は じ め に
近年の画像診断機器の発達により,膵漿液 性嚢胞腺腫(serous cystadenoma: SCA)はしば しば発見されるが,悪性はまれであることか ら経過観察されることが多い. 今回,我々は 画像上,多房性嚢胞が増大傾向を示し,嚢胞 内に壁在結節を疑う所見を認め,膵管内乳頭 粘液性腫瘍(intraductal papillary-mucinous neo-plasm: IPMN)との鑑別が困難であったため切 除し,SCAであった1例を報告する. 症例:58歳 女性 主訴:なし 既往歴:22歳: 虫垂炎(手術),40歳: 喘息, 57歳:卵巣莢膜細胞腫,Meigs症候群,胆石症 (手術) 現病歴: 当院産婦人科で右卵巣腫瘍(右卵巣 莢膜細胞腫)に対して単純子宮全摘術+両側 付属器摘出術(+胆嚢摘出術)を施行された. その際にCTで膵頭部の嚢胞性腫瘤(2.4 cm) を指摘され経過観察されていた.今回14ヶ月 後,経過観察目的のCTで嚢胞性腫瘤が2.4 cm から3.5 cmへ増大傾向を示したため,精査加 療目的で当科を紹介受診した. 入院時現症:身長149cm,体重94kg,BMI 40.1 kg/m2,腹部に圧痛なし,腫瘤触知なし,手術 瘢痕あり,上腹部正中切開(胆嚢摘出術),下 腹部正中切開(卵巣腫瘍術後),血液生化学所 見:T-Cho(315 mg/dl),TG(395 mg/dl)の上昇 あり,腫瘍マーカー(CEA,CA19-9)上昇なし, 腹部造影CT所見: 右卵巣莢膜細胞腫術前の CTにて偶然膵頭部に径2.4 cmの嚢胞性病変を [症 例 報 告]
画像上拡大傾向を示した膵漿液性嚢胞腺腫の1例
中本 充洋,皆川 紀剛,山口 幸二
産業医科大学 医学部 第1外科学教室
要 旨:膵漿液性嚢胞腺腫(serous cystadenoma: SCA)は,悪性はまれであり経過観察されるこ とが多い.今回我々は,嚢胞が増大傾向を示し,intraductal papillary-mucinous neoplasm(IPMN)との 鑑別が困難であったため切除し,SCAであった 1 例を経験したため報告する.症例は58歳,女性. Meigs症候群を伴う右卵巣莢膜細胞腫に対して摘出術を施行された際,CTで膵頭部の多房性嚢胞 性腫瘤を指摘され経過観察されていた.14ヶ月後のCTで嚢胞が2.4 cmから3.5 cmへ増大傾向を示 し,嚢胞内に壁在結節を疑う所見を認め,IPMNの可能性が否定できなかったため,幽門輪温存膵頭 十二指腸切除術を施行した.術後の病理診断ではSCAの診断であった.発見の時点ではMeigs症 候群による多量の腹水のため嚢胞が圧迫され,実際の嚢胞の大きさよりも小さく見えていた可能 性が考えられた. キーワード:膵漿液性嚢胞腺腫,IPMN,Meigs症候群. (2012年 2 月14日 受付, 2012年 4 月23日 受理)
類円形の核を入れる.
胞体にはperiodic acid-Schiff (PAS)陽性顆粒 を示し(Fig. 4C),また,それらはジアスターゼ で消化され,グリコーゲンを豊富に有してい
たことが分かる(Fig. 4D).MIB-1 indexは 1 % 未満であった(Fig. 4E).
以上より,SCAと診断した. 術後 1 年の時 点で再発は認めていない.
Fig. 3.
Findings of ultrasonography. A. Endoscopic ultrasound (EUS) show the cyst 5.3×3.0 cm, B. EUS showed mural nodules within the cyst, C. Main pancreatic duct (MPD) doesnʼt reveal stenosis or dilatation. Cyst press MPD. Cyst isnʼt communicated with MPD.Fig. 4.
Surgical and laboratory findings. A. Section shows the cyst, 4 cm in diameter in pancreatic head, B. The cyst was lined with a single layer of simple cuboidal epithelium, C. D. Periodic acid-Schiff staining, with and without diastase digestion, showed abundant glycogen within cytoplasm of epithelial cells, yielding a definitive diagnosis of SCA, E. MIB-1 index is less than 1%.A
A
B
C
C
D
E
B
A
A
B
C
C
D
E
B
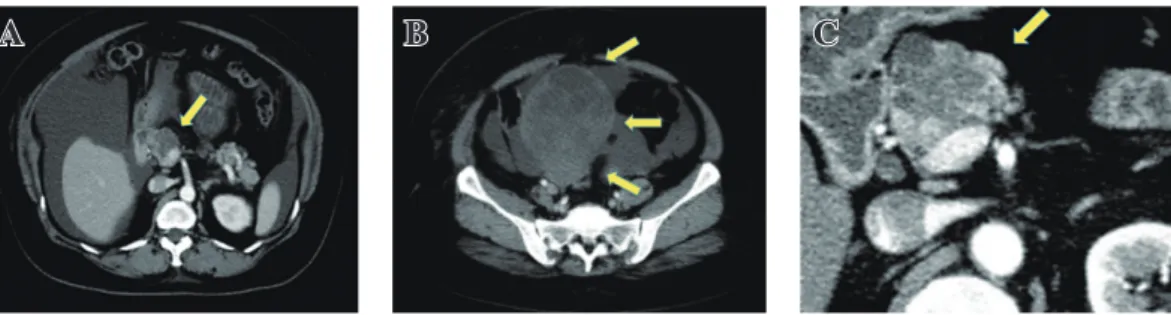
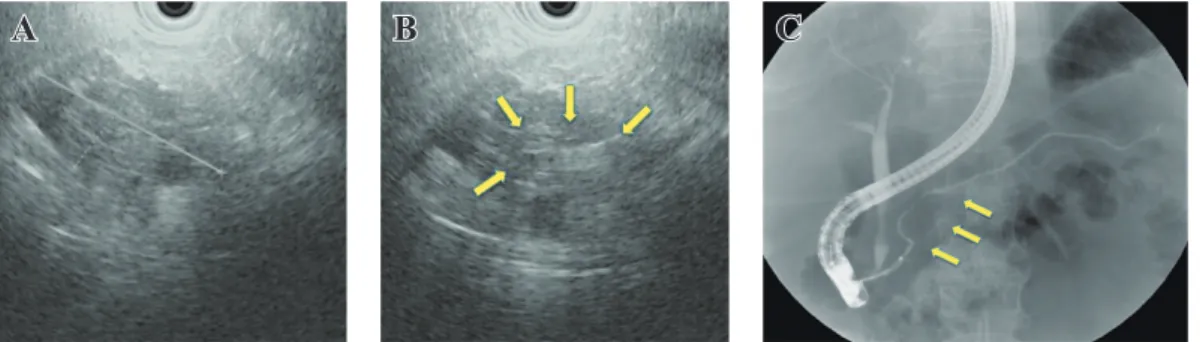
認めた.Meigs症候群による腹水の貯留も認 めている(Fig. 1A).12.0×8.6 cmの右卵巣莢 膜細胞腫(Fig. 1B).14ヶ月後のCT画像. 嚢 胞径は2.4 cmより3.5 cmへ拡大していた(Fig. 1C).MRI所見:T2強調画像で膵頭部に4.0cm 程度の多房性嚢胞性腫瘤を認める(Fig. 2A). Magnetic resonance cholangiopancreatography: (MRCP)では明らかな主膵管の拡張は認めない(Fig. 2B).超音波内視鏡検査所見(endo-scopic ultrasound: EUS):膵頭部に5.3×3.0cm 台の小嚢胞集簇(cyst by cyst)を認める(Fig. 3A).内部には嚢胞隔壁周囲に壁在結節を疑 うと充実成分を認める(Fig. 3B).内視鏡的逆 行性胆管膵管造影(endoscopic retrograde cho-langiopancreatography: (ERCP)):膵管の拡張, 狭窄や途絶の像は認めず.膵頭部の膵管は嚢 胞の圧排により変位している.嚢胞内への造 影剤の流入は認めず(Fig. 3C).膵頭部膵管よ り擦過細胞診を施行し,ClassⅢの診断であっ た. 以上より,増大傾向を認める膵嚢胞性腫瘍 であり,EUSで壁在結節の存在を疑う所見も認 め,分枝型のIPMNを否定できなかったため, 幽門輪温存膵頭十二指腸切除術を施行した. 手術所見:膵頭部から膵頸部にかけて4cm台 の嚢胞性病変を認めた(Fig. 4A). 病理組織 学的検査所見: 大型から中型の嚢胞を認め, その上皮は一層性の立方~円柱上皮に覆われ ていた. 内部に粘液は認めず,乳頭状に増殖 するような腫瘍性病変も認めなかった.明ら かな壁在結節も認めず(Fig. 4B).嚢胞の被膜 上皮細胞は,小型立方状で明るい胞体を示し,
Fig. 1.
Measurements of the cyst. A. Diameter of the pancreatic cyst is 2.4 cm, B. Right Thecoma (with Meigs syndrome) 12.0×8.6 cm, C. The cyst expanded from 2.4 to 3.5 cm in 14 months.Fig. 2.
Findings of magnetic resonance cholangiopancreatography. A. The cyst showed high signal intensity, B. Main pancreatic duct was not dilated.A
B
C
A
B
A
B
C
類円形の核を入れる.
胞体にはperiodic acid-Schiff (PAS)陽性顆粒 を示し(Fig. 4C),また,それらはジアスターゼ で消化され,グリコーゲンを豊富に有してい
たことが分かる(Fig. 4D).MIB-1 indexは 1 % 未満であった(Fig. 4E).
以上より,SCAと診断した. 術後 1 年の時 点で再発は認めていない.
Fig. 3.
Findings of ultrasonography. A. Endoscopic ultrasound (EUS) show the cyst 5.3×3.0 cm, B. EUS showed mural nodules within the cyst, C. Main pancreatic duct (MPD) doesnʼt reveal stenosis or dilatation. Cyst press MPD. Cyst isnʼt communicated with MPD.Fig. 4.
Surgical and laboratory findings. A. Section shows the cyst, 4 cm in diameter in pancreatic head, B. The cyst was lined with a single layer of simple cuboidal epithelium, C. D. Periodic acid-Schiff staining, with and without diastase digestion, showed abundant glycogen within cytoplasm of epithelial cells, yielding a definitive diagnosis of SCA, E. MIB-1 index is less than 1%.A
A
B
C
C
D
E
B
A
A
B
C
C
D
E
B
引 用 文 献
1 . Compagno J & Oertel JE (1978): Microcystic adenomas of the pancreas (glycogen-rich cystade-nomas): a clinicopathologic study of 34 cases. Am J Clin Pathol 69: 289-298
2 . 日本膵臓学会編(2009):膵癌取扱い規約.第6版.金原出版,東京 pp 24-31
3 . Hamilton SR & Aaltonen LA (2000): WHO classification of tumors. In: Pathology and genetics of tumors of the digestive system, LARC Press, Lyon p 204
4 . Hruban RH, Pitman MB & Klimstra DS (2007): Serous cystic neoplasms AFIP Atlas of tumor pa-thology: Tumors of the pancreas 4th series, Am Reg of pathol 6, Washington DC pp 33-50
5 . 一二三倫郎,山根隆明,川口哲,他(2001):膵漿液性嚢胞腺腫の肉眼形態の多様性に関する検 討.胆と膵 22:91-98
6 . 渡邊利広,木村理(2010):診断(分類)と治療:外科手術の適応は.肝胆膵 61:367-381
7 . Tseng JF, Warshaw AL, Sahani DV, Lauwers GY, Rattner DW & Carlos Fernandez-del Castillo C (2005): Serous cystadenoma of the pancreas: tumor growth rates and recommendations for treatment. Ann Surg 242: 413-421
8 . Galanis C, Zamani A, Cameron JL, Campbell KA, Lillemoe KD, Caparrelli D, Chang D, Hruban RH & Yeo CJ (2007): Resected serous cystic neoplasms of the pancreas: a review of 158 patients with recommendations for treatment. J Gastrointest Surg 11: 820-826
9 . Meigs JV (1954): Pelvic tumors other than fibromas of the ovary with ascites and hydrothorax. Obstet Gynecol 3: 471-486
考 察
SCAは1978年,Compagnoらによってmicro-cystic adenoma of the pancreasという疾患概念 として初めて報告された[1]. 膵腫瘍全体の 1 ~ 2 %と比較的稀な膵嚢胞性腫瘍で,glyco-genに富む淡明な細胞で構成される小型の嚢 胞が蜂巣状に集簇する. SCAは国際的に統一された分類はなく,膵癌 取扱い規約第 6 版では病理学的に漿液性嚢胞 腺腫と漿液性嚢胞腺癌の 2 つに分類されてい る[2].また,World Health Organization(WHO) 分類では serous microcystic adenoma,serous oli-gocystic adenomaとserous cystadenocarcinoma に [3],Armed Forces Institute of Pathology (AFIP) の 分類では microcystic serous cystadenoma,macro-cystic serous cystadenoma, solid serous adenoma, von Hippel-Lindau-associated serous cystic neo-plasm,serous cystadenocarcinoma に分類されて おり[4],serous cystic neoplasm(SCN)の範疇に はいるが,各々微妙に異なっている.
一二三らはSCNを数mm単位の小嚢胞腔か ら構成される蜂巣状のtype Ⅰ (microcystic type) と,cm単位の大嚢胞部分が混在して存在する type Ⅱ (macrocystic type)の2型に分類し,さら に各々を亜分類している[5]. 本症例はこの 分類ではtype Ⅱa(macrocystic dominant type) にあたる.また,渡邊らはSCNを1. microcystic type,2. macrocystic type,3. mixed type,4. solid typeに分類しており[6],本症例はこの分類で いくとmixed type にあてはまる.
SCNはその形態の多様性もあり,IPMN, mucinous cyst neoplasm(MCN),神経内分泌腫 瘍のようなmalignant potentialを持つ腫瘍と の鑑別診断が困難であり,腹部超音波,EUS, CT,MRIの所見を総合して診断しなければな らない. SCNはそのほとんどが良性であるが,約1% が悪性とされている[6-8]. 通常,SCNの診断が付けば,経過観察とさ れるが,1. 有症状,2. 高度脈管侵襲,3. 鑑別診 断困難,4. 浸潤性・多結節性発育,急速な増大 傾向,5. 腫瘍径 4 cm以上に該当する症例は, malignant potentialを有するSCNとして,腫瘍局 在,年齢や全身状態を考慮しつつ,外科的切除 を考慮することが望ましいとされている[6]. Tseng JFらの報告によるとSCAの median growth rate は0.60 cm/yearであり,4 cm以下の 腫瘍では0.12 cm/yearであるのに対して,4 cm 以上の腫瘍では1.98 cm/yearであった[7].本 症例では当初2.5 cmであった腫瘍が14ヶ月で 3.5 cmへと増大しており0.94 cm/yearのgrowth rate と,4 cm以下の腫瘍としては通常より急 速な増大傾向を示したため,外科切除の適応 と考えた. 増大傾向の原因を考えると,当初,膵嚢胞性 腫瘤が画像で捉えられた際は,卵巣腫瘍(卵巣 莢膜細胞腫)とともに多量の腹水を認めてい た.一般に,卵巣腫瘍,子宮筋腫などの婦人科 領域の腫瘍で,1. 腹水を伴う,2. 胸水を伴う, 3. 腫瘍摘出により腹水と胸水が消失し再貯 留をしない,という項目を満たすものをMeigs 症候群と呼び[9],本症例も卵巣莢膜細胞腫 によるMeigs症候群を来していたが,卵巣腫瘍 摘出後,腹水が消失したため,腹圧が減少し, 漿液性嚢胞腺腫が増大した可能性が考えられ る.腫瘍は核分裂像をほとんど認めず,MIB- 1 indexも低値であることもこの考えを示唆す る要因である. 結 語 今回,我々は画像上,多房性嚢胞に増大傾向 があり,嚢胞内に壁在結節を疑う所見を認め, IPMNとの鑑別が困難であった膵漿液性嚢胞 腺腫の1例を報告した.
引 用 文 献
1 . Compagno J & Oertel JE (1978): Microcystic adenomas of the pancreas (glycogen-rich cystade-nomas): a clinicopathologic study of 34 cases. Am J Clin Pathol 69: 289-298
2 . 日本膵臓学会編(2009):膵癌取扱い規約.第6版.金原出版,東京 pp 24-31
3 . Hamilton SR & Aaltonen LA (2000): WHO classification of tumors. In: Pathology and genetics of tumors of the digestive system, LARC Press, Lyon p 204
4 . Hruban RH, Pitman MB & Klimstra DS (2007): Serous cystic neoplasms AFIP Atlas of tumor pa-thology: Tumors of the pancreas 4th series, Am Reg of pathol 6, Washington DC pp 33-50
5 . 一二三倫郎,山根隆明,川口哲,他(2001):膵漿液性嚢胞腺腫の肉眼形態の多様性に関する検 討.胆と膵 22:91-98
6 . 渡邊利広,木村理(2010):診断(分類)と治療:外科手術の適応は.肝胆膵 61:367-381
7 . Tseng JF, Warshaw AL, Sahani DV, Lauwers GY, Rattner DW & Carlos Fernandez-del Castillo C (2005): Serous cystadenoma of the pancreas: tumor growth rates and recommendations for treatment. Ann Surg 242: 413-421
8 . Galanis C, Zamani A, Cameron JL, Campbell KA, Lillemoe KD, Caparrelli D, Chang D, Hruban RH & Yeo CJ (2007): Resected serous cystic neoplasms of the pancreas: a review of 158 patients with recommendations for treatment. J Gastrointest Surg 11: 820-826
9 . Meigs JV (1954): Pelvic tumors other than fibromas of the ovary with ascites and hydrothorax. Obstet Gynecol 3: 471-486
Serous Cystadenoma of the Pancreas Showing Enlargement on Images: A Case Report
Mitsuhiro N
akamoto, Noritaka M
inagawaand Koji Y
amaguchiDepartment of Surgery, School of Medicine, University of Occupational and Environmental Health, Japan. Yahatanishi-ku Kitakyushu 807-8555, Japan
Abstract : Serious Cystadenoma (SCA) of the Pancreas is seldom malignant and is usually monitored over
time. Here we report a case of SCA an enlarged cyst that had to be excised because it was difficult to diagnose by intraductal papillary-mucinous neoplasm (IPMN). The patient was a 58-year-old woman with thecoma of the right ovary accompanied by Meigs syndrome, who had undergone abdominal total hysterectomy and bilateral oophorectomy. Abdominal computed tomography scan (CT) showed a multilocular cyst 2.4 cm in di-ameter in the head of the pancreas. Fourteen months later, a periodic CT showed that the multilocular cyst had enlarged from 2.4 to 3.5 cm in diameter. Branch duct intraductal papillary-mucinous neoplasm (IPMN) with a tendency to enlargement and with mural nodule was suspected. Pylorus-preserving pancreatoduodenectomy (PPPD) was performed, and pathological findings revealed that the cyst was lined with a single layer of simple cuboidal epithelium. Periodic acid-Shiff staining, with and without diastase digestion, showed abundant glyco-gen within epithelial cells, yielding a definitive diagnosis of SCA. The ascites were probably due to the Meigs syndrome pressing the cyst, and the size of the cyst appeared smaller than the real size.
Key words: Serous cystadenoma, IPMN, Meigs syndrome.