序 文
脳室炎は,新生児では化膿性髄膜炎に併発する ことが多く1)2),成人では外傷,脳膿瘍,手術によ る脳室周囲の処置などを契機に発症し3)4),経過は 重篤で致死率は高い.今回我々は,肝膿瘍の治療 中に化膿性髄膜炎及び脳室炎を併発した成人の 1 症例を経験し,若干の考察を加え報告する.
症 例 患者:45 歳,男性.
主訴:発熱.
既往歴:2000 年頃より高脂血症, 高尿酸血症.
家族歴:特記事項なし.
現病歴:2002 年 1 月 21 日ごろより悪寒,戦慄 を伴う 39℃ 以上の発熱を認め,経過観察をしてい たが,全身衰弱がひどくなり,1 月 25 日当院を受 診した. 来院時,白血球増多,CRP 高値を認め,
腹部 CT 上,肝右葉に多房性の低吸収域像を呈し たため,多発性肝膿瘍と診断し入院となった.
入 院 時 現 症:身 長 173cm,体 重 78kg,体 温 39.5℃,血圧 110!64mmHg,脈拍 96!分,整,呼吸 数 24!分.眼瞼結膜貧血なし,眼球結膜黄染あり,
意識清明,心雑音なし,呼吸音清,腹部は平坦で 右季肋部の圧痛を認めた.神経学的所見に異常所 見を認めなかった.
入院後経過(Table 1,Fig. 2):白血球増多,CRP 上昇などの炎症所見に加え,肝機能障害を認め,
腹部 CT 上,肝右葉 S5,S8 を中心に多房性の低吸 収域を呈することから(Fig. 1),細菌性肝膿瘍と診 断した.培養検査では血液と肝膿瘍のドレナージ よりKlebsiella pneumoniaeを検出したが,髄液から 起炎菌は同定されなかった.入院後,肝膿瘍に対 して sulbactam sodium!cefoperazon sodium
(SBT!CPZ)2g!日,minocycline hydrochloride
(MINO)200mg!日を開始した.また入院翌日より 成人呼吸促迫症候群を併発し,methylpredniso- lone sodium succinate(M-PSL)1,000mg!日を 3 日 間投与し,その後は後療法として PSL の内服を 行った.1 月 28 日頃より頭痛が増強し,項部硬直,
Kernig 徴候と髄膜刺激症状を認め, 髄液検査上,
細胞数 8,336!3(単核球 816,分葉核球 7,520)!mm3 であり化膿性髄膜炎と診断した.髄液移行性を考 慮 し,ceftriaxone(CTRX)4g!日,meropenem trihydrate(MEPM)2g!日へと抗生物質の変更を 行った.以降,神経症状は軽快し,炎症所見も改 善傾向であったため,2 月 5 日より CTRX の単独 投与に変更したが,肝膿瘍の改善がみられないた め,2 月 9 日に経皮的膿瘍 ド レ ナ ー ジ を 行 い,
MEPM を再開した.以後経過良好となり,髄液所 見 も 著 明 に 改 善 し て き た た め,2 月 17 日 に MEPM を中止した.しかし 2 月 22 日,複視を訴 え, 左下直筋の眼球運動制限を呈し, 頭部 MRI,
症 例
肝膿瘍の治療中,化膿性髄膜炎および脳室炎を併発した 1 例
1)聖マリアンナ医科大学神経内科,2)同消化器肝臓内科
本間 裕子
1)白石 眞
1)柳澤 俊之
1)眞木 二葉
1)杉原 浩
1)高橋 洋一
1)大塚 由佳
2)(平成 15 年 3 月 19 日受付)
(平成 15 年 7 月 8 日受理)
別刷請求先:(〒216―8511)川崎市宮前区菅生 2―16―1 聖マリアンナ医科大学神経内科
本間 裕子
Key words: liver abscess, cerebral ventriculitis, meningitis
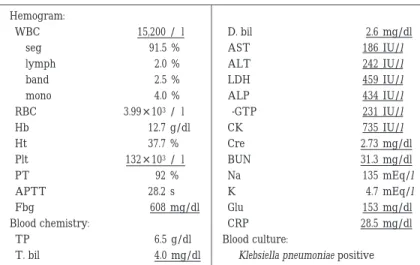
Table 1 Laboratory data on admission
Hemogram:
D. bil 2.6 mg/dl
WBC 15,200 /µl
AST 186 IU/l
seg 91.5 %
ALT 242 IU/l
lymph 2.0 %
LDH 459 IU/l
band 2.5 %
ALP 434 IU/l
mono 4.0 %
γ-GTP 231 IU/l
RBC 3.99 × 103 /µl
CK 735 IU/l
Hb 12.7 g/dl
Cre 2.73 mg/dl
Ht 37.7 %
BUN 31.3 mg/dl
Plt 132 × 103 /µl
Na 135 mEq/l
PT 92 %
K 4.7 mEq/l
APTT 28.2 s
Glu 153 mg/dl
Fbg 608 mg/dl
CRP 28.5 mg/dl
Blood chemistry:
Blood culture:
TP 6.5 g/dl
Klebsiella pneumoniae positive
T. bil 4.0 mg/dl
FLAIR 画像で第四脳室の高信号,同部の Gd の造 影効果を認め(Fig. 3),脳室炎と診断した.MEPM を再開し,M-PSL 500mg!日を 3 日間施行した.2 月 26 日頃より複視および眼球運動制限は軽快し,
3 月 14 日に抗生物質の投与を終了した.その後は 症状の再発はなく退院となった.
考 察
本症例は,肝膿瘍の治療中に化膿性髄膜炎を併 発し,さらにその治療中にも関わらず脳室炎を 併った成人の 1 例である.脳室炎は新生児の化膿 性髄膜炎に合併することが多い1)2)が,成人での発 症例は稀であることから,MRI で脳室壁に沿った
異常造影を経験することは少ない5)6).また,最近 では,エイズに伴う cytomegalo virus や単純ヘル ペスウイルスによる脳室炎の報告例があるが7), 化膿性髄膜炎は抗生物質の治療によって良好な経 過を得るため,脳室炎に進展することは少ない.
しかし本症例は,肝膿瘍に髄膜炎を合併したため,
多剤の抗生物質の併用を早期から行っていた.
髄膜炎の成人での経験的治療として,起因菌と して肺炎球菌やインフルエンザ桿菌を考え am- picillin(ABPC),cefotaxime sodium(CTX),ceftri- axone sodium(CTRX)の併用が従来行われてい た.しかし近年では,ペニシリン及びβラクタム 系抗生物質に対する肺炎球菌の耐性が問題とな り,ペニシリン低感受性株や耐性菌に有効で,リ ス テ リ ア 菌 な ど を 広 く カ バ ー す る MEPM や VCM の併用が行われてきている8).また,小児の インフルエンザ菌性髄膜炎においての,抗生物質 とステロイドとの併用の有用性が指摘されてい る9)10).また最近では成人の細菌性髄膜炎におい て の ス テ ロ イ ド の 有 用 性 に つ き 検 討 さ れ て お り11),その報告によると成人細菌性髄膜炎症例に 対するステロイド療法は,不良な転帰のリスク,
死亡率を減少させると報告されている.本症例で は化膿性髄膜炎に対してではなく,成人呼吸促迫 症候群に対して止むを得ずステロイドの投与を 行っていた.よって本症例においての良好な転帰 Fig. 1 Liver abscesses are localized in the right lobe
on CT scans. These abscesses appear as hypodense round lesions with irregular borders.
感染症学雑誌 第77巻 第11号
A B Fig. 2 Clinical course
Fig. 3 On the 40th day after the onset, FLAIR images(SE 6,000!120)(A)and T1- weighted MRI(SE 480!12)with gadolinium enhancement(B)revealed ventric- ulitis in the 4th ventricle. The ventriculitis was clearly demonstrated especially on T1-weighted image with gadolinium-enhanced, which showed pronounced the focal lesion.
は,ステロイドの投与が関与していると推測した.
本症例の抗生物質の選択に際しては,肝膿瘍が あることから CTRX,MEPM を empirical に選択 した.後にK. pneumoniaeが同定され,CTRX およ び MEPM 両薬剤ともディスク法での感受性テス トが有効であり,使用薬剤に問題はなかったとい える.しかし CTRX 単剤投与の時期に脳室炎を併 発したことを考えると,臨床的に CTRX に耐性で MEPM に有効であった症例とも考えられた.また 本症例の問題点として,長期の抗生物質投与によ る薬剤の耐性化や肝機能障害の増悪を恐れたた め,抗生物質の長期併用療法を行えなかったこと が,長期治療中の脳室炎発症に関与していると思 われた.今後,化膿性髄膜炎および脳室炎におい て,抗生物質の選択,投与量,および投与期間に ついて,十分な注意をはらい,集中的な治療を行っ ていくことが重要と考えた.
文 献
1)Gilles FH, Jammes JL, Berenberg W:Neonatal meningitis. Arch Neurol 1977;34:560―2.
2)Salmon JH:Ventriculitis complicating meningi- tis. Amer J Dis Child 1972;124:35―40.
3) Osborn JS , Sharp S , Hanson EJ , MacGee E , Brewer JH:Staphilococcus epidermides ventric- ulitis treatment with vancomycin and rifanpicin.
Neurosurgery 1986;19:824―7.
4)Walsh TJ, Schlegel R, Moody MM, Costerton JW,
Salcman M:Ventriculoatrial shunt infection due to Cryptococcus neoformans:An ultrastructural and quantitative microbiological study. Neurosur- gery 1986;18:373―5.
5)吉村菜穂子,相馬芳明:発症早期に頭部 MRI で 脳室炎の所見を示した結核性髄膜脳炎の 1 剖検 例.神経内科 1993;38:597―601.
6)Barloon TJ, Yuh WT, Knepper LE, Biller J, Ryals TJ, Sato Y:Cerebral ventriculitis:MR findings.
J Comput Assist Tomogr 1990;14:272―5.
7)Laskin OL, Stahl-Bayliss CM, Morgello S:Con- comitant herpes simplex virus type 1 and cy- tomegalovirus ventriculoencephalitis in acquired immunodeficiency syndrome. Arch Neurol 1987;44:843―7.
8)American academy of pediatrics, committee on infectious disease:Therapy for children with in- vasive pneumococcal infections. American Acad- emy of Pediatrics Committee on Infectious Dis- eases. Pediatrics 1997;99:289―99.
9)McIntyre PB, Berkey CS, King SM, Schaad UB, Terhi K, Kanra GY,et al.:Dexamethasone as ad- junctive therapy in bacterial meningitis. A meta- analysis of randomized clinical trials since 1988. J.
A.M.A 1997;278:925―31.
10)Coyle PK:Glucocorticoids in central nerves sys- tem bacterial infection. Arch Neurol 1999;56:
796―801.
11)J De Gans, D Van De Beek:Dexamethasone in Adults with Bacterial Meningitis. N Engl J Med 2002;347:1549―56.
感染症学雑誌 第77巻 第11号
A Case of Ventriculitis with Bacterial Meningitis Occurred during the Treatment of Liver Abscess Yuko HONMA1), Makoto SHIRAISHI1), Toshiyuki YANAGISAWA1), Futaba MAKI1),
Hiroshi SUGIHARA1), Yoichi TAKAHASHI1), and Yuka OTSUKA2)
1)Division of Neurology,2)Gastroentelogy, St. Marianna University School of medicine
A 47-case-year old male was admitted to our hospital because of high fever and general fatigue.
He had no immune deficiency, and had no other disease in his past history. On admission, the white blood cell count and C-reacted protein were severely elevated(18,700!µl, 27. 7mg!dl, respectively)
and abdominal CT revealed multiple low density, From these results, he was diagnosed as liver ab- scess. Intravenous MINO and SBT!CPZ injection were started. On the fifth hospital day, he suffered from headache and nuchal rigidity. The clinical data revealed the cerebro-spinal fluid(CSF)counting 8,336 cells!mm3(mononuclear 8,000,)protein at 119mg!dl, and sugar 42mg!dl. CSF cultures were negative, but Klebsiella was recognized in the blood culture and drainage fluid in liver abscess. This condition was diagnosed as bacterial meningitis and antibiotics were changed to intravenous CTRX and MEPM. Furthermore we administered oral PSL and intravenous steroid-pulse therapy. After these combination therapies his condition improved gradually. After 40 hospital day, however, he suddenly had double vision, Axial FLAIR(SE6,000!120)image revealed with high signal intensity at 4th ventricle. Intravenous MEPM was administered again. On the 60thhospital day, double vision was gradually improved and abnormal intensity at 4thventricle was almost disappeared. This case may provide us a considerable suggestion on the treatment of bacterial meningitis.
〔J.J.A. Inf. D. 77:977〜981, 2003〕