再生不良性貧血患者に生じた Aspergillus viridinutans による 肺膿瘍の 1 例
1)鳥取大学医学部付属病院呼吸器膠原病内科,2)同 感染制御部,3)同 検査部,4)千葉大学真菌医学研究センター
北浦 剛
1)千酌 浩樹
1)2)室田 博美
3)藤原 弘光
3)唐下 泰一
1)岡田 健作
1)中本 成紀
1)2)井岸 正
1)鰤岡 直人
1)矢口 貴志
4)清水 英治
1)(平成 26 年 4 月 25 日受付)
(平成 26 年 7 月 9 日受理)
Key words : Aspergillus viridinutans, lung abscess, aplastic anemia
序 文
近年,遺伝子解析の発達によりこれまでAspergillus fumigatus(A. fumigatus)とされていた糸状菌の中に 多くの類縁種が存在することが明らかとなってい
る1)〜3).また,類縁種においては,病原性や抗真菌薬
に対する感受性がA. fumigatusと異なる場合があるこ とも知られている4)〜6).Aspergillus viridinutans(A. vi- ridinutans)もその一種であるが,同真菌による感染 症の報告は稀である.今回,免疫不全を有しA. virid-
inutansによる肺膿瘍を生じた症例を経験したため報
告する.
症 例 症例:75 歳,女性.
主訴:発熱,乾性咳嗽.
既往歴:再生不良性貧血.
生活歴:喫煙歴なし,飲酒;焼酎 0.5 合!日.
現病歴:患者は再生不良性貧血のため,当院血液内 科にて蛋白同化ステロイド内服,週 1 回の赤血球・血 小板輸血,抗真菌薬および ST 合剤の予防内服(flu- conazole 200mg!日,trimethoprim-sulfamethoxazole 80mg!日)を受けていた.
当科入院 1 カ月前より軽度の乾性咳嗽が出現し,胸 部 CT で左肺下葉胸膜直下に 2cm 大の結節影を指摘 された.当科紹介となり,経皮的穿刺を施行,淡黄色 の 膿 汁 を 吸 引 し た.肺 膿 瘍 を 疑 い amoxicillin- clavulanic acid 750mg!日+amoxicillin 750mg!日によ る治療を開始した.1 週間後 39℃ 台の発熱の出現,胸
部 CT 上結節影が増大するなど臨床所見の改善を認め ず,穿刺液の培養検査でアスペルギルス様の糸状菌を 検出したためアスペルギルスによる肺膿瘍の疑いで入 院となった.
入院時身体所見:身長 145.6cm,体重 44.5kg.意識 清明,体温 38.3℃,血圧 104!49mm!Hg,脈拍 83 回!
分,SpO2 95%(room air),結膜;軽度貧血あり・黄 疸なし.胸部;心音清・肺副雑音聴取せず.腹部;明 らかな異常所見なし.四肢;浮腫なし.
入院時血液検査:好中球減少(484!μL),Hgb 低下
(7.0g!dL),血小板減 少(1×104!μL),Cr 上 昇(1.09 mg!dL),CRP 上 昇(18.27mg!dL)を 認 め,血 清 ア スペルギルスガラクトマンナン抗原およびアスペルギ ルス沈降抗体が陽性であった.血清β-D グルカンは 陰性であった.
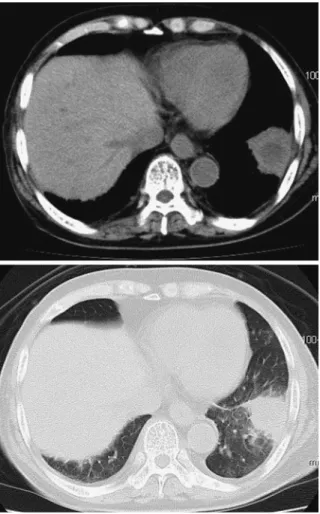
入院時胸部 CT 検査:左下葉胸膜直下に 5cm 大の 内部に低吸収域,周囲に浸潤影を伴う腫瘤影を認めた
(Fig. 1).
入院後経過:穿刺液の培養検査にて検出された糸状 菌は,形態学的にA. fumigatusが疑われたが,コロニー の色調が白色であり,また顕微鏡所見で分生子の発育 が不良であるなど,やや非典型的な所見であった.
Liposomal amphotericin B(L-AMB)135mg!day(3 mg!kg!day)にて加療開始したが,左下葉の腫瘤影 はさらに増大した.このため入院 15 日目に気管支鏡 検査を施行した.気管支洗浄液を用いた細胞診では,
PAS 染色・Grocott 染色でアスペルギルス様の糸状菌 を認め,培養検査でも初診時と同様の糸状菌を検出し た.同糸状菌による治療抵抗性の肺膿瘍と判断し,入 症 例
別刷請求先:(〒683―8503)鳥取県米子市西町 86 鳥取大学医学部付属病院呼吸器膠原病内科
Fig. 1 Chest CT on admission shows mass shad- ow with central low attenuation area in the left lower lobe
Fig. 2 Clinical course
(VRCZ)の併用療法に変更した.経過中抗菌薬も併 用したが,穿刺液,気管支洗浄液,胸水いずれも嫌気 培養を含めて細菌は検出されず,真菌の単独感染と考 えられた.入院 34 日目の胸部単純 CT で胸水(滲出 性)の出現,炎症反応の上昇,エコー検査で胸腔内に 隔壁を認め,膿瘍の胸腔内穿破が疑われた.随時穿刺 排液によるドレナージを行ったが発熱,炎症反応高値 が持続し,徐々に ADL(activities of daily living)も 低下した.このため入院 44 日目より G-CSF(granulo- cyte colony-stimulating factor)投与を開始したとこ ろ,好中球の上昇とともに炎症反応の低下,画像所見 の改善を認め,全身状態も良好となった.外来加療の 希望から VRCZ 内服とし入院 66 日目退院とした.経 過中 VRCZ の投与量は血中濃度(トラフ値)に基づ き 200〜300mg!日で適宜増減し,トラフ値は 0.9〜3.5 μg!mL で推移した.3.5μg!mL となった時点で幻視が 出現したため投与量を減量,血中濃度低下後症状は消 失した.その後も外来にて VRCZ 内服を継続してい るが,肺病変の再発は認めていない(Fig. 2).
検出された真菌の同定を千葉大学真菌医学研究セン ターにて行った.検鏡所見では大型,フラスコ形の頂 のう,球形,粗面の分生子などの形態がA. fumigatus に類似する菌株が得られた(Fig. 3).しかし,A. fumi-
gatusと異なり 48℃ 下での培養で生育を認めず,ポテ
ト・デキストロース寒天培地,25℃,14 日間の培養 でも分生子の形成が悪く,白色のコロニーとなった
(Fig. 3).また,β-tubulin 遺伝子の塩基配列を決定し,
Fig. 3 Image of Aspergillus viridinutans (IFM 61579) culture on Potato Dextrose Agar (PDA) medium at 25℃ at 14 days (A) and microscopical examination (B) (C). (Bars=
10μm)
Clustal X を 用 い て 関 連 種 と 系 統 樹 を Neighbor- joining 法で描いたところ,A. viridinutansの分岐群に 含まれた.系統樹の統計学的有意性の検証は Boot- strap 法(1,000 回試行)により行い,起因菌 IFM 61579 株を含む分岐は高い Bootstrap 値で支持された(Fig.
4).以上の形態的,分子系統的所見から,A. viridinutans と同定した.
考 察
A. viridinutansはA. fumigatus類 縁 種 に 分 類 さ れ1)7)8),広く土中等に存在するものである9).形態学的
にはA. fumigatusに類似し判別は困難であるが,分生
子の形成量が少なく,最高生育温度が低い点は異な る10).本症例においても,分生子の形成量が少なく,
コロニーの色調が白色調であり典型的なA. fumigatus の特徴とは異なっていたため,詳細な同定を行った.
A. viridinutansによる感染症の報告は極めて稀であ
り,著者らの調べた限りでは本邦における詳細な感染 症症例の報告はない.世界においては呼吸器感染症と して 4 例が報告されており10)〜12),患者はすべて何らか の免疫不全を有していた.その他角膜への感染例が 1 例存在する13).本例を含む呼吸器感染症 5 例の報告の うち 4 例が肺膿瘍を呈している(頸部膿瘍,縦隔膿瘍 の合併を 1 例ずつ含む)(Table 1).Vinh らもA. vi-
ridinutansによる肺感染症が,慢性的な経過をとり,解
剖学的に隣接した臓器に広がっていく傾向があること を記述している10).これは免疫不全者におこるA. fumi-
gatusによる侵襲性肺アスペルギルス症が急速に進行
し,血管侵襲や血行性の播種を伴うのとは明らかに異 なる経過である.A. viridinutansと近縁であるN. uda-
tusと比べ低いことが示されており6),A. viridinutans においても同様に病原性・侵襲性の低さが,本臨床的 特徴をもたらしている可能性がある.
A. viridinutansのポリエン系,アゾール系等の抗真
菌薬に対する感受性はA. fumigatusに比べ低いことが 報告されている.A. fumigatusでは,amphotericin B,
VRCZ に対する MIC はいずれも 0.5〜1.0μg!mL 以下 である場合が多いが14)15),これまでに報告されたA. vi- ridinutansにおいてはそれぞれ 1〜8μg!mL,1〜4μg!
mL と高値を示しており(Table 2),予後も不良であっ た.本例も MIC はそれぞれ 2μg!mL, 4μg!mL と高く,
これら抗真菌薬のみでは十分な臨床効果は得らなかっ た一因と考えられた.一方,本症例では CPFG+VRCZ の併用療法に変更後も病状の悪化を認めた.その後,
再生不良性貧血の白血病化を懸念し使用を控えていた G-CSF の併用を開始したところ,明らかに臨床症状,
検査所見の改善を認めた.以上の経過からは G-CSF が本症例の改善に最も寄与したと考えられ,抗真菌薬 に対し低感受性の菌種による肺アスペルギルス症に対 して,G-CSF 投与などによる宿主状態の改善が有用 である可能性が示された.
A. viridinutansによる肺膿瘍の 1 例を経験した.A.
fumigatusには臨床経過や薬剤感受性が大きく異なる
類縁種が存在する.従ってアスペルギルス様の糸状菌 が検出された場合には,A. fumigatus類縁種の可能性 を念頭に置く必要がある.殊に慢性に拡大する病変を 認める,ポリエン系及びアゾール系薬への反応が乏し い,分生子の形成が乏しく白色調のコロニーとなる等 の特徴を有する場合には,A. viridinutansによる感染
Fig. 4 Phylogenetic tree of Aspergillus viridinutans (IFM 61579) and the related species.
Table 1 The five cases with pulmonary disease due to A. viridinutans.
Age Sex Underlying disease Diagnosis Outcome
Vinh, et al.10) 14 M Chronic granulomatous disease Lung/mediastinum abscess Cure
8 M Hyperimmunoglobulin-E syndrome Lung abscess Death
Coelho, et al.11) 56 M Rheumatoid arthritis, Diabetes Lung/neck abscess Death
Pelaez, et al.12) 48 F Acute lymphocytic leukemia IPA Death
Our case 75 F Aplastic anemia Lung abscess Improved
IPA: invasive pulmonary aspergillosis
Table 2 Antifungal susceptibility of A. viridinutans isolated from clinical specimens.
Age Sex Amphotericin B
(MIC; μg/mL) Itraconazole
(MIC; μg/mL) Voriconazole
(MIC; μg/mL) Posaconazole
(MIC; μg/mL) Caspofungin
(MEC; μg/mL) Micafungin (MEC; μg/mL)
Vinh, et al.10) 14 M 4 1 1 0.06 0.25
8 M 2-8 8 2-4 ≦0.016-0.5 0.06-0.25
Coelho, et al.11) 56 M 1 >16 4 0.25 ≦0.016
Pelaez, et al.12) 48 F 1 1 0.5 1 <0.03
Our case 75 F 2 4 4 ≦0.015
MIC: minimal inhibitory concentration, MEC: minimal effective concentration
本論文の主旨は,第 87 回日本感染症学会学術講演 会(2013 年 6 月)において報告した.
利益相反自己申告:申告すべきものなし 文 献
1)Yaguchi T, Horie Y, Tanaka R, Matsuzawa T, Ito J, Nishimura K:Molecular phylogenetics of multiple genes on Aspergillus section Fumigati isolated from clinical specimens in Japan. Japa- nese journal of medical mycology 2007;48
(1):37―46.
2)Balajee SA, Houbraken J, Verweij PE, Hong SB, Yaghuchi T, Varga J,et al.:Aspergillus species identification in the clinical setting. Studies in mycology 2007;59:39―46.
3)Hong SB, Go SJ, Shin HD, Frisvad JC, Samson RA:Polyphasic taxonomy of Aspergillus fumiga- tus and related species. Mycologia 2005;97
(6):1316―29.
4)Balajee SA, Gribskov J, Brandt M, Ito J, Fother- gill A, Marr KA:Mistaken identity :Neosartorya pseudofischeriand its anamorph masquerading as Aspergillus fumigatus. Journal of clinical microbi- ology 2005;43(12):5996―9.
5)Montenegro G, Sanchez Puch S, Jewtuchowicz VM, Pinoni MV, Relloso S, Temporitti E,et al.:
Phenotypic and genotypic characterization of Aspergillus lentulusandAspergillus fumigatus iso- lates in a patient with probable invasive asper- gillosis. Journal of medical microbiology 2009;
58(Pt 3):391―5.
6)Sugui JA, Vinh DC, Nardone G, Shea YR, Chang YC, Zelazny AM,et al.:Neosartorya udagawae (Aspergillus udagawae), an emerging agent of as- pergillosis : how different is it from Aspergillus fumigatus? Journal of clinical microbiology 2010;48(1):220―8.
7)Katz ME, Dougall AM, Weeks K, Cheetham BF:Multiple genetically distinct groups re- vealed among clinical isolates identified as atypi- cal Aspergillus fumigatus. Journal of clinical mi- crobiology 2005;43(2):551―5.
8)Alcazar-Fuoli L, Mellado E, Alastruey-Izquierdo A, Cuenca-Estrella M, Rodriguez-Tudela JL:
Aspergillus section Fumigati: antifungal suscepti- bility patterns and sequence-based identifica- tion. Antimicrobial agents and chemotherapy 2008;52(4):1244―51.
9)Varga J, Toth B, Rigo K, Debets F, Kozakiewicz Z:Genetic variability within the Aspergillus vi- ridinutans species. Folia microbiologica 2000;45
(5):423―8.
10)Vinh DC, Shea YR, Jones PA, Freeman AF, Zelazny A, Holland SM:Chronic invasive as- pergillosis caused by Aspergillus viridinutans.
Emerging infectious diseases 2009;15(8):
1292―4.
11)Coelho D, Silva S, Vale-Silva L, Gomes H, Pinto E, Sarmento A,et al.:Aspergillus viridinutans: an agent of adult chronic invasive aspergillosis.
Medical mycology : official publication of the In- ternational Society for Human and Animal My- cology 2011;49(7):755―9.
12)Pelaez T, Alvarez-Perez S, Mellado E, Serrano D, Valerio M, Blanco JL,et al.:Invasive asper- gillosis caused by cryptic Aspergillus species : a report of two consecutive episodes in a patient with leukemia. Journal of medical microbiology 2013;62:474―8.
13)Shigeyasu C, Yamada M, Nakamura N, Mizuno Y, Sato T, Yaguchi T:Keratomycosis caused by Aspergillus viridinutans: an Aspergillus fumigatus-resembling mold presenting distinct clinical and antifungal susceptibility patterns.
Medical mycology : official publication of the In- ternational Society for Human and Animal My- cology 2012;50(5):525―8.
14)Pfaller MA, Messer SA, Boyken L, Rice C, Ten- dolkar S, Hollis RJ,et al.:In vitro survey of tria- zole cross-resistance among more than 700 clini- cal isolates ofAspergillusspecies. Journal of clini- cal microbiology 2008;46(8):2568―72.
15)Espinel-Ingroff A, Johnson E, Hockey H, Troke P:Activities of voriconazole, itraconazole and amphotericin B in vitro against 590 moulds from 323 patients in the voriconazole Phase III clinical studies. The Journal of antimicrobial chemotherapy 2008;61(3):616―20.
A Case of Lung Abscess Due toAspergillus viridinutansin a Patient with Aplastic Anemia
Tsuyoshi KITAURA1), Hiroki CHIKUMI1)2), Hiromi MUROTA3), Hiromitsu FUJIWARA3), Hirokazu TOUGE1), Kensaku OKADA1), Masaki NAKAMOTO1)2), Tadashi IGISHI1), Naoto BURIOKA1),
Takashi YAGUCHI4)& Eiji SHIMIZU1)
1)Department of Multidisciplinary Internal Medicine, Faculty of Medicine, Tottori University,2)Center for Infectious diseases and3)Department of Clinical Laboratory, Tottori University Hospital, 4)Medical Mycology Research Center,
Chiba University
A 75-year-old woman with aplastic anemia was admitted to our university hospital because of a dry cough that had persisted for a month. Chest computed tomography showed a mass shadow with a central low attenuation area in the lower lobe of the left lung. Filamentous fungus resemblingAspergillus fumigatus was cultured from the specimens obtained by transthoracic needle aspiration biopsy and bronchoalveolar lavage. The initial diagnosis was a lung abscess due to A. fumigatus, although the patient did not respond well to antifungal agents. Subsequently, the filamentous fungus was identified as Aspergillus viridinutansby sequence analysis of theβ-tubulin gene, and the patient was successfully treated with combination therapy along with granulocyte colony-stimulating factor.
The incidence ofA. viridinutans infection is very rare.A. viridinutansis morphologically similar to A. fu- migatus; however,the response to antifungal agents is generally worse than that observed inA. fumigatus in- fections. Therefore, the selection of agents and supplemental therapy is of vital importance in cases ofA. vi- ridinutansinfection.
〔J.J.A. Inf. D. 88:855〜860, 2014〕