原発性脳リンパ腫を合併したトキソプラズマ脳炎の再発例
1)がん・感染症センター都立駒込病院感染症科,2)同 感染制御科,3)千葉大学大学院医学研究院感染生体防御学,
4)東京都保健医療公社豊島病院
鷲野 巧弥
1)矢嶋敬史郎
1)福島 一彰
1)関谷 紀貴
2)野呂瀬一美
3)味澤 篤
1)4)今村 顕史
1)(平成 29 年 12 月 20 日受付)
(平成 30 年 6 月 5 日受理)
Key words : toxoplasmic encephalitis, primary central nervous system lymphoma(PCNSL),AIDS
序 文
トキソプラズマ脳炎(toxoplasmic encephalitis;
TE)は,AIDS(acquired immune deficiency syn- drome)患者における頭蓋内結節性病変の原因の中で
最も多くを占める
1). CDC(Centers for Disease Con- trol and Prevention)の診断クライテリア2)では,意 識障害や局所の神経所見と画像所見が
TEに合致し,
かつ血清抗トキソプラズマ抗体陽性か診断的治療に反 応する場合に
TEと診断するとされている.TE が疑 われる症例では,原発性脳リンパ腫(primary central
nervous system lymphoma;PCNSL)との鑑別を要するが,画像所見と血清抗体による確定診断は難しく,
診断的治療を行うことも多い.TE と
PCNSLの合併 は剖検例の報告に限られ,検索しえた範囲では生前に 診断された報告はない.今回我々は,適切なタイミン グで脳生検を行うことで両者の合併と診断し救命しえ た症例を経験したので報告する.
症 例
症例:63 歳,男性.
主訴:痙攣発作.
既往歴:なし.
生活歴:喫煙歴なし,飲酒歴なし.
現病歴:5 年前に左基底核,左頭頂葉,右後頭葉の
TE発症を契機に
HIV感染症と診断された.ピリメ タミン(初日に
200mg/日,2日目以降に
75mg/日),スルファジアジン(4,000mg/日)による半年間の初 期治療と抗
HIV療法により軽快したが,維持治療中 の
2年前に通院を自己中断した.今回,左上下肢の強 直間代性痙攣が出現し当院に救急搬送された.
入院時現症:意識清明,体温
36.3℃,血圧123/82 mmHg,脈拍74回/分,呼吸数
16回/分,SpO
2 100%(室内気).身体所見では,口蓋弓に白苔を認めるほか に特記すべき所見なし.神経学的所見は,左上下肢で 徒手筋力テスト
4点程度の不全片麻痺を認めた.
血液検査所見:LDH と
sIL-2R(soluble interleukin- 2 receptor)価の上昇を認めた.抗トキソプラズマIgG抗体は陽性で,CD4 陽性リンパ球数
2/μL,HIV-RNA 2.0×104copies/mLであった(Table 1).
画 像 検 査 所 見:頭 部 造 影
MRIの
T1強 調 像(T1-
weighted image;T1WI)で右頭頂葉に周囲に強い浮腫を伴った非典型的な増強効果をもつ
2.7cm大の結 節を認め,タリウムシンチグラフィーで同部位に取り 込みを認めた(Fig. 1).
髄液検査所見:細胞数の上昇なし.
Epstein-Barr vi-rus(EBV)PCR
が陽性であったが,細胞診で悪性細
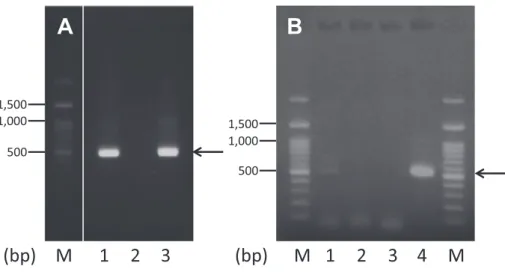
胞を認めなかった.トキソプラズマ
B1遺伝子を標的 とした
nested PCR法
3)でトキソプラズマ特異的遺伝 子が検出された(Fig. 2A).
入院後経過:髄液トキソプラズマ
PCR検査が陽性 で
MRI所見も
TEに合致することから
TEの再発と 考えられた.前回治療中に汎血球減少によりスルファ ジアジンをクリンダマイシンに変更した期間があった ため,初期治療はピリメタミン(初日に
200mg/日,2日目以降に
50mg/日)とクリンダマイシン(2,400mg/日)を選択した.2 週間の診断的治療を行ったが病変 は縮小しなかった.髄液
EBV-PCR検査が陽性でタリ ウムシンチグラフィーでも取り込みがみられたことか
ら
PCNSLの合併を考慮し,入院
3週目に開頭生検術
を施行した.病理組織学的所見では,結節辺縁部から 採取した検体は
CD20陽性の腫瘍細胞を認め,びまん 性大細胞型
B細胞リンパ腫(diffuse large B-cell lym-
症 例別刷請求先:(〒113―8677)東京都文京区本駒込 3―18―22 がん・感染症センター都立駒込病院感染症科
矢嶋敬史郎
Fig. 1 A: Contrast-enhanced brain MRI T1WI shows a 2.7-cm nodule with the eccentric target sign and surrounding edema in the right parietal lobe. B: Thallium-201 scintigra- phy uptake in the nodule (early ratio: 2.2 delay ratio: 1.9 retention index: 0.85)
Table 1 Laboratory data on admission
Hematology Biochemistry Infection/Immunology
WBC 4,700 /μL TP 6.5 g/dL HIV-RNA 2.0×104copies/mL
Neu 75.7 % UN 7 mg/dL CD4 2 cells/μL
Lym 16.2 % Cre 0.63 mg/dL sIL-2R 693 U/mL
Mono 4.5 % Na 139 mEq/L Toxoplasma IgG >240 IU/mL
Eos 3.4 % K 3 mEq/L Cryptococcus Ag (−)
Baso 0.2 % T-bil 0.5 mg/dL HBs-Ag (−)
RBC 313×104/μL AST 58 U/L HCV-Ab (−)
Hb 10.6 /μL ALT 74 U/L RPR (−)
Ht 30.2 % LDH 281 U/L TPLA (−)
Plt 15.2×104/μL CRP 0.05 mg/dL
Abbreviations: RPR, Rapid plasma regain; TPLA, Treponema pallidum latex agglutination; HIV, human immunodeficiency virus; sIL-2R, soluble interleukin-2 receptor; IgG, immunoglobulin G
phoma;DLBCL)に矛盾しなかったが,中心部から
採取した検体はリンパ球や組織球に富み,腫大した
as-trocyte
もみられ,リンパ腫のみでは説明のつかない
病変であった(Fig. 3).脳生検組織を用いて前述の
nested PCR
法を行ったところ,辺縁部の組織からは
トキソプラズマ特異的遺伝子の増幅が認められなかっ たが,中心部の組織からは僅かながら増幅が認められ た(Fig. 2B).以上より
PCNSLを合併した
TEの再 発と診断した.経過中に薬疹が出現したため,クリン ダマイシンをアトバコン(3,000mg/日)に変更し,3 カ月間の初期治療の後に維持治療へ移行した.また,
テノホビル/エムトリシタビン,ラルテグラビルで抗
HIV療法を再開し,PCNSL に対して全脳照射(30Gy/
15fr)および局所照射(10Gy/5fr)とステロイド投与
(ベタメタゾン
8mg/日より漸減)を行った.後遺症を残さず軽快し,その後約
1年が経過したが再発は認
められていない.
考 察
TE
と
PCNSLは
AIDS患者における頭蓋内結節性 病変の中で最も多く,いずれも
CD4陽性リンパ球数 が
50未満で発症することの多い日和見疾患である.両 者の合併は稀ではあるが,TE 治療中に異なる部位の 頭蓋内病変が増大し,剖検で
PCNSLと判明した症例
4)や,TE の治療に反応せず剖検で
TEと
PCNSLの合
併と判明した症例
5)が報告されている.いずれも死亡
後に剖検で両者の合併と診断された報告に限られ,本
症例のように生前に両者の合併と診断され治療に成功
した症例の報告は初めてである.TE は確定診断が難
しいため,診断的治療を要することも多く,診断のつ
かない合併例が潜在している可能性がある.その一因
としては,トキソプラズマ
PCR検査方法が確立され
ていないことが考えられる.
Fig. 2 Detection of Toxoplasma gondii B1 gene with the nested polymerase chain reaction technique.
(A) Cerebrospinal fluid sample (lane M, size marker; lane 1, cerebrospinal fluid; lane 2, negative control; lane 3, positive control; arrow, 531 bp)
(B) Brain biopsy samples (lane M, size marker; lane 1, central brain tissue; lane 2, peripheral brain tissue; lane 3, negative control; lane 4, positive control; arrow, 531 bp)
1 2 3 M
A
500 1,500 1,000
1 2 3
M 4 M
B
500 1,500 1,000
(bp) (bp)
Fig. 3 Histopathological findings of the brain biopsy demonstrate diffuse large B-cell lym- phoma cells in the margin of the nodule (A. Hematoxylin & eosin, ×40; B. CD20, ×40), but none in the center of the nodule (C. Hematoxylin & eosin, ×40; D. Masson-Noguchi staining, ×20).
臨 床 症 状 や 画 像 所 見 か ら
TEが 疑 わ れ る も の の
PCNSL
との鑑別のための脳生検を考慮すべき症例と
して,血清抗トキソプラズマ
IgG抗体陰性例や髄液
EBV-PCR陽性例が報告されている
6)7).髄液
EBV-PCRは
PCNSLに特異度が 高 く
7),陽 性 で あ れ ば
PCNSLが示唆される.本症例は
TEの既往があり血清抗トキ ソプラズマ抗体は今回の
TE再発の診断根拠となら
ず,髄液
EBV-PCRも陽性であったため,脳生検を考
慮すべき症例と考えられた.一方,タリウムシンチグ ラフィーで取り込みがある場合も
PCNSLが示唆され るが,uptake ratio や
retention indexの低い症例で は
PCNSLでない可能性があると報告されており
8)9), 本症例では
TEに対する診断的治療を優先した.2 週 間の経過で改善すれば
TEと診断できるが,PCNSL であれば診断の遅れが予後に影響するため
6)10),診断 的治療に反応しないと分かった時点ですみやかに脳生 検を行う必要がある.合併例においても適切なタイミ ングでの脳生検が有用である.
TE
の診断における髄液トキソプラズマ
PCR検査 は,感度にばらつきがあるものの特異度はほぼ
100%と報告されており
11)12),陽性であれば診断的価値が高 い.しかし,治療開始後
1週間で感度が下がると報告 されており
12)13),治療開始前の検体採取が望ましい.ま た,HE 染色で病理学的にトキソプラズマやその嚢子 が確認できない場合にも,組織検体のトキソプラズマ
PCR検査により診断できた例も報告されている
14).今 回,脳生検組織の
nested PCR検査を行い,中心部か ら検出されたが,辺縁部からは検出されなかった.こ のことから,この脳生検組織の中心部にはトキソプラ ズマ
DNAが存在していたことが明らかになり確定診 断に結びついた.診断に困る場合には脳生検組織を用 いた
PCR検査も有用と考えられる.
PCNSL
を合併した
TEの再発例を経験した.適切
なタイミングで脳生検を行い,生検組織検体のトキソ プラズマ
PCR検査も併用することで診断・治療でき た.稀ではあるが
TEと
PCNSLが合併することがあ り,合併例においても適切な脳生検とトキソプラズマ
PCR検査が有用であると考えられた.
謝辞:PCR 検査に際して多大なるご協力を頂きま した千葉大学大学院医学研究院感染生体防御学の彦坂 健児先生に深謝いたします.
利益相反自己申告:申告すべきものなし
文 献1)厚生労働省エイズ動向委員会:平成27(2015)年 エイズ発生動向年報.
2)Kaplan JE, Benson C, Holmes KK, Brooks JT, Pau A, Masur H:Guidelines for prevention and treatment of opportunistic infections in HIV- infected adults and adolescents recommenda- tions. MMWR Recomm Rep 2009;58:1―207.
3)Grigg ME, Boothroyd JC:Rapid identification of virulent type I strains of the protozoan pathogen Toxoplasma gondii by PCR-restriction
fragment length polymorphism analysis at the B1gene. J Clin Microbiol 2001;39:398―400.
4)Laviopierre AM, Lawler GA:Cerebral toxopla- smosis and lymphoma in patients with acquired immunodeficiency syndrome. Australas Radiol 1989;33:270―5.
5)Stenzel W, Pels H, Staib P, Impekoven P, Bek- tas N, Deckert M:Concomitant manifestation of primary CNS lymphoma and Toxoplasma en- cephalitis in a patient with AIDS. J Neurol 2004;251:764―6.
6)Utsuki S, Oka H, Abe K, Osawa S, Yamazaki T, Yasui Y,etal.:Primary central nervous system lymphoma in acquired immune deficiency syn- drome mimicking toxoplasmosis. Brain Tumor Pathol 2011;28:83―7.
7)Antinori A, Ammassari A, De Luca A, Cingolani A, Murri R, Scoppettuolo G,etal.:Diagnosis of AIDS-related focal brain lesions : a decision- making analysis based on clinical and neuroradi- ologic characteristics combined with polym- erase chain reaction assays in CSF. Neurology 1997;48:687―94.
8)Miller RF, Hall-Craggs MA, Costa DC, Brink NS, Scaravilli F, Lucas SB,etal.:Magnetic resonance imaging, thallium-201 SPET scanning, and laboratory analyses for discrimination of cerebral lymphoma and toxoplasmosis in AIDS.
Sex Transm Infect 1998;74:258―64.
9)Lorberboym M, Wallach F, Estok L, Mosesson RE, Sacher M, Kim CK,etal.:Thallium-201 re- tention in focal intracranial lesions for differen- tial diagnosis of primary lymphoma and nonma- lignant lesions in AIDS patients. J Nucl Med 1998;39:1366―9.
10)Terriff BA, Harrison P, Holden JK:Apparent spontaneous regression of AIDS-related pri- mary CNS lymphoma mimicking resolving toxoplasmosis. J Acquir Immune Defic Syndr 1992;5:953―4.
11)Alfonso Y, Fraga J, Fonseca C, Jiménez N, Pinil- los T, Dorta-Contreras AJ,etal.:Molecular di- agnosis ofToxoplasma gondiiinfection in cerebro- spinal fluid from AIDS patients. Cerebrospinal Fluid Res 2009;6:2.
12)Cingolani A, De Luca A, Ammassari A, Murri R, Linzalone A, Grillo R,etal.:PCR detection of Toxoplasma gondii DNA in CSF for the differen- tial diagnosis of AIDS-related focal brain lesions.
J Med Microbiol 1996;45:472―6.
13)Anselmo LM, Vilar FC, Lima JE, Yamamoto AY, Bollela VR, Takayanagui OM:Usefulness and limitations of polymerase chain reaction in the etiologic diagnosis of neurotoxoplasmosis in immunocompromised patients. J Neurol Sci 2014;346:231―4.
14)Kruse AY, Kvich L, Eickhardt S, Omland LH,
Bjarnsholt T, Moser C:Unexpected diagnosis of cerebral toxoplasmosis by 16S and D2 large-
subunit ribosomal DNA PCR and sequencing. J Clin Microbiol 2015;53:1983―5.
A Recurrent Case of Toxoplasmic Encephalitis Accompanied by Primary Central Nervous System Lymphoma
Takuya WASHINO1), Keishiro YAJIMA1), Kazuaki FUKUSHIMA1), Noritaka SEKIYA2), Kazumi NOROSE3), Atsushi AJISAWA1)4)& Akifumi IMAMURA1)
1)Department of Infectious Diseases and2)Department of Infection Prevention and Control,
Tokyo Metropolitan Komagome Hospital,3)Department of Infection and Host Defense, Graduate School of Medicine, Chiba University,4)Toshima Hospital, Tokyo Metropolitan Health and Medical Treatment Corporation In patients with human immunodeficiency virus (HIV) infection, toxoplasmic encephalitis (TE) is a com- mon cause of space-occupying brain lesions, but primary central nervous system lymphoma (PCNSL) can likewise present as a focal brain lesion and has a poor prognosis. Therefore, distinguishing TE from PCNSL is important, but usually difficult. We herein on report a rare case for TE complicated with PCNSL in a pa- tient with HIV infection. He was referred to our hospital with tonic-clonic seizures. He had been treated for TE and HIV infection for 5 years, but he stopped going to the hospital 2 years previously. His CD4-positive cell count was 2/μL and the serum anti-Toxoplasma IgG antibody was positive. Cranial magnetic resonance imaging (MRI) showed a 2.7-cm nodule with the eccentric target sign and surrounding edema in the right parietal lobe. Thallium-201 scintigraphy showed an uptake in the nodule. Both Epstein-Barr virus and Toxoplasma gondiiDNAs were detected in the cerebrospinal fluid with the polymerase chain reaction (PCR) technique. Because empiric treatment for TE failed to improve his symptoms, a brain biopsy was performed and showed PCNSL on histopathologic examination andToxoplasma DNA on PCR. After whole-brain radia- tion therapy, dexamethasone, and antiretroviral therapy, his symptoms and MRI abnormalities improved. A brain biopsy andToxoplasmaPCR test should be considered in cases with atypical clinical presentation.
〔J.J.A. Inf. D. 92:696〜700, 2018〕