Introduction
A study group of the Ministry of Health, Labour and Welfare (MHLW) has just announced the newest 2013 version of the Guidelines for the Treatment of Chronic Hepatitis B1). In essence, the Guidelines specify drugs and treatment period by categorizing patients into those aged 35 years or older and those younger than 35 years. Recommended treatment regimens are classified into several types based on presence or absence of the hepatitis B e antigen (eAg) or hepatitis B DNA (HBV-DNA), and the alanine transaminase (ALT) level prior to treatment.
According to the Guidelines, therapeutic agents are selected from 2 types, pegylated interferon
(peginterferon) alfa-2a and entecavir, which is a nucleoside analog (NA) preparation. The use of the former drug is limited to 48 weeks, while no limitation is specified for the latter drug.
The purpose of treatment of chronic hepatitis B is inhibition of disease progression and prevention of cancer. Specifically, treatment is intended to achieve seroconversion of eAg so that hepatitis B surface antigen (HBsAg) would eventually turn negative through the antiviral and immunostimulatory actions of peginterferon alfa-2a in the long term2). In the short term, treatment aims to obtain negative serostatus of HBV-DNA through the potent inhibitory effect of entecavir on the replication
Clinical significance of serial quantitative measurement of hepatitis B surface antigen in patients with chronic hepatitis B who were treated with nucleoside analogs
Kazuyoshi Ishikawa1), Tohru Nitatori1), Chihoko Nakakarumai2), Naoko Isobe3)
Abstract
Hepatitis B surface antigen (HBsAg) was measured serially in 18 patients with chronic hepatitis B (13 males, 5 females; median age, 60 years; median observation period, 55 months) treated with nucleoside analogs (NAs). In 8 patients for whom comparison before and after the treatment was possible, correlation was noted among HBsAg, hepatitis B DNA (HBV-DNA) and hepatitis B core-related antigen (HBcrAg) levels before the treatment. HBV-DNA was distributed over 5.7 to 7.3 LGE/mL or 5.8 to > 8.8 log copies/
mL at the start of the treatment with NAs and was markedly decreased in all patients to 2.1> log copies/
mL at the time of the last observation. However, HBsAg was decreased only in 3 patients, unchanged in 4 patients and increased in 1 patient. In the patient whose HBsAg was increased, HBcrAg was not lowered enough and hepatocellular carcinoma (HCC) was detected 85 months after the treatment with NA. HBsAg in 5 patients remained at above 1,000 IU/mL. Patients whose HBsAg is not lowered enough should be considered to be at risk for carcinogenesis regardless of serum HBV-DNA level. Overall, treatment with NAs clearly lowered the serum HBV-DNA level in patients with chronic hepatitis B, but did not reduce the HBsAg level sufficiently. In order to improve a clinical condition of chronic hepatitis B and prevent cancer, treatment should be aimed at lowering the HBsAg level, and the combined use of NAs and peginterferon alfa-2a or sequential therapy should be considered. Serial measurement of HBsAg during treatment with NAs is thus considered to be useful for monitoring the therapeutic efficacy of NAs.
Key word:hepatitis B surface antigen, hepatitis B e antigen and antibody, HBV-DNA, hepatitis B virus core-related antigen , nucleoside analog
受付日:平成 25 年 10 月 8 日 受理日:平成 25 年 12 月 24 日
1)Faculty of nursing, Iwate Prefectural University
2)Future Wind Seiwa Hospital
3)Niigata University of Health and Welfare
of HBV-DNA3-5). The Guidelines were developed to adjust the treatment according to the clinical background of each patient, thereby obtaining the therapeutic effect more efficiently.
In actual treatment, it often takes 1 to 2 years to evaluate the therapeutic effect of peginterferon alfa-2a. In contrast, entecavir produces its effect quickly. In many patients, serum HBV-DNA becomes negative after a few months of treatment. However, a small number of patients develop resistance to treatment with entecavir. Issues related to entecavir for future research include resistance to treatment as well as the timing of stopping treatment.
According to the Guidelines, candidates for treatment with entecavir are patients with a high viral load, those with abnormal ALT and those of advanced age for whom histological progression is expected. Overseas guidelines are composed of largely the same criteria6-8). The Guidelines issued by the MHLW Study Group specify that patients with HBV-DNA of ≧4 log copies/mL and ALT of ≧31 IU/L undergo treatment with entecavir, regardless of the presence or absence of eAg. In actual clinical practice, a large proportion of patients are 35 years of age or older and eAg negative, which means that entecavir is the first-line therapy for most patients.
The ultimate goal of treatment for chronic hepatitis B is to achieve remission and prevent cancer through achieving seronegativity of HBsAg, which means elimination of the virus.
In the short term, treatment aims to normalize ALT, convert eAg to seronegative or achieve seroconversion to e antibody (eAb) and obtain negative HBV-DNA serostatus. Currently, no clear conclusion has been reached concerning the evaluating of the therapeutic effect of the above-mentioned drugs with respect to long- term prognosis and the necessity of using combination therapy with these drugs.
In the present study, we serially and quantitatively measured HBsAg in patients with chronic hepatitis B treated with NAs after the start of treatment, and examined the significance of treatment with NAs for the long-
term prognosis of the disease.
Materials and methods Subjects
This study included 18 patients with chronic hepatitis B who were treated with various nucleoside analogs(NA). In each patient, HBsAg was measured after starting treatment with serial observation at least once a year and, ALT, HBV-DNA levels, eAg /eAb, hepatitis B virus core-related antigen(HBcrAg)and HBV genotype also were evaluated.
Quantification of HBsAg
HBsAg was quantified using a ARCHTECT・HBsAg QT kit(Abbot Japan Co. Ltd., Chiba, Japan). The result was were expressed as IU/ml. The value of more than 0.05 IU/ml was considered positive.
Quantification of HBV-DNA
Serum HBV-DNA was quantified using a TMA kit (Chugai Diagnostic Science Co.
Ltd., Tokyo, Japan) , at a first. The result was were expressed as log genome equivalent (LGE) / ml. The value of less than 3.7 LGE/
mL was considered as an undetectable level.
Subsequently HBV DNA was quantified using a COBAS AmpliPrep-COBAS TaqMan HBV test (Roche, Branchburg, NJ, USA). The result was expressed as a log copy number / ml.
The value of less than 2.1 log copy/ml was considered as an undetectable level.
Determination of serum eAg and eAb
Serum eAg and eAb were determined by enzyme-linked immunosorbent assay. The result of eAg was expressed as cut off index.
The value more than 2.0 was considered positive. The result of eAb was expressed as
%inhibition. The value more than 50% was considered positive.
Quanrtification of HBcrAg
Serum HBcrAg was quantified using a Lumipulse kit(Fujirebio Inc., Tokyo, Japan).
The result was expressed as a log unit / ml. The value more than 3.0 was considered positive.
HBV genotyping
HBV genotyping were performed using Imunis kit (Institute of Immunology Co. Ltd.,
Tokyo, Japan).
Determination of amino acid substitution the reverse transcriptase domain of polymerase gene Determination of amino acid substitution in the rt domain of polymerase gene which is resistant to lamivudine was performed using Inno-LiPA HBV DR Version2 Plus kit (Medical and Biological Laboratories Co Ltd., Ina, Japan ).
Statistical analysis
Statistical analysis was performed using SPSS 20.0J for Windows (SPSS Inc., IL, USA).
Student's t-test and Pearson’s correlation coefficient were employed to determine significant differences, and p values of less than 5% were considered significant.
Ethical considerations
The present study conformed to the guidelines of epidemiological studies devised by the Ministry of Health, Labor and Welfare, Japan, to prevent leakage of personal information, and were conducted to for the purpose of social profit.
Results
Background of the study patients
This study comprised a total of 18 patients (13 males, 5 females; mean age, 57.3 years; median
age, 60 years; mean observation period, 59.8 months; median observation period, 55 months).
The background of the patients is summarized in Table 1. Three patients were eAg positive, 2 were negative for both eAg and eAb, and 13 were eAb positive. The genotype was B in 10 patients and C in 8 patients. Treatment was started with lamivudine in 7 patients and was continued in 2. Three of those 7 patients had viral breakthrough due to emergence of a resistant strain, and adefovir was added. In the remaining 2 patients, lamivudine was switched to entecavir. Treatment was started with entecavir in 11 patients and was continued in all 11. At the completion of observation, HBV- DNA was negative in 13 patients and signal positive in 5, indicating a clear decrease. ALT was stable in all patients. The clinical course was favorable in all patients except 1 with genotype C, who was receiving continuous treatment with lamivudine and developed hepatocellular carcinoma (HCC).
Correlation of HBsAg with HBV-DNA, HBcrAg and ALT before treatment
The relationships among HBsAg, HBV-DNA and ALT in 8 patients for whom comparison was possible before the treatment with NAs
Table 1.Patients with hepatitis B who were treated with nucleoside analogs
are presented in Figures 1 through 4. A significant positive correlation between HBsAg and HBV-DNA was observed when HBV-DNA was expressed in units of logarithmic genome equivalents (LGE)/mL, and a tendency toward positive correlation was noted when HBV-DNA was expressed in log copies/mL. A similar tendency toward positive correlation was observed between HBV-DNA and HBcrAg. No correlation was found between HBV-DNA and ALT.
Comparison of backgrounds before treatment according to genotype
The background of the 8 patients for whom
comparison was possible before initiation of treatment with NAs was examined by genotype (Table 2). Five patients had genotype B and 3 patients had genotype C. No difference
Figure 1. Correlation between HBsAg
concentration and HBV-DNA(LEG/mL)
before the nucleoside analog treatment
Figure 2. Correlation between HBsAg concentration and HBV-DNA(Log copy/
mL) before the nucleoside analog treatment
Figure 3. Correlation between HBsAg concentration and HBcrAg before the nucleoside analog treatment
Figure 4. Correlation between HBsAg concentration and ALT before the nucleoside analog treatment
Table 2.Age and labolatory data at the
start of the nucleoside analog treatment
according to a genotype
was observed in age and HBsAg between the genotypes, while HBcrAg was significantly higher in patients with genotype C. ALT showed a tendency toward increase in patients with genotype C.
Comparison of various markers in patients between initiation of treatment and endpoint of observation Changes in HBV-DNA, HBsAg and HBcrAg in 8 patients for whom comparison was possible between these variables at the start of treatment with NAs and at the time of the last observation are presented in Table 3.
Treatment with lamivudine was continued in 2 patients, adefovir was added to lamivudine due to emergence of a resistant strain in 1 patient, and treatment with entecavir was continued in 5 patients. HBV-DNA was high in all patients (5.7 to 7.3 LGE/mL or 5.8 to > 8.8 log copies/
mL) at the start of treatment and >2.1 log copies/mL in all patients at the time of the last observation, indicating a marked decrease.
However, HBsAg showed a clear decrease only in 3 patients, was largely unchanged in 4 patients, and was clearly increased in 1 patient, who developed HCC. HBsAg remained above 1,000 IU/mL in 5 patients, and >2,000 IU/mL in 3 of the 5 patients. Seven out of 8 patients were HBcrAg positive at the start of treatment, and HBcrAg became negative only in 2 patients at the time of the last observation. The other 5 patients continued to be HBcrAg positive, although the amount of antigen decreased.
The patient whose HBsAg increased and who developed HCC continued to be HBcrAg positive. The onset of cancer was 85 months
after the start of treatment with lamivudine.
Subsequent changes in HBsAg concentration after the start of nucleoside analog treatment
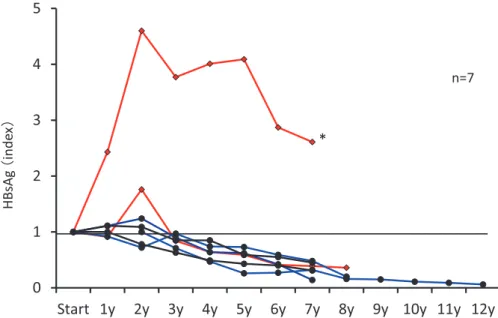
The changes in HBsAg over time in the 7 patients who started the treatment with lamivudine are shown in Figure 5. The mean duration of observation was 93.4 months (median, 88 months). The rates of increase or decrease in HBsAg at the start of treatment are presented. In one of the patients who continued to be treated with lamivudine only, HBsAg started to increase 1 year after the start of the treatment and was 4.6 times the starting level after 2 years. Then, HBsAg gradually decreased, but the patient developed HCC 7 years after the start, when HBsAg was 2.6 times the level at the start of treatment. In the other patient, who was continuously treated with lamivudine only, HBsAg increased to 1.8 times the level at the start of the treatment after 2 years, became decreased thereafter, and was below the level at the start and further decreased gradually from 3 to 8 years after the start. In all 3 patients who received the addition of adefovir and the 2 patients for whom lamivudine was switched to entecavir, HBsAg was below the level at the start of the treatment and gradually decreased from 3 years after the start.
The changes in HBsAg over time in the 11 patients who started the treatment with entecavir are shown in Figure 6. The mean duration of the observation period was 38.5 months (median, 36 months). As with the patients who started the treatment with lamivudine, the rates of increase or decrease from HBsAg at
Table 3.Status of HBV-DNA, HBsAg and HBcrAg concentration at the start and endpoint
of observation in patients treated with various nucleoside analogs
Figure 5.Subsequent changes of HBsAg concentration in patients in whom the nucleoside analog treatment was started with lamivudine. A value of HBsAg at the start of treatment is defined to be 1. Red lines present patients in whom lamivudine was continued, blue lines present those in whom adefovir was added because of viral breakthough, and black lines present those in whom lamivudine was switched to entecavir. *Asterisk indicates the patient who developed HCC.
Figure 6.Subsequent changes of HBsAg concentration in patients in whom the nucleoside analog treatment was started with entecavir. A value of HBsAg at the start of treatment is defined to be 1. Red lines present patients who were positive for HBeAg and black lines present patients who were positive for HBeAb at the start of treatment respectively.
*Asterisk indicates the patient who lost HBeAg.
0 1 2 3 4
Start 1y 2y 3y 4y 5y 6y
HBsAg(index)
Figure 6.Subsequent changes of HBsAg concentration in patients in whom the nucleoside analog treatment was started with entecavir. A value of HBsAg at the start of treatment is defined to be 1. Red lines present patients who were positive for HBeAg and black lines present patients who were positive for HBeAb at the start of treatment respectively. *Asterisk indicates the patient who lost HBeAg.
n=11
*
the start of the treatment are presented. In one of the 3 eAg positive patients, HBsAg increased after the start of the treatment, reached 3.4 times the starting level 2 years later, and was still 3.0 times the starting level at 3 years after the start. In the other 2 eAg positive patients, HBsAg gradually decreased to below the level at the start of the treatment, at 1 year after the start. In some of the 8 eAb positive patients, HBsAg was higher than the level at the start of the treatment even 3 years after the start and thereafter.
Discussion
The therapeutic methods for chronic hepatitis B that have been improved through various transitions have just been summarized in the newest Guidelines from the MHLW. The short-term therapeutic goals are prevention of cancer and inhibition of fibrosis by the strong inhibitory action of NAs on the replication of HBV-DNA9,10). In the present study, HBV-DNA decreased down to the undetectable level or less at the time of the last observation in all 18 study patients. The clinical course was stable in all patients except 1 who developed HCC. In that patient, HBsAg clearly increased from the level at the start of treatment, and HBcrAg also continued to be positive.
Moreover, in 5 (including the above patient who developed HCC) out of the 8 patients for whom comparison of variables before and after the treatment was possible, HBsAg clearly did not decrease and remained >1,000 IU/mL at the time of the last observation. Patients with HBsAg levels of 1000 IU/mL or higher have been reported to be at high risk for cancer and therefore should be carefully observed for possible development of cancer in the future11,12). Before the start of the treatment with NAs, a positive correlation or a tendency toward correlation was observed between HBsAg and HBV-DNA. However, while HBV-DNA decreased rapidly after the start of treatment, HBsAg increased, remained unchanged or decreased, showing various patterns13).
In the patients for whom treatment was
started with lamivudine and adefovir was added due to emergence of a resistant strain, decrease in HBsAg was most rapid and prominent. All patients for whom treatment was started with entecavir remained on the same treatment.
Among them, 1 out of 3 eAg positive patients showed an increase in HBsAg. In contrast, in another eAg positive patient, HBsAg rapidly decreased after the start of treatment and eAg became negative; this suggests that the disappearance of eAg or a continued decrease in HBV-DNA can be expected if a clear decrease in HBsAg is observed after the start of treatment in eAg positive patients14,15). In the other patients, a clear tendency toward a decrease in HBsAg was not noted, probably due to the short observation period. Based on these results, when the long-term goal is to achieve negative HBsAg, some patients do not easily benefit from monotherapy with an NA, specifically entecavir. Therefore, concomitant use of peginterferon alfa-2a or sequential therapy in which an NA is switched to peginterferon alfa-2a should be considered in the future.
Nevertheless, no sufficient evidence exists at present for improvement in therapeutic efficacy by either of the above methods1,16).
A positive correlation was observed between HBsAg and HBcrAg before the start of treatment; after the start of treatment, HBcrAg did not become negative in patients whose HBsAg clearly did not decrease. HBcrAg is known to reflect the amount of covalently closed circular DNA (cccDNA), a replicative intermediate of intrahepatic HBV17) . The absence of a decrease in HBsAg is considered to indicate that the HBV replication in the liver has not been stopped, regardless of the serum HBV-DNA level. For this reason, it is necessary to recognize the risk for the development of liver cancer in patients without a decrease in HBsAg. In particular, patients with genotype C who have a significantly increased level of HBcrAg require close observation.
In the present study, treatment with NAs clearly decreased the serum HBV-DNA level in patients with chronic hepatitis B, but was not
sufficiently effective in reducing HBsAg. One of the patients treated with NAs developed cancer. Although many of the patients were eAb positive, HBsAg remained high after the treatmalest with NAs in half of these patients.
This suggests that seroconversion to eAb does not contribute to a reduction in cancer risk.
We therefore speculate that serial quantitative measurement of HBsAg in patients being treated with NAs is useful for monitoring the efficacy of this treatment. Moreover, we consider that such measurement should be used more frequently in the future for selecting which untreated chronic hepatitis B patients should receive treatments with NAs.
References
1)The Japan society of hepatology:Guidelines for the management of hepatitis B virus infection. Kanzo, 54, 402-472, 2013.
2)Marcellin P, Bonino F et al.:Sustained response of hepatitis B e antigen-negative patients 3 years after treatment with peginterferon alpha-2a. Gastroenterology, 136, 2169-2179, 2009.
3)Chang TT., Gish RG. et al.:A comparison of entecavir and lamivudine for HBeAg- positive chronic hepatitis B. N Engl J Med, 354, 1001-10, 2006.
4)Lai CL., Shouval D. et al.:Entecavir versus lamivudine for patients with HBeAg- negative chronic hepatitis B. N Engl J Med, 354, 1011-20, 2006.
5)Sherman M, Yurdaydin C. et al.:Entecavir for treatment of lamivudine-refractory, HBeAg-positive chronic hepatitis B.
Gastroenterology, 130, 2039-49, 2006.
6)European Association For The Study Of The Liver:EASL clinical practice guidelines:
Management of chronic hepatitis B virus infection. J Hepatol, 57, 167-185, 2012.
7)Liaw YF, Leung N et al.:Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int, 2, 263-283, 2008.
8)Lok AS, McMahon BJ:Chronic hepatitis B:
update 2009. Hepatology, 50, 661-662, 2009.
9)Chen CJ, Yang HI et al.:Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA, 295, 65-73, 2006.
10)Papatheodoridis GV, Manolakopoulos S et al.:Follow-up and indications for liver biopsy in HBeAg-negative chronic hepatitis B virus infection with persistently normal ALT: a systematic review. J Hepatol, 57, 196-202, 2012.
11)Tseng TC, Liu CJ et al.:High levels of hepatitis B surface antigen increase risk of hepatocellular carcinoma in patients with low HBV load. Gastroenterology, 142, 1140- 1149, 2012.
12)Tseng TC, Kao JH:Clinical utility of quantitative HBsAg in natural history and nucleos(t)ide analogue treatment of chronic hepatitis B: new trick of old dog. J Gastroenterol, 48, 13-21, 2013.
13)Fung J, Lai CL et al.:Quantitative hepatitis B surface antigen levels in patients with chronic hepatitis B after 2 years of entecavir treatment. Am J Gastroenterol, 106, 1766-1773, 2011.
14)Lee MH, Lee da M et al.:Correlation of serum hepatitis B surface antigen level with response to entecavir in naïve patients with chronic hepatitis B. J Med Virol, 83, 1178- 1186, 2011.
15)Kim SS, Lee D et al.:Association of on- treatment serum hepatitis B surface antigen evel with sustained virological response to nucleos(t)ide analog in patients with hepatitis B e-antigen positive chronic hepatitis B. Hepatol Res, 43,219―227, 2013.
16)Hosaka T, Suzuki F et al.:Clearance of hepatitis B surface antigen during long- term nucleot(s)ide analog treatment in chronic hepatitis B:results from a nine- year longitudinal study. J Gastroenterol, 48, 930-941, 2013.
17)Wong DK, Tanaka Y et al.:Hepatitis B virus core-related antigens as markers for monitoring chronic hepatitis B infection. J Clin Microbiol 45, 3942-3947, 2007.
和文要旨
Nucleoside analog(NA)投与を行った B 型慢性肝炎 18 例(男性 13 例、女性 5 例、観察期間中央値 55 ヵ月)を対象にした。治療前後の比較が可能であった 8 例では、治療前の HBsAg 量と HBV-DNA 量お よび HBcrAg 量には相関傾向がみとめられた。治療開始時に高値を示した HBV-DNA 量は、全例検出感度 以下に著減した。しかし、HBsAg 量が減少したのは 3 例のみで、他の 4 例は不変、1 例は増加した。
HBsAg 量増加の 1 例では HBcrAg 量の減少も不十分で、治療開始 85 ヵ月後に HCC の発生をみた。HBsAg 量非減少例では、発がんのリスクを認識しておく必要があると考えられた。全 18 例でみても、NA 治療は B 型慢性肝炎患者の血中 HBV-DNA 量を明らかに減少させたが、HBsAg 量の減少効果は不十分であった。
今後 B 型慢性肝炎の治療は HBsAg 量の減少を目指し、NA と peginterferon alpha-2a の併用あるいは sequential therapy も考慮されるべきと考えられる。NA 治療例における HBsAg 量の経時的測定は、NA 治療中の治療効果把握のモニタリングに有用であると考えられる。
キーワード:HBs 抗原、HBe 抗原・抗体、HBV-DNA、HB コア関連抗原、核酸アナログ製剤