し,. 今回,ASD 群の中で SVA が 100 mm を超えた著明. 立位時の胸椎後弯角が有意に減少したことを報告した. な体幹前傾を呈した群は 100 mm 未満の群に比べ,立. ハタ・ヨガを取り入れた運動介入は,脊椎後弯角 40 度. 位バランスが悪化する結果であった。重心動揺と脊椎ア. 以上を有する女性患者の体幹前傾角が 4.4% 減少する結. ライメントに関しての報告は散見される。Ishikawa ら. 果を示した. は閉経後骨粗鬆症患者 93 例を対象に,Spinal mouse を. 背筋増強運動や Pilates 運動,ヨガなどの運動プログラ. 用いて脊椎アライメントと重心動揺の相関関係を調査. ムを積極的に実施し,体幹前傾化を防ぐことで良好な立. し,Spinal Inclination は外周面積や総軌跡長と中等度の. 位バランスを維持することができるかもしれない。. 正の相関(r = 0.550,r = 0.434)を認め,脊柱前傾化は. 本研究にはいくつかの limitation が存在する。第 1 に. 22). 。. 単一施設で行われたこと,第 2 に症例が少ないこと,第. Imagama らの高齢男性 100 例を対象とした報告では,. 3 に背筋や下肢などの筋力を測定していないこと,第 4. SVA と開眼における総軌跡長との間で有意な相関関係. に冠状面アライメントパラメータを含めた検討を行って. (r = 0.440)を認めたとしており,体幹の前傾は視線を. いないことである。将来的にはこれらのデータと重心動. 下向きにさせるため,迅速に状況を把握する能力が障害. 揺の結果を精査することにより,脊柱変形と立位バラン. 立位バランス不良と密接に関係することを報告した. されバランスの低下を招くと考察している. 23). 。本研究. において SVA >100 mm 群は,PT と PI-LL,Knee flex が増大し,体幹前傾に対する代償姿勢. 36). を呈していた。. 42). 。また,Kuo らは 60 歳以上の健常 43). 。. 44). 。これらの報告から,脊柱変形患者には. スに関するより深い理解が得られると考えられる。 結 語. 一般に,体幹前傾による PT の増大は股関節伸展モーメ. ASD の立位バランスについて重心動揺を用いて評価し. ントが大きくなり,立位や歩行時において筋疲労が容易. た。ASD 群は脊柱変形を有しない健常成人と比べ重心動. に生じるとされている. 36)37). 。PI-LL の増大は,すなわ. ち LL 減少を意味しており. 38). ,LL 減少により腰背筋群. がつねに受動的に伸展された状態となり,持続的筋活動 が出現する. 。この変化により筋内圧は上昇し,筋血. 39). 。また,下肢関節屈曲位による立位保持は大. 四. 頭筋を中心とした下肢筋群の持続的収縮により,多大な エネルギーを要し立位バランスに影響することが報告さ れている. 群は SVA <100 mm 群に比し立位バランスが悪化する結 果となった。. 39). 流量が減少するため腰背部筋に機能不全を生じさせ る. 揺は悪化した。また,ASD 群の中でも SVA >100 mm. 40). 。本研究において ASD の中の SVA >100 mm. 群は腰背筋群の機能不全や下肢筋群の疲労などが立位バ ランス不良を生じさせたと推測された。 Bess らの先行研究. 12). では,多施設にて The Medical. Outcome Survey Short-Form 36 を用いて ASD の HRQOL を評価しており,SVA が 100 mm 以上の例は 100 mm 以下の例に比べ HRQOL が有意に悪化したことを報告 した。今回,SRS-22 の諸項目において SVA >100 mm 群と SVA <100 mm 群に有意差を認めなかった。対象 や評価項目,測定環境(単一対多施設研究)の違いなど の影響が反映されていると考えられた。 ASD 患者において良好な立位バランスを保持するた めには,体幹前傾化を防ぐ運動療法が重要と考えられ る。Itoi と Sinaki らは 49 ∼ 65 歳の健常女性を対象に前 向き研究を行い,最大背筋力の 30% の重さのバックパッ クを背負い腹臥位にて 10 回持ち上げる方法を導入する ことで,脊柱後弯を改善し,体幹前傾化の予防になるこ とを報告した. 41). 。Ball らは,自宅の床やセラバンドを. 利益相反 開示すべき利益相反はない。 文 献 1)Kado DM, Huang MH, et al.: Hyperkyphotic posture predicts mortality in older community dwelling men and women: a prospective study. J Am Geriatr Soc. 2004; 52: 1662‒1667. 2)Takahashi T, Ishida K, et al.: Trunk deformity is associated with a reduction in outdoor activities of daily living and life satisfaction in community-dwelling older people. Osteoprosis Int. 2005; 16: 273‒279. 3)Aebi M: The adult scoliosis. Eur spine J. 2005; 14: 925‒ 948. 4)Yagi M, Ohne H, et al.: Walking balance and compensatory gait mechanisms in surgically treated patients with adult spinal deformity. Spine J. 2016; 17: 409‒417. 5)Moke L, Severijns M, et al.: Performance on balance evaluations systems test (BESTest) impacts healthrelated quality of life in adult spinal deformity patients. Spine (Phila Pa 1976). 2018; 43: 637‒646. 6)Banno T, Yamato Y, et al.: Assessment of the crosssection areas of the psoas major and multifidus muscles in patients with adult spine deformity. Clin Spine Surg. 2017; 30: 968‒973. 7)Yagi M, Hosogane N, et al.: The paravertebla muscle and psoas for the maintenance of global spinal alignment in patient with degenerative lumbar scoliosis. Spine J. 2016;.
(6) 成人脊柱変形における重心動揺計を用いた立位バランスの検討 16: 451‒458. 8)Lee CS, Lee CK, et al.: Dynamic sagittal imbalance of the spine in degenerative flat back. Spine (Phila Pa 1976). 2001; 26: 2029‒2035. 9)Eguchi Y, Toyoguchi T, et al.: Analysis of skeletal muscle mass in women over 40 with degenerative lumbar scoliosis. Eur spine J. 2018 Dec 4.doi: 10.1007/s00586-0185854-0. 10)Glassman SD, Bridwell K, et al.: The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005; 30: 2024‒2029. 11)Glassman SD, Berven S, et al.: Correlation of radiographic parameters and clinical symptoms in adult scoliosis. Spine (Phila Pa 1976). 2003; 30: 682‒688. 12)Bess S, Line B, et al.: The health impact of symptomatic adult spinal deformity: Comparison of deformity types to united states population norms and chronic disease. Spine (Phila Pa 1976). 2016; 41: 224‒233. 13)Ishikawa Y, Miyakoshi N, et al.: Spinal sagittal contour affecting falls: Cut-off value of the lumbar spine for falls. Gait & posture. 2013; 38: 260‒263. 14)Fujita T, Nakamura S, et al.: Effect of age on body sway assessed by computerized posturograhy. J Bone Miner Metab. 2005; 23: 152‒156. 15)Bauer C, Gröger I, et al.: Intrasession reliability of force platform parameters in community- dwelling older adult. Arch Phys Med Rehabil. 2008; 89: 1977‒1982. 16)Winter D: Human balance and posture control during standing and walking. Gait & Posture. 1995; 3: 193‒214. 17)Wang Z, Ko JH, et al.: The degrees of freedom problem in human standing posture: collective and component dynamics. PLoS One. 2014; 9: e85414. 18)Ogaya S, Okita Y, et al.: Muscle contributions to center of mass excursion in ankle and hip strategies during forward body tilting. J Biomech. 2016; 49: 3381‒3386. 19)Bok SK, Lee TH, et al.: The effects of changes of ankle strength and range of motion according to aging on balance. Ann Rehabil Med. 2013; 37: 10‒16. 20)Boyas S, Hajj M, et al.: Influence of ankle plantarflexor fatigue on postural sway, lower limb articular angles, and postural strategies during unipedal quiet standing. Gait & posture. 2013; 37: 547‒551. 21)Yagi M, Kaneko S, et al.: Standing balance and compensatory mechanisms in patients with adult spine deformity. Spine (Phila Pa 1976). 2017; 42: 584‒591. 22)Ishikawa Y, Miyakoshi N, et al.: Spinal curvature and postural balance in patients with osteoporosis. Osteoporosis Int. 2009; 20: 2049‒2053. 23)Imagama S, Ito Z, et al.: Influence of spinal sagittal alignment, body balance, muscle strength, and physical ability on falling of middle-aged and elderly males. Eur spine J. 2013; 22: 1346‒1353. 24)Dubousset J, Charpak G, et al.: A new 2D and 3D imaging approach to muscleskeletal physiology and pathology with low-dose radiation and the standing position: the EOS system. Bull Acad Natl Med. 2005; 189: 287‒297. 25)Kalifa G, Charpak Y, et al.: Evaluation of a new low-dose digital x-ray device: first dosimetric and clinical results in children. Pediatr Radiol. 1998; 28: 557‒561. 26)Deschenes S, Charron G, et al.: Diagnostic imaging of spinal deformities: reducing patients radiation dose with a new slot-scanning X-ray imager. Spine (Phila Pa 1976).. 329. 2010; 35: 989‒994. 27)Yoshikawa M, Doita M, et al.: Impaired postural stability in patients with cervical myelopathy. Spine (Phila Pa 1976). 2008; 33: 460‒464. 28)Bouche K, Stevens V, et al.: Comparison of postural control in unilateral stance between healthy controls and lumbar discectomy patients with and without pain. Eur spine J. 2006; 15: 423‒432. 29)三森由香子,渡辺航太,他:脊柱の変形部位が静止立位姿 勢制御に及ぼす影響─思春期特発性側弯症のシングルカー ブにおける検討─.理学療法学.2015; 42: 377‒383. 30)Asher M, Min Lai S, et al.: The reliability and concurrent validity of the scoliosis research society-22 patint questionnaire for idiopathic scoliosis. Spine (Phila Pa 1976). 2003; 28: 63‒69. 31)Asher M, Min Lai S, et al.: Refinement of the SRS22 health-related quality of life questionnaire function domain. Spine (Phila Pa 1976). 2006; 31: 593‒597. 32)O’Brien MF, Kuklo TR, et al.: The spinal deformity study group radiographic measurement manual. Memphis, TN: Medtronic Sofamor Danek USA, Inc; 2004. 33)Hasegawa K, Okamoto M, et al.: Normative values of spino-pelvic sagittal alignment, balance, age, and healthrelated quality of life in a cohort of healthy adult subjects. Eur Spine J. 2016; 25: 3675‒3698. 34)Schwab F, Ungar B, et al.: Scoliosis Research Societyschwab adult spinal deformity classification: A validation study. Spine (phila Pa 1976). 2012; 37: 1077‒1082. 35)Allison GT, Henry SM: The influence of fatigue on trunk muscle responses to sudden arm movements, a pilot study. Clin biomech. 2002; 17: 414‒417. 36)Roussouly P, Pinheiro-Franco J: Biomechanical analysis of the spino-pelvic organization and adaptation in pathology. Eur spine J. 2011; 20: S609‒S618. 37)Lazennec JY, Ramare S, et al.: Sagittal alignment in lumbosacral fusion: relations between radiological parameters and pain. Eur spine J. 2000; 9: 47‒55. 38)Arima H, Yamato Y, et al.: Discrepancy between standing posture and sagittal balance during walking in adult spinal deformity patients. Spine (Phila Pa 1976). 2016; 42: 25‒30. 39)Konno S, Kikuchi S, et al.: The relationship between intramuscular pressure of the paraspinal muscle and low back pain. Spine (Phila Pa 1976). 1994; 19: 2186‒2189. 40)Ishikawa Y, Miyakoshi N, et al.: Relationships among spinal mobility and sagittal alignment of spine and lower extremity to quality of life and risk of falls. Gait & posture. 2017; 53: 98‒103. 41)Itoi E, Sinaki M: Effect of back-strengthening exercise on posture in healthy women 49 to 65 years of age. Mayo Clin proc. 1994; 69: 1054‒1059. 42)Ball JM, Cagle P, et al.: Spinal extension exercises prevent natural progression of kyphosis. Osteoporos Int. 2009; 20: 481‒489. 43)Kuo YK, Tully EA, et al.: Sagittal spinal posture after pilates-based exercise in healthy older adults. Spine (Phila Pa 1976). 2009; 34: 1046‒1051. 44)Greendale GA, Huang MH, et al.: Yoga decrease kyphosis in senior women and men with adult onset hyperkyphosis: results of a randomized controlled trial. J Am Geriatr Soc. 2009; 57: 1569‒1579..
(7) 330. 理学療法学 第 47 巻第 4 号. 〈Abstract〉. Impaired Postural Stability in Patients with Adult Spinal Deformity: Evaluation Based on Computerized Stabilometry. Shinya SAKURAI, PT, Kumiko ARAMOTO, PT, Tetsuya OHARA, MD Department of Rehabilitation, Meijo Hospital Hironori TANABE, MD, DMSc, Tetsuya OHARA, MD Department of Orthopaedic & Spine Surgery, Meijo Hospital. Purpose: Recent insights suggest that spinal deformity impacts various functional disorders. However, there are few reports of examinations of postural balance in patients with adult spinal deformity (ASD), and the effect of kyphotic changes in ASD on postural balance remains unclear. The aim of this study was to evaluate standing balance and the influence of kyphotic changes on standing balance in patients with ASD. Method: We investigated 46 female patients with ASD (age: 67.4 ± 10.0 years) and compared the results with those of 21 age-matched healthy female adults. Based on the sagittal vertical axis (SVA), patients were allocated to the SVA >100 mm and SVA <100 mm groups. Postural stability was examined using a stabilometer. Using the stabilometer, the sway of the gravity center was measured at the upright position with eyes open for 60 seconds. We used 2 parameters for evaluation: the enveloped area (ENV), which measures the degree of sway of the gravity center, and total track length (LNG), which measures the sway length in the standing posture. 2 Results: The mean ENV in the patient group was 5.3 ± 3.9 cm , whereas that in the control group was 3.3 2 ± 1.1 cm , revealing significantly larger postural instability in the patient group compared to that in the. control group. The LNG in the patient group was significantly worse than that in the control group. It was also shown that postural instability was significantly larger in the patients with SVA >100 mm than that in patients with SVA <100 mm. Conclusion: The results of the present study demonstrated impairments in postural stability in patients with ASD. In these patients, kyphotic changes were associated with greater postural instability. Therefore, exercises that delay the progression of kyphosis may be crucial for postural stability in patients with ASD. Key Words: Adult spinal deformity, Postural stability, Stabilometry.
(8)
図
関連したドキュメント
The motion ranges of knee angle became small in the order of normal healthy persons, L4 patients and HipOA patients while that of upper body angle became large in the order of
TABLE I~Iv, Fig.2,3に今回検討した試料についての
For quantitative assessment, we calculated the coefficient of variance (CV) of fat region and contrast between fat region, normal tissue, and lesion on MR images acquired using
振動流中および一様 流中に没水 した小口径の直立 円柱周辺の3次 元流体場 に関する数値解析 を行った.円 柱高 さの違いに よる流況および底面せん断力
Wach 加群のモジュライを考えることでクリスタリン表現の局所普遍変形環を構 成し, 最後に一章の計算結果を用いて, 中間重みクリスタリン表現の局所普遍変形
さらに, 会計監査人が独立の立場を保持し, かつ, 適正な監査を実施してい るかを監視及び検証するとともに,
本案における複数の放送対象地域における放送番組の
変更前変更後備考 (2) 浸水防護重点化範囲の境界における浸水対策 【検討方針】
