は じ め に
内頚動脈(internal carotid artery:ICA)paraclinoid 動脈 瘤に対する主たる治療法には開頭クリッピング術と血管内 治療(interventional radiology:IVR)があるが,治療結果 や合併症率に関しては差がないとする報告が多い3).未破 裂 paraclinoid 瘤に対する開頭群(691 例)と IVR 群(1,013 例)のメタアナリシスによれば,正常視力が悪化する率は 開頭群 10.8%で IVR 2.0%と IVR に分がある一方,低下し ている視力が改善する率は開頭群のほうが良好である2). クリッピング・コイル塞栓・フローダイバーター(FD)3 聖マリアンナ医科大学 脳神経外科(受稿日 2018. 6. 3)(脱稿日 2018. 9. 10)〔連絡先:〒 216-8511 神奈川県川崎市宮前区菅生 2-16-1 聖 マリアンナ医科大学 脳神経外科 田中雄一郎〕[Address correspondence: Yuichiro TANAKA, M.D., Ph.D., Department of Neurosurgery, St. Marianna University School of Medicine, 2-16-1 Sugao, Miyamae-ku, Kawasaki, Kanagawa 216-8511, Japan]
脳卒中の外科 48: 1 〜 6,2020
特集 内頚動脈瘤クリッピング術
者のメタアナリシスでは,治療後の視機能に有意差はな かったものの FD 群で良好との傾向がある一方,術後の視 機能悪化に 3 者間の差はない8).今後,この部位の瘤の治 療には FD の適用が増加すると予測されるが1),現時点で はクリッピング術を要する機会も少なからず存在する. IVR 時代においては,クリッピング術の合併症を減らし 視機能を改善させるさらなる努力が求められる.本稿で は,10〜20 mm の大型瘤 3 症例を提示して,クリッピン グ術の技術的側面とピットフォールを論じる.大型 ICA paraclinoid 動脈瘤のクリッピング術とピットフォール
田中雄一郎,大塩恒太郎,伊藤 英道,佐瀬 泰玄
池田 哲也,川口公悠樹,梶 友紘,久代裕一郎
Clipping Surgery for Large ICA Paraclinoid Aneurysms and Pitfalls
Yuichiro TANAKA, M.D., Ph.D., Kotaro OOSHIO, M.D., Ph.D., Hidemichi ITO, M.D., Ph.D., Taigen SASE, M.D., Ph.D., Tetsuya IKEDA, M.D., Kimiyuki KAWAGUCHI, M.D.,
Tomohiro KAJI, M.D., Ph.D., and Yuichiro KUSHIRO, M.D.
Department of Neurosurgery, St. Marianna University School of Medicine, Kawasaki, Kanagawa, Japan
Summary: For many years, neck clipping of large internal carotid artery paraclinoid aneurysms has been challenging. However, recent technical developments in coil embolization and flow diverters have been associated with great advancements. Indeed, reducing surgical complications related to neck clipping in the era of interventional radiology is essential. The basic techniques include 1) prepa-ration of the cervical carotid artery, 2) cannulation of the carotid artery, 3) craniotomy, 4) sectioning of the falciform ligament, 5) removal of the anterior clinoid process, 6) preparation of the ophthalmic artery, 7) temporary arterial occlusion, and 8) intraoperative angiography or indocyanine green video-angiography. Key points of the surgical techniques include appropriate preparation of the parent ar-tery and selection of the aneurysm clips. Here, some technical details, including the removal of the anterior clinoid process, the separation of the distal dural ring and the transposition of the sphenopa-rietal sinus, are described to both avoid surgical complications and improve the visual outcome.
Key words:
・ anterior clinoid process ・ clipping
・ paraclinoid aneurysm Surg Cereb Stroke (Jpn) 48: 1-6, 2020
手 術 方 法 1.装備・機材
開頭クリッピング術で必要な装備や機材には,somato-sensory evoked potential(SEP)/motor evoked potential (MEP)/visual evoked potential(VEP)モニタリング,術中 血管撮影(digital subtruction angiography:DSA),indocy-anine green(ICG)ビデオ血管撮影などがある. 2.手術の基本的手順 ①頚部頚動脈の露出:大型瘤では必須で,内頚動脈内膜 剝離術の半分ほどの皮切で施行,②カテーテル留置:suc-tion-decompression を要する例では外頚動脈ないし総頚動 脈に挿入,③前頭側頭開頭,④ falciform process 切離と anterior clinoid process(ACP)削除,⑤硬膜輪切離と眼動 脈確保,⑥母動脈一時閉塞下に瘤周囲の剝離と瘤頚部確 保,⑦クリッピング,⑧術中血管撮影ないし ICG,⑨閉創. 3.手術の適応 paraclinoid 動脈瘤とは,瘤頚部が遠位硬膜輪から後交 通動脈分岐部までの硬膜内の ICA 瘤と定義した.いわゆ る C3 瘤は海綿静脈洞内の瘤も含むが,内向き瘤の多くは carotid cave 内に発生するので,くも膜下腔の瘤に分類さ れる.遠位硬膜輪は,側面から透視すると長軸が前方に傾 斜した楕円でその内側アーチが近位に偏り,carotid cave はその後下方に位置する.この部の術前評価には非サブト ラクション血管撮影と MRI の constructive interference in steady state(CISS)画像(脳槽像)が有用である.carotid cave 内に留まる小型瘤と判断された場合は,クリッピン グ術の対象とはしなかった6)10).その時点で施設の IVR 技 術力に照らして施術が比較的困難とされた瘤にクリッピン グ術を適用した.筆頭筆者が術者としてクリッピングを施 行した連続 60 名 63 個の paraclinoid 瘤(うち 10 mm 以上は 14 個)の治療成績と合併症に関しては,すでに本誌で報告 した12).以下,ピットフォールに遭遇した 3 例を提示する. 症 例 〈症例 1〉 左眼視力の低下を主訴とした 65 歳女性.視力は 1.2/0.5 で,右同名半盲と左動眼神経不全麻痺を認めた.左 ICA 眼動脈分岐部に 15 mm の瘤を認めた(Fig. 1).20 分間の バルーン閉塞試験は無症状であった.シルビウス裂を開く と,瘤に押し上げられた左視神経を認め,falciform pro-cess 切開で除圧した.視神経上面には硬膜縁の圧痕が観 察された.ACP と視神経管上に翻転した 1 cm の硬膜弁を 糸で吊り,ポケット状の窪みの底で ACP を削除した.硬 膜輪を約半周切離して眼動脈起始部を確保した.頚部頚動 脈,瘤遠位 ICA および眼動脈の一時閉塞で瘤内圧は十分 下がり,suction decompression は必要とせずクリッピン グは可能であった.しかし,初めに用いた弯曲ブレードの クリップは術中 DSA で ICA 狭窄を生じており,斜め屈曲 ブレードのクリップと L 型右弯曲有窓クリップの 2 本に 置き換える必要があった(Fig. 2).術後視力は 0.8 に改善 し視野も広がり,動眼神経麻痺も数週間で完全寛解した. 〈症例 2〉 41 歳女性の破裂動脈瘤例(grade 5).右 ICA の眼動脈分 岐部より遠位の上向き瘤(10 mm)で,解離性ではなく囊状 Fig. 1 Three-dimensional computed tomography (CT) angiography in Case 1 showing a
paraclinoid aneurysm (15 mm) of the left internal carotid artery (A). A magnetic resonance imaging illustrating the upward displacement of the left optic nerve dis-placed by the aneurysm (B).
Left optic nerve
CISS image
Fig. 2 Intraoperative (A, B) and postoperative (C) angiograms in Case 1. A stenosis of the carotid
sy-phon and the incomplete closure of the clip blades (arrows) are shown (A). The curved clip (1) is replaced by an obliquely-angled clip (2) and a curved L-shaped clip (3) (B, C).
1 2 3 2 3 A B C
Fig. 3 Computed tomography (CT) angiography before (A) and after operation (B) in Case 2. A B
Fig. 4 Intraoperative findings of the right frontotemporal craniotomy and extradural removal of
the anterior clinoid process (ACP, 1) in Case 2. Removal of the lateral part of the superior orbital fissure consisting in the periosteal dura (2) (A). Separation between the cranial nerves (3) and the meningeal dura to expose the tip of the anterior clinoid process (4) (B). Drilling of the fully-exposed ACP (C).
1 2 2 3 4 1 4 A B C
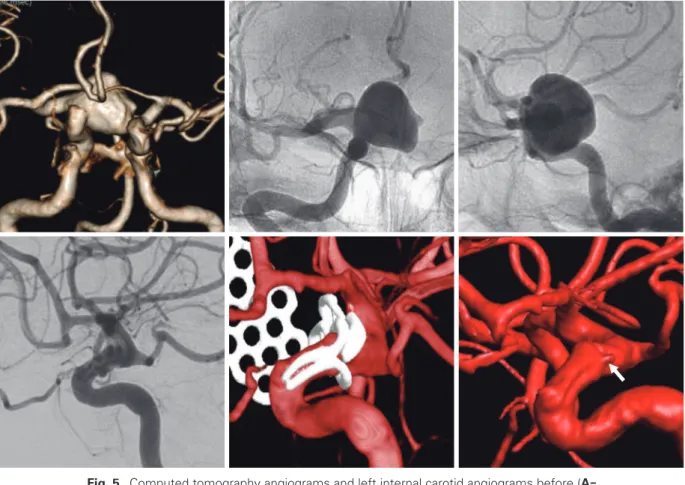
Fig. 5 Computed tomography angiograms and left internal carotid angiograms before (A -C) and after the operation (D-F) in Case 3, showing the successful occlusion of a
large paraclinoid aneurysm with two aneurysm clips. Computed tomography angio-grams before (E) and after the subtraction of the metallic materials (F) showing a tiny residue (arrow) at the triangular cleft between the clips.
A B C D E F
Fig. 6 Intraoperative findings of the right frontotemporal craniotomy in Case 3. Bridging veins of the
fron-tal and temporal lobes (1, 2) drain into the sphenopariefron-tal sinus (SPS). Elevation of the fronfron-tal lobe is restricted by the bridging veins (1). The internal carotid artery is partially shown (3) (A). The dura is divided along the sylvian fissure after the extradual removal of the anterior clinoid process (B). The venous complex is shifted posteriorly and the aneurysm (4) is exposed (C).
1 2 3 1 1 2 3 4 A B C
動脈瘤と判断した(Fig. 3).硬膜外から上眼窩裂外側の骨 膜を切離して露出した ACP を切除した(Fig. 4).硬膜輪 を切離して ICA に可動性をもたせ,瘤頚部近位の母動脈 周囲にテンポラリークリップを挿入する十分なスペースを 確保してから瘤周囲を剝離した.右視神経の外側と動脈瘤 頚部の外側のくも膜の癒着が強く,不完全な剝離のままク リップをかけると小破裂があった.ブレードの位置を母動 脈側にずらして対処でき,最終的にスリップアウト予防の ため 2 本のクリップを平行にかけた(Fig. 3).術後 3 カ月 で高次脳機能障害は改善し,復職できた. 〈症例 3〉 右視力低下(0.4)で発症した 20 歳女性.右 ICA ophthal-mic segment に 20 mm の内向きの瘤を認めた(Fig. 5).前 頭葉は 3 本のシルビウス静脈の 1 本で蝶形頭頂静脈洞 (sphenoparietal sinus:SPS)に固定され,挙上不能と判明 した(Fig. 6).硬膜外で ACP を削除し,SPS 前縁の硬膜 を切離して脳を移動させると瘤を露出できた.総頚動脈, 外頚動脈,ICA 遠位,眼動脈の 10 分間遮断と suction de-compression 下に,L 型右弯曲有窓クリップと弯曲のミニ クリップの 2 本で瘤を閉塞した.術後の CTA で,有窓ク リップのブレード基部の合わせ目とミニクリップのブレー ド先端の隙間に造影剤の侵入があったが,瘤は血栓化して いた(Fig. 5).術後視力に変化はなかった. 考 察 ICA paraclinoid 動脈瘤が他の頭蓋内動脈瘤と最も異な るのは,硬膜内操作のみでは安全確実な母動脈確保ができ ないことである.バルーンカテーテルを頚部頚動脈に留置 する方法もあるが,ヘパリン化による術野の血液漏出が問 題になることもあり,現時点では頚部切開が無難であ る.症例 1 のように眼動脈も含めたトラッピングを行え ば,suction decompression が不要な例も多い.しかし, 術中破裂の際の一時血流遮断のために頚部頚動脈の確保は 欠かせない. 大型瘤では頭蓋内での母動脈確保のために ACP 削除が 必要なことが多い.硬膜外法と硬膜内法があり,その選択 に関しては長く議論されてきた7).両方法の利点と欠点を よく吟味して症例ごとに決めるべきであるが,術者がより どちらの方法に馴染んでいるかで選択されることが多いよ うである.われわれは好んで,小型の硬膜弁を用いたハイ ブリッド法を用いている11).ただし,症例 2 のような上向 きの破裂瘤の場合は,硬膜内で前頭葉を挙上すると破裂す る可能性が高いので,硬膜外から ACP を削除している. 症例 3 のように,シルビウス裂開放不能例で SPS 移動の 操作を連続して行えることも硬膜外法の利点である4). 大型瘤のクリッピングでは,複数のクリップが必要にな ることが多いが,特に内向き瘤においては初めの 1 本と最 後の 1 本が重要である.遠位硬膜輪の切開が不十分な場 合,症例 1 のように ICA の狭窄を生じやすい.瘤頚部近 位が遠位硬膜輪に近いほど硬膜輪切離の距離を長くする必 要がある.carotid cave 瘤と同様に全周性切離が必要なこ ともある.2 番目ないし最後に瘤頚部遠位にかけるクリッ プは,窓のないタイプが推奨される.理由としては,後交 通動脈や前脈絡叢動脈を誤ってブレードで挟むのを防ぐた めと,窓部が折れてブレードに移行する部位の隙間でつか み残しが生じる恐れがあるためである.内向き瘤には有窓 クリップを用いることが多いが,非有窓クリップで対応で きることもある.シンプルな形状のクリップをシンプルな 組み合わせで用いるのが multiple clipping の基本である. 頚部が幅広の瘤では,クリッピングで再建された母動脈 が直線化しやすい9).これは,closed cell の頭蓋内ステン ト使用時と同様に注意を払うべき現象である.症例 1 の 3 番目のクリップのように,L 型有窓クリップにはブレード が左ないし右に側弯しているタイプがあるので,ICA 直 線化軽減のため右 ICA 瘤には右弯曲を,左 ICA 瘤には左 弯曲を用いる.また,長いブレードのクリップ 1 本のみで 対処せず,複数の短いブレードのクリップを組み合わせる ことも推奨される.症例 2 のような隣接するクリップの隙 間に漏出経路ができないよう,2 本のクリップのブレード を重複させるのがよい. 最大の合併症である視機能悪化は,あらゆる知識と精緻 な手技を総動員して極力避けなければならない12).視機能 障害は,視神経周囲のドリリング,視神経の剝離操作,眼 動脈や上下垂体動脈の血流障害,クリップによる圧迫,異 物に対する炎症などにより発生し得る.実際は複数の要因 が重複している可能性があり,必ずしも特定の原因に絞り づらいのが実状であろう.動脈瘤壁に癒着した視神経の剝 離は最小限の面積に留めるのが無難である.クリッピング 後に視神経がたわむ場合にのみ,必要な剝離を追加してい る.瘤壁に癒着した上下垂体動脈も剝離しづらいことがあ る.概して癒着した動脈は,大型瘤ではストレッチされ血 流が乏しく閉塞しても無症状のことが多いが,遮断は念の ため VEP モニター下に行うべきである.VEP は万能では ないが,paraclinoid 瘤の手術に備えて,普段から安定し たモニタリングをできる環境を整えておく必要がある5). 術前視力低下例においてはクリッピング術が IVR の優位 に立ち得ることを意識して,視機能改善を目指す手術に努 めるべきである. 結 論 paraclinoid 瘤クリッピング術のキーポイントは,母動脈
の確保と適切なクリップ選択である.一時血流遮断で瘤の 圧を下げて剝離やクリッピング操作を行えば,他部位の瘤 の手術に比べ格別リスクが上積みされるわけではない.た だし,ACP 削除や硬膜輪切離に習熟を要する.術前視機 能低下例では,その改善を目指したクリッピング術を行う ことで IVR に対する優位性を発揮し得る. 本論文は,2018 年 3 月に福岡で開催された第 47 回日本 脳卒中の外科学会学術集会における教育講演の内容を一部 改めて記載した. 著者全員は日本脳神経外科学会への COI 自己申告を完 了しています.本論文の発表に関して開示すべき COI は ありません. 文 献
1) Adeeb N, Griessenauer CJ, Foreman PM, et al: Comparison of stent-assisted coil embolization and Pipeline embolization de-vice for endovascular treatment of ophthalmic segment an-eurysms: a multicenter cohort study. World Neurosurg 105: 206-212, 2017
2) Asaid M, O’Neill AH, Bervini D, et al: Unruptured paraclinoid aneurysm treatment effects on visual function: systematic review and meta-analysis. World Neurosurg 106: 322-330, 2017
3) Bae DH, Kim JM, Won YD, et al: Clinical outcome of paracli-noid internal carotid artery aneurysms after microsurgical neck clipping in comparison with endovascular embolization.
J Cerebrovasc Endovasc Neurosurg 16: 225-234, 2014 4) Day JD, Giannotta SL, Fukushima T: Extradural
temporopo-lar approach to lesions of the upper basitemporopo-lar artery and infra-chiasmatic region. J Neurosurg 81: 230-235, 1994
5) Goto T, Tanaka Y, Kodama K, et al: Loss of visual evoked potential following temporary occlusion of the superior hy-pophyseal artery during aneurysm clip placement surgery. J
Neurosurg 107: 865-867, 2007
6) Kobayashi S, Kyoshima K, Gibo H, et al: Carotid cave aneu-rysms of the internal carotid artery. J Neurosurg 70: 216-221, 1989
7) 中川 忠,小澤常徳,森 宏,ほか:傍前床突起内頚動脈 瘤の手術手技─硬膜内および硬膜外前床突起削除法の選択に ついて.脳卒中の外科 46: 97-103, 2018
8) Silva MA, See AP, Dasenbrock HH, et al: Vision outcomes in patients with paraclinoid aneurysms treated with clipping, coiling, or flow diversion: a systematic review and meta-analysis. Neurosurg Focus 42: E15, 2017
9) Tanaka Y, Kobayashi S, Kyoshima K: Multiple clipping tech-nique for large and giant internal carotid artery aneurysms and complications: angiographic analysis. J Neurosurg 80: 635-642, 1994
10) Tanaka Y, Hongo K, Tada T, et al: Radiometric analysis of paraclinoid carotid artery aneurysms. J Neurosurg 96: 649-653, 2002
11) Tanaka Y, Hongo K, Tada T, et al: Protective dural flap for bone drilling at the paraclinoid region and porus acusticus.
Neurol Med Chir(Tokyo)43: 416-418, 2003
12) 田中雄一郎,大塩恒太郎,伊藤英道,ほか:Paraclinoid 動脈 瘤頚部クリッピング術における合併症の分析.脳卒中の外科 45: 165-170, 2017