気胸を合併した肺 Mycobacterium marinum 感染症の 1 例
1)関西電力病院呼吸器内科,2)淀川キリスト教病院呼吸器内科,
3)独立行政法人国立病院機構近畿中央胸部疾患センター臨床研究センター感染症研究部,
4)聖隷横浜病院呼吸器内科
玉置健一郎
1)鍋谷大二郎
2)吉田志緒美
3)青山 眞弓
4)澤田 宗生
1)草田 詩恵
1)竹嶋 好
1)久保 嘉朗
1)(平成 23 年 10 月 28 日受付)
(平成 24 年 1 月 11 日受理)
Key words : Mycobacterium marinum, pneumonia, pneumothorax
序 文
従来,Mycobacterium Marinumのヒトへの感染は,
魚や飼育熱帯魚との直接接触や菌に汚染した水と四肢 の擦過傷が接触することにより発症するとされてお り,四肢体幹の皮膚に結節や潰瘍を形成し swimming pool granuloma や fish tank granuloma 等と言われて いる.治療薬はクラリスロマイシン,リファンピシン,
エサンブトールなどの併用が言われておりデブリード マンが必要な深部皮膚病変には 2 剤以上の併用が望ま しいとされている1).M. marinumによる肺感染症は 極めて稀であり,同菌による肺感染症に合併した気胸 は今までに報告されていない.我々は気胸を合併した 肺M. marinum感染症の貴重な 1 例を経験したので報 告する.
症 例 症例:81 歳,男性.
主訴:呼吸困難.
既往歴:38 歳時に内痔核手術,72 歳時に変形性膝 関節症手術,78 歳時より前立腺肥大,過活動性膀胱 に対し内服加療されていた.
アレルギー歴:鯖で蕁麻疹.
家族歴:特記事項なし.
職歴:旅行会社の添乗員(20 年前に退職).
生活歴:喫煙歴なし.粉塵暴露歴なし.魚類を含め たペットの飼育歴なし.
現病歴:2006 年 6 月,半年間で約 10kg の体重減少 を主訴に近医受診された.胸部レントゲン上,異常陰 影を指摘され computed tomography(以下 CT)など
の精査を施行されたが,原因不明と言われた.また,
上部下部消化管内視鏡検査では異常を認めなかった.
2008 年 8 月に胸部異常陰影の為に A 病院へ入院精査 となった.胸部レントゲン画像では両側中肺野に網状 陰影を認め,胸部 CT 画像では中葉舌区を中心に気管 支拡張像と多数の小結節性陰影や分岐状陰影の散布像 を認めた(Fig. 1A).また 2 回以上の喀痰塗沫培養検
査よりM. marinumによる肺非結核性抗酸菌(NTM)
症と診断された.当時,呼吸器症状や血液検査上での 炎症所見は認めず,エリスロマイシンと去痰剤の投薬 で外来加療されていた.2008 年 11 月下旬頃より,喀 痰,咳嗽を認め,更に発熱,呼吸時に増強する胸痛が 出現し,12 月 1 日に当院救急外来受診された.低酸 素血症,両側肺炎,右気胸を認め,右胸腔内に chest tube を挿入し入院となった.
入 院 時 現 症:身 長 169.0cm,体 重 42.9kg,体 温 38.3℃,血圧 163!99mmHg,脈拍 90!分,整,呼吸回 数 24 回!分,SpO2:88%(room air).眼:両 側 眼 球 結膜に黄疸を認めず,両側眼球結膜に貧血を認めず,
心音:整,肺音:右肺呼吸音の低下を認め,左肺には 湿性ラ音を聴取する,腹部:平坦,軟,肝脾腫を認め ず,四肢:浮腫を認めず,皮膚:皮疹を認めず,ばち 指なし.神経学的異常所見なし.
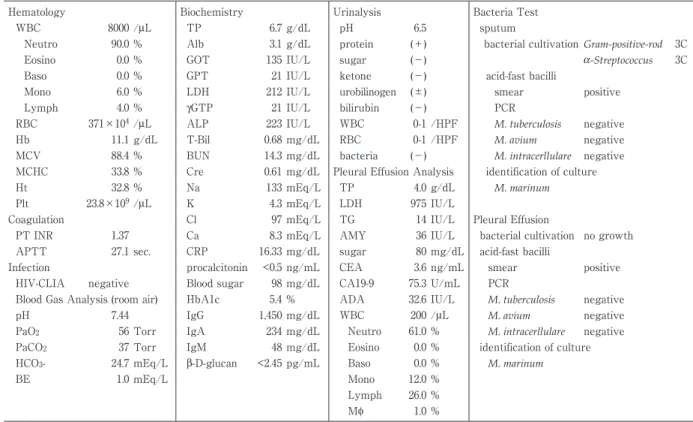
血液検査所見(Table 1):白血球の左方移動と軽度 の貧血,CRP 高値を認め,血液ガスでは room air で PaO2 56Torr の低酸素血症を認めた.また HIV 抗体 スクリーニングは陰性であった.
画像所見(Fig. 1B):上段は入院時の胸部レントゲ ンで,右気胸に対し chest tube を挿入しているが肺 の膨張は不充分である.左中肺野には網状影を認める.
下段の胸部 CT では右下葉には air bronchogram を 症 例
別刷請求先:(〒553―0003)大阪府大阪市福島区福島 2 丁目 1―7
関西電力病院呼吸器内科 玉置健一郎
Fig. 1 A) Chest radiography (top) taken on admission to the previous hospital. Reticu- lar shadows are observed in both, left dominant and middle lung field. In the chest CT (bottom) bronchial dilation is apparent in the lingular segment of the middle lobe and granular shadows are evident in the left inferior lobe. B) Chest radiography (top) taken on admission to our hospital shows the chest tube inserted into the right pneu- mothorax, but there is insufficient inflation of the lung. Reticular shadows are ob- served in the left middle lung field. Chest CT (bottom) shows consolidation with an air bronchogram in the right inferior lobe. Accumulation of right pleural effusion is also observed. B) Chest radiography (top) shows obvious improvement of the reticular shadows in both lungs. CT (bottom) shows obvious improvement of the consolidation with the air bronchogram, and improvement of the thickened bronchial walls and granular shadows.
伴う consolidation を認める.中葉舌区には気管支拡 張像を認め,左下葉には小粒状影を認める.また右胸 水の貯留を認める.
喀痰検査(Table 1):喀痰検査では細胞診は陰性で あった.肉眼的所見は P3,顕微鏡的所見は Geckler group 5 と良好な喀痰であったが一般細菌培養検査は Gram-positive-rod 3 コロニー及 びα-Streptococcus 3 コ ロニーのみであった.抗酸菌塗沫検査(チールネルゼ ン,蛍光染色)で 3+および 2+の陽性であったが,po- lymerase chain reaction(以下 PCR)検査ではM. tu- berculosis,M. avium,M. intracerllulareすべてに 陰 性 であった.MGIT 培養,2% 小川培養ともに陽性とな り,2% 小川培地を用いた 25℃,30℃,35℃ 培養で はすべての検体から光発色性,遅発育性のコロニーが 分離されたが,42℃ で発育は認められなかった.さ らに従来のM. marinumによくみられるスムース型の コロニーではなく,ラフ型のコロニーが過剰に発育し た.非結核性抗酸菌の同定キットである DDH マイコ バクテリアではM. marinumと同定され,INNO-LiPA MYCOBACTERIA(Innogenetics,ベ ル ギ ー)で は
M. marinum!M. ulceranseと 同 定 さ れ た.16S rDNA の前半部分は抗酸菌の菌種同定には有用であるが,M.
marinumとM. ulceranse,M. shinshuenseを 区 別 す る ことはできない.このため,本菌の 16S rDNA の全 長を対象として解析した結果,M. marinumと同定さ れた.また,rpoB遺伝子(348bp)の塩基配列型解析 においてもM. marinumと同定された.
胸水検査所見(Table 1):総蛋白 4.0g!dL,LDH 975 IU!L と Light の 基 準2)よ り 滲 出 性 胸 水 で あ っ た.
CEA,CA19-9 の有意な上昇を認めず,白血球は好中 球 優 位 で adenosine deaminase(以 下 ADA)は 32.6 IU!L であった.細胞診は陰性,一般細菌培養では菌 の発育を認めず,抗酸菌検査では喀痰と同様に塗沫・
培養検査共に陽性,PCR でM. tuberculosis,M. avium,
M. intracellulare陰性であった.分離された菌は 16S rDNA 全 長 塩 基 配 列 型 でM. marinum標 準 菌 株 と 100% の一致を示し,rpoB遺伝子の 2 カ所で各々 1 塩 基の違いが認められたにすぎなかったことからM.
marinumと判定された.胸水は糖が 40mg 以上で被包 化されておらず膿性でないことと Light の Parapneu-
Table 1 Laboratory data on admission and bacteria test of sputum and pleural effusion
Hematology Biochemistry Urinalysis Bacteria Test
WBC 8000 /μL TP 6.7 g/dL pH 6.5 sputum
Neutro 90.0 % Alb 3.1 g/dL protein (+) bacterial cultivationGram-positive-rod 3C
Eosino 0.0 % GOT 135 IU/L sugar (−) α-Streptococcus 3C
Baso 0.0 % GPT 21 IU/L ketone (−) acid-fast bacilli
Mono 6.0 % LDH 212 IU/L urobilinogen (±) smear positive
Lymph 4.0 % γGTP 21 IU/L bilirubin (−) PCR
RBC 371×104/μL ALP 223 IU/L WBC 0-1 /HPF M. tuberculosis negative
Hb 11.1 g/dL T-Bil 0.68 mg/dL RBC 0-1 /HPF M. avium negative
MCV 88.4 % BUN 14.3 mg/dL bacteria (−) M. intracerllulare negative
MCHC 33.8 % Cre 0.61 mg/dL Pleural Effusion Analysis identification of culture
Ht 32.8 % Na 133 mEq/L TP 4.0 g/dL M. marinum
Plt 23.8×109/μL K 4.3 mEq/L LDH 975 IU/L
Coagulation Cl 97 mEq/L TG 14 IU/L Pleural Effusion
PT INR 1.37 Ca 8.3 mEq/L AMY 36 IU/L bacterial cultivation no growth
APTT 27.1 sec. CRP 16.33 mg/dL sugar 80 mg/dL acid-fast bacilli
Infection procalcitonin <0.5 ng/mL CEA 3.6 ng/mL smear positive
HIV-CLIA negative Blood sugar 98 mg/dL CA19-9 75.3 U/mL PCR
Blood Gas Analysis (room air) HbA1c 5.4 % ADA 32.6 IU/L M. tuberculosis negative
pH 7.44 IgG 1,450 mg/dL WBC 200 /μL M. avium negative
PaO2 56 Torr IgA 234 mg/dL Neutro 61.0 % M. intracerllulare negative
PaCO2 37 Torr IgM 48 mg/dL Eosino 0.0 % identification of culture
HCO3- 24.7 mEq/L β-D-glucan <2.45 pg/mL Baso 0.0 % M. marinum
BE 1.0 mEq/L Mono 12.0 %
Lymph 26.0 %
Mϕ 1.0 %
monic effusion と Empyema の基準3)より膿胸ではな く simple complicated parapneumonic effusion と考 えた.以上よりM. marinumによる肺感染症,気胸,
肺炎随伴胸水と診断した.
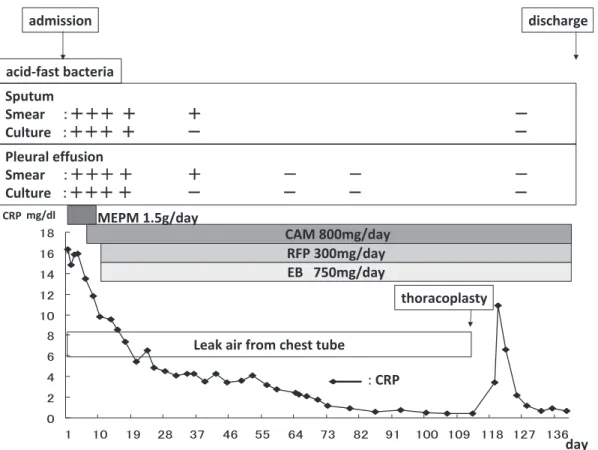
入院後経過(Fig. 2):入院直後はエンピリックに メロペネム 1.5g!day を投与していたが,M. marinum による肺感染症と診断した後はクラリスロマイシン 800mg!day,リファンピシン 300mg!day,エサンブ トール 750mg!day による加療 と し た.徐 々 に CRP の低下を認め,喀痰・胸水からの抗酸菌塗沫,培養も 陰性化した.しかし,chest tube からはエアーリー クが治まらず,肺の膨張は不完全であり,クランプテ ストを行うと肺の虚脱と明らかな喀痰量の増加を認め たため,当院呼吸器外科に依頼し胸郭形成術および肺 縫縮術を施行した.エアーリークは治まり chest tube を抜去可能となり術後の CRP 上昇も改善し退院と なった.画像上,胸部レントゲンでは両肺の網状陰影 は 明 ら か に 改 善 が 見 ら れ,CT に お い て も air- bronchgram を伴う consolidation は明らかに改善し,
気管支壁の肥厚,小粒状陰影も改善を認めた(Fig. 1 C).その後,少なくとも半年間,再燃は認めていな い.
考 察
従来ヒトへのM. marinum感染は,魚や飼育熱帯魚 との直接接触や菌に汚染した水と四肢の擦過傷が接触
することにより発症するとされ,四肢体幹の皮膚に結 節や潰瘍を形成する.肺への感染の報告はニシキヘビ やマナティーでの報告4)5)がある一方でヒトに対しての 報告も調べた限りでは 2 例6)7)のみと非常にまれであ る.また,報告のうち 1 例は後天性免疫不全症候群の 44 歳男性へのM. marinum全身感染症と考えられた もので,もう 1 例はM. marinumによる肺結節を認め た 56 歳の健常人女性の報告であった.本例は良好な 喀痰が得られたが一般細菌培養では有意菌を認めず,
一般細菌による肺炎は否定的と考えられた.胸部 CT 画像において中葉舌区を中心に気管支拡張像と多数の 小結節性陰影や分岐状陰影の散布像を認め,2 回以上 の異なった喀痰検体でのM. marinum培養陽性を認 め,「肺非結核性抗酸菌症診断に関する指針 2008」8)よ
りM. marinumによる肺感染症と考えられた.感染経
路に関しては swimming pool や魚類接触歴はなく体 表に皮疹を認めず,しかも複数の喀痰検体や胸水から
M. marinumが分離されたことから,環境からの迷入
やヒトへの一時的な定着が起こっているとは考えにく い.HIV 感染症や糖尿病などの易感染性につながる 病態は認めなかったが,気管支拡張が既存にあり局所 免疫の低下によりM. marinumによる肺感染症を発症 した可能性が考えられた.またM. marinumの培養の 最適温度は 30℃ 前後であるが,Lai らによると肺感 染症を引き起こしたM. marinumは 35℃ 培養で陽性
Fig. 2 The process changing from positive (+) to negative (−) findings of acid-fast bacteria in the sputum, the pleural effusion and clinical course.
という7).本症例の菌株は 35℃ の条件で最も発育が旺 盛となり,通常より高い温度でも培養されうるM.
marinumがやや温度の低い体表面の皮膚感染症でな
く,温度の高い体内の肺感染症を起こしたと思われる.
肺結核に気胸が合併することは知られており頻度も 1.5% との報告がある9).一方,非結核性抗酸菌症(以 下 NTM 症)に関しての胸膜関連合併症は胸水などを 含め少ないと考えられていた10)が,荻原らは気胸合併 率が 2.3% と推定しており11),結核に比べ少なくない 可能性もある.病巣が胸膜直下にある場合は初期の NTM 症でも胸膜穿破により気胸をきたすことがある とされる12)が,荻原らの検討では NTM 症の病変が一 側肺野面積を超える範囲のものが多く,NTM 症の病 状進行の末に広範囲に肺が荒廃しているものが多かっ たとしている11).本例は広範囲の気管支拡張像,小結 節陰影と,気胸並びに胸水を認めたが,M. marinum が検出された胸水は膿胸を満たすものではなく肺炎随 伴性もしくは胸膜炎に伴うものと考えられた.本例に
M. marinumが感染した時期は不明であるが,胸部異
常陰影を指摘された少なくとも 2 年以上前からの可能 性が高く,肺病変は大部分がM. marinumによるもの と考えられた.気胸に関しては,組織学的には証明で きていないが,胸水からM. marinumが検出されたこ とを考えると胸膜直下の抗酸菌性病変が胸膜を穿破し
たものと考えられた.
治療薬はクラリスロマイシン,リファンピシン,エ サンブトールなどの併用が言われておりデブリードマ ンが必要な深部皮膚病変には 2 剤以上の併用が望まし いとされている1).これに習い本症例はクラリスロマ イシン 800mg!day,リファンピシン 300mg!day,エ サンブトール 750mg!day による加療とし,改善を認 めた.NTM 症は肺結核に比べ比較的短期間に軽快す ることが少ないため,合併する気胸は予後不良であり,
外科的治療を含めた集学的治療が必要といわれる11). 本例は薬物療法が他の NTM 症と比べ比較的短期間に 軽快したこと,外科的治療が可能であったことなどが 回復の要因であったと考える.
我々が調べた限りM. marinumによる気胸を伴った 肺感染症の報告は未だかつて無く報告した.
最後に本症例に関し多大なる助言をいただきました,広 島県健康保険協会健康クリニックの斎藤肇先生に深謝申し 上げます.
文 献
1)Lewis FM, Marsh BJ, von Reyn CF:Fish tank exposure and cutaneous infections due toMyco- bacterium marinum: tuberculin skin testing, treatment, and prevention. Clin Infect Dis 2003;37:390―7.
2)Light RW:Clinical practice. Pleural effusion.
The New England journal of medicine 2002;
346:1971―7.
3)Light RW:A new classification of parapneu- monic effusions and empyema. Chest 1995;
108:299―301.
4)Hernandez-Divers SJ, Shearer D:Pulmonary mycobacteriosis caused by Mycobacterium hae- mophilum and M. marinum in a royal python.
Journal of the American Veterinary Medical Association 2002;220:1661―3, 50.
5)Sato T, Shibuya H, Ohba S, Nojiri T, Shirai W:
Mycobacteriosis in two captive Florida mana- tees(Trichechus manatus latirostris). J Zoo Wildl Med 2003;34:184―8.
6)Kishihara Y, Nakashima K, Nukina H, Hayashi J, Kashiwagi S:Two cases of acquired immu- nodeficiency syndrome with disseminated non- tuberculous mycobacterial infection. Kansen- shogaku zasshi 1993;67:1223―37.
7)Lai CC, Lee LN, Chang YL, Lee YC, Ding LW, Hsueh PR:Pulmonary infection due to Myco- bacterium marinum in an immunocompetent pa-
tient. Clin Infect Dis 2005;40:206―8.
8)日本結核病学会非結核性抗酸菌症対策委員会:
肺非結核性抗酸菌症診断に関する指針―2008 年.
結核 2008;83:525―6.
9)Aktogu S, Yorgancioglu A, Cirak K, Kose T, Dereli SM:Clinical spectrum of pulmonary and pleural tuberculosis : a report of 5,480 cases. Eur Respir J 1996;9:2031―5.
10)福元重太郎,猪島一郎,藤田昌樹,桑野和善,中 西洋一:気胸・胸膜炎を合併し た 肺Mycobacte- rium intracellulare症 の 1 例.結 核 2005;80:
571―5.
11)荻原恵理,椎原 淳,榎本崇宏,土屋典子,馬
場智尚,篠原 岳,他:気胸を合併した非結核 性抗酸菌症 16 例の臨 床 的 検 討.日 呼 吸 会 誌 2010;48:104―7.
12)水谷尚雄,萱野公一:肺末梢孤立性のMycobacte- rium avium intracellulare complex 感染巣による 続発性自然気胸の一例.日呼外会誌 2008;22:
943―7.
A Case of Lung Infection Complicated by Pneumothorax Caused byMycobacterium marinum
Kenichiro TAMAKI1), Daijiro NABEYA2), Shiomi YOSHIDA3), Mayumi AOYAMA1), Muneo SAWADA1), Utae SOUTA1), Miyoshi TAKESHIMA1)& Yoshiro KUBO1)
1)Department of Respiratory Tract Medicine, Kansai Electric Power Hospital,
2)Department of Respiratory Tract Medicine, Yodogawa Chiristian Hospital,
3)Department of National Hospital Organization Kinki-chuo Chest Medical Center,
4)Department of Respiratory Tract Medicine, Seirei Yokohama Hospital
Mycobacterium marinum is a waterborne mycobacterium that commonly infects fish and amphibians worldwide, but transmission to humans can occasionally occur, typically as a granulomatous skin infection following minor hand trauma. Infection involving the lungs is very rare. We herein describe a case of M.
marinum-associated pneumonia and pneumothorax.
In August 2008, an 81-year-old man was admitted to a hospital for detailed examination of weight loss and an abnormal shadow on chest imaging. Based on a sputum test, nontuberculous mycobacteriosis caused byM. marinumwas diagnosed. At that time, the blood chemistry revealed no respiratory symptoms or in- flammatory findings, and the patient was treated on an outpatient basis with erythromycin and an expecto- rant. In late November 2008, sputum and coughing were observed. Furthermore, the patient developed a fe- ver and chest pain that increased while breathing and he visited the emergency outpatient unit of our hos- pital on December 1. Hypoxemia, bilateral pneumonia, and right pneumothorax were observed, and a chest tube was inserted into the right thoracic cavity. Results of an acid-fast bacteria smear from the sputum and pleural effusion were positive, andM. marinumwas identified on culture. The patient was diagnosed as hav- ing a lung infection complicated by pneumothorax caused by M. marinum. The lung infection was amelio- rated with clarithromycin, rifampicin and ethambutol. However, no decreased in the air leaking from the chest tube was noted and inflation of the lung was incomplete. The department of respiratory surgery therefore performed thoracoplasty and lung cerclage. Subsequently, the air leak subsided, allowing removal of the chest tube and the patient was discharged.
〔J.J.A. Inf. D. 86:139〜143, 2012〕