Anterior Cruciate Ligament Reconstruction
using Hamstring Tendon
Comparison between Single-and Double-Bundle Technique
Kazuhisa Hatayama,
Hiroshi Higuchi,
Masanori Terauchi,
and Kenji Takagishi
Aim: The purpose of this study was to prospectively compare for clinical outcomes between single-and double-bundle anterior cruciate ligament reconstruction. M ethods: One hundred fifty-three patients who underwent anterior cruciate ligament reconstruction using hamstring tendon were included. Single-or double-bundle reconstruction was perfSingle-ormed fSingle-or 94 (S group) Single-or 59 patients (D group),respectively. At 2 years after surgery, the manual knee laxity test, anterior stability with KT-1000, range of motion, muscle strength and Lysholm score were evaluated. Second-look arthroscopy was performed for each knee. Results: The mean side-to-side difference of the KT 1000 value after surgery was 3.8mm in S group and 3.1mm in D group,which was not significant different. However,the percentage of less than 5mm of anterior knee laxity was significantly larger in D group. Other clinical results were not significantly different between the groups. Conclusions: Clinical outcomes were similar after single-and double-bundle anterior cruciate ligament reconstruction using hamstring tendon.(Kitakanto Med J 2009;59:131∼135)
Key Words: Anterior cruciate ligament reconstruction, Arthroscopy, Double-bundle reconstruc-tion, Hamstring tendon
Introduction
Transtibial anterior cruciate ligament (ACL) re-construction using multi-stranded hamstring tendons has become a popular procedure, similar to bone-patellar tendon-bone because of the good clinical outcome. Until a few years ago, the single-bundle ACL reconstruction, which mimics the anteromedial bundle(AMB),was conventionally performed. Satis-factory anterior stability following single-bundle ACL reconstruction is restored, but a residual rotational instability has been reported. Anatomical researches of native ACL have been vigorously perfor-med to more closely restore normal knee kinematics in the ACL-reconstructed knee. The ACL consists of 2 separate bundles,the AMB and the posterolateral bundle (PLB). These bundles have different func-tions. AMB and PLB are taut throughout the range of motion and at near extension,respectively. In partic-ular,it was clarified that the PLB contributes to anter-olateral rotational stability. Therefore more recently,
several authors have reported the double-bundle recon-struction procedure, which aims to reconstruct both the AMB and PLB of the ACL. Rosenberg et al. reported a bi-socket procedure using hamstring tendon in which 2 femoral sockets were created around the 1 or 11 o clock position. In 1999,Muneta et al.report-ed the double-bundle procal.report-edure with 2 tunnels in the tibia and 2 tunnels in the femur. However,there are few comparative reports concerning the results of these two reconstruction procedures. The purpose of our study was to prospectively compare for the clinical results between the two types of ACL reconstruction techniques performed at our institute.
M aterials and M ethods
Patients
We included 153 patients (90 males, 63 females) undergoing a primary ACL reconstruction using multi-strand hamstring tendon in our institute. They had no combined collateral or posterior cruciate liga-ment surgery. S group was assigned 94 patients (58
1 Department of Orthopaedic Surgery,Social Insurance Gunma Central General Hospital 2 Department of Orthopaedic Sports Surgery, Asakura Sports Rehabilitation Clinic, 249-1 Asakura-machi, Maebashi, Gunma 371-0811, Japan 3 Department of Orthopaedic Surgery, Gunma Graduate School of Medicine
Received : January 23, 2009
Address: KAZUHISA HATAYAMA Department of Orthopaedic Surgery,Social Insurance Gunma Central General Hospital,1-7-13 Koun-cho, Maebashi, Gunma 371-0025, Japan
males,36 females)who underwent single-bundle recon-struction and D group was assigned 59 patients (32 males, 27 females) who underwent double-bundle re-construction. The mean age at surgery was 27.8 years (SD, 7.4years) in S group and 25.4years (SD, 10.2 years) in D group. The mean time from injury to surgery was 8.6 months in S group and 7.2 months in D group. The age, gender and time to surgery were not different between the groups. All patients were followed for a minimum of 2 years. The detailed demographic data of our study are shown in Table 1. This study was a prospective cohort study.
Surgical technique
The arthroscopic ACL reconstruction was perfor-med with the transtibial tunnel technique in all patients. Firstly, the semitendinosus tendon was har-vested in the usual fashion. The semitendinosus ten-don was divided into two parts, and then baseball sutures were performed on both sides of each graft using nonabsorbable No.2 sutures. A hybrid graft was made using Endobuttons (Smith & Nephew, Andover,MA)on the femur side. The tibial side was augmented using a Telos artificial ligament (Telos, Marburg, Germany). In S group, the harvested ten-dons were quadrupled, and in D group, the tenten-dons were doubled for AMB and PLB. After the ACL remnant was debrided, tibial bone tunnel was created using an ACL drill guide(Smith & Nephew,Andover, MA). Femoral tunnels for AMB and PLB were made after notch plasty. In S group, a femoral tunnel was made in the 11 o clock direction on the notch for the right knee(Fig.1A,B). In D group,according to the method reported by Muneta et al, a bone tunnels were made in the 11:30 direction for AMB and in the
10:30 for PLB (Fig. 2A, B). The grafts were passed through each tunnel, femoral fixation was performed with the Endobuttons, and tibial fixation was accom-plished with spike staples (M/E/system Inc.,JA). In S group, the graft was tensioned at 20 degrees of knee flexion with 80N. In D group, each bundle was ten-sioned at 20 degrees of flexion with 40N.
Postoperative Rehabilitation
Both groups followed the same postoperative reha-bilitation protocol. Partial weight bearing was start-ed at 1 week after surgery, followstart-ed by full weight bearing at 3 weeks. Full range of motion was allowed at 3 weeks. Jogging was started at 3 months, and Jumping & cutting exercise was started at 6 months. Sporting exercise was performed at 8 months,and they were subsequently encouraged to return to sports.
Evaluation
Manual knee laxity tests(Lachman test and pivot-shift test) and range of motion were evaluated at 2 years after surgery. Anterior knee laxity was also measured using a KT 1000 arthrometer (Medmetric, San Diego,CA)at 30 degrees of knee flexion under an anterior drawer force of 132 N. Side-to-side displace-ment differences are reported in millimeters. The Lysholm knee score was used to evaluate specific symptoms relating to knee function before surgery and 2 years after surgery.
For analysis of thigh muscle strength, the maxi-mum extension and flexion strengths of both knees were measured using Biodex system 3 (Biodex Medical Systems, Shirley, NY) at 180 degrees/second and ex-pressed as a percentage of the uninjured knee as 100%.
All subjects provided informed consent, and Single and Double-Bundle ACL Reconstruction
Table 1 Patient Demographics
Single-bundle Double-bundle p Value
Number of patients 94 59
Age (years) 27.8±7.4 25.4±10.2 N.S.
Gender (female/male) 58/36 32/27 N.S. Time to surgery(mo) 8.6±5.7 7.2±6.2 N.S. Preoperative KT-1000 (mm) 9.2±3.2 8.5±2.8 N.S. Preoperative Lysholm score 51±15 49±12 N.S. Table 2 Postoperative clinical results
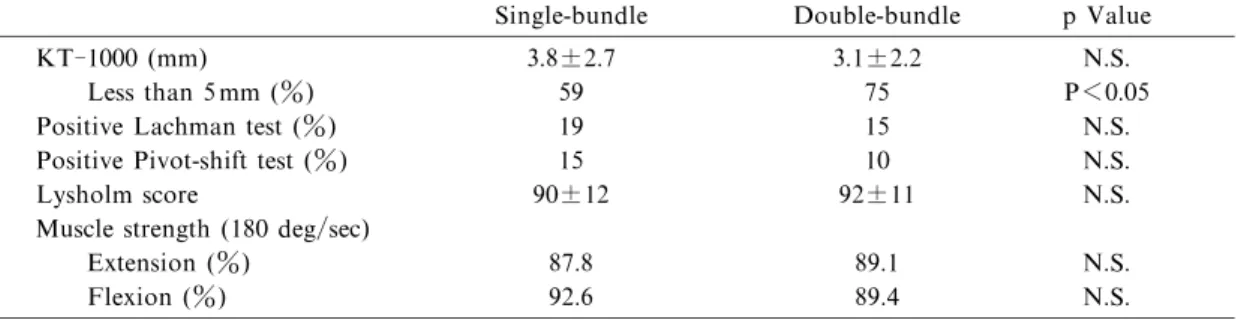
Single-bundle Double-bundle p Value
KT-1000 (mm) 3.8±2.7 3.1±2.2 N.S.
Less than 5mm (%) 59 75 P<0.05
Positive Lachman test (%) 19 15 N.S. Positive Pivot-shift test (%) 15 10 N.S.
Lysholm score 90±12 92±11 N.S.
Muscle strength (180 deg/sec)
Extension (%) 87.8 89.1 N.S.
second-look arthroscopy was performed independently of postoperative symptoms 12 months after surgery. All data were collected prospectively.
Statistical analysis
Statistical analysis was performed using Stat View software (Abacus Concepts). Chi-square test, t-test and the Mann-Whiteney U test were used to compare
Fig. 1a Fig. 1b
Fig.1 (a, b) Postoperative anteroposterior (A) and lateral (B) radiographs in single-bundle procedure.
Fig.2 (a, b) Postoperative anteroposterior (A) and lateral (B) radiographs in double-bundle procedure. Fig. 2b
the 2 groups, and the level of significance was set at P<0.05.
Results
The mean Lysholm score before surgery was 51 points in S group and 49 points in D group. The preoperative Lysholm Score was not different between the groups (P=0.48). The Lysholm score after sur-gery was 90 points in S group and 92 points in D group, which was not significantly different between the groups (P=0.46) (Table 2).
Two years after surgery, the Lachman test was positive in 18 of 94 (19%) in S group and 9 of 59 (15%)in D group. The Pivot-shift test was positive in 14 of 94 (15%) in S group and 6 of 59 (10%) in D group. The results of manual knee laxity tests after surgery were not significantly different between the groups (Lachman : P=0.35, Pivot-shift : P=0.28) (Table 2).
The mean side-to-side difference of the KT-1000 value before surgery was 9.2mm (SD, 3.2mm) in S group and 8.5mm (SD, 2.8mm) in D group. There was no significant difference in the preoperative laxity between the groups(P=0.21). The KT-1000 value at 2 years after surgery was 3.8mm (SD, 2.7mm) in S group and 3.1mm (SD, 2.2mm) in D group, and anterior laxity was significantly improved (P<0.001). However, there was no significant difference between the groups (P=0.15). Fifty-six of the 94 patients (59%)in S group and 44 of the 59 patients(75%)in D group showed a side-to-side difference of less than 5 mm. The percentage of less than 5mm was signifi-cantly larger in the double-bundle procedure(P=0.04) (Table 2).
Eight of the 94 patients(9 %)in S group and 3 of the 59 patients in D group showed loss of knee exten-sion of less than 5 degrees. The range of motion of the knee after surgery was not significantly different between the groups (P=0.32).
When we performed second-look arthroscopy at 1 year after surgery, 24 of the 94 patients (26%) in S group and 17 of the 59 patients (29%) in D group showed partial laceration or elongation of the graft.
The maximum knee extension and flexion strengths measured using Biodex system 3 at 180 degrees/second were 87.8% and 92.6% in S group,and 89.1% and 89.4% in D group, respectively. There were no significant differences between the groups (extension : P=0.38, flexion : P=0.40) (Table 2).
Discussion
Recently, double-bundle ACL reconstruction using hamstring tendons,which is intended to improve clinical results by mimicking the native ACL, have
been reported. However, there are few comparative reports concerning the postoperative outcomes between single- and double-bundle procedures. Adachi et al. conducted a prospective randomized study between single-and double-bundle ACL recon-struction using hamstring tendons. The results of the study showed no significant difference with regard to anterior laxity measured by the KT-2000 arthrometer at 20 or 70 degrees of knee flexion. Muneta et al. retrospectively compared the reconstruction techniques and showed no statistical differences in the IKDC evaluation form and Lysholm score. However, double-bundle reconstruction was superior to single-bundle reconstruction in the Lachman test, anterior drawer test and KT-1000 measurement. Yasuda et al. demonstrated that anatomic double-bundle reconstruc-tion grafted on the posireconstruc-tion based on their anatomical research was significantly better than conventional single-bundle reconstruction in anterior stability and the pivot-shift test.
Although the clinical outcomes following double-bundle ACL reconstruction have been reported, these results can not simply be compared because the femor-al tunnel positions that strongly affect the length change of the graft throughout the range of motion were different among these reports. In this study, we prospectively compared the clinical outcomes between single-and double-bundle reconstructions that created two femoral tunnels, as described by Muneta and colleagues. As a result, there was no significant difference in manual knee laxity tests and anterior laxity measured in the short-term using a KT-1000 arthrometer between the 2 groups. However, we demonstrated that the percentage of less than 5 mm of anterior knee laxity was significantly larger in the double-bundle procedure. On the other hand, the incidence of adverse effects,such as loss of motion and muscle weakness, was not significantly different between the procedures. Although double-bundle reconstruction using two tunnels in the femur and in the tibia is technically more demanding than single-bundle reconstruction, the double-single-bundle procedure may enable improvement of the postoperative out-come. It is necessary to investigate the proper bone tunnel position to mimic the AMB and PLB and the procedure to ensure even tension of both grafts with a different tensioning pattern.
As an advantage of the double-bundle reconstruc-tion, Muneta et al. stated that the increased contact area between the graft and bone tunnel is preferable to enhance graft healing and to achieve stronger graft tissue faster than the usual single-bundle graft. Meanwhile,Howell et al.reported that the angle of the tibial tunnel in the coronal plane correlated with Single and Double-Bundle ACL Reconstruction
anterior laxity after transtibial single-bundle ACL reconstruction and a tibial tunnel angle above 75 degrees was associated with more anterior laxity. Likewise, biomechanical study of the ACL-reconstructed knee in which the femoral tunnel was created at the 10 or 11 o clock position demonstrated that the 10 o clock position, which is more lateral, could further reduce rotatory laxity. In our study, ACL reconstruction was performed with the transtibial tunnel technique in all cases and a femoral tunnel was created at the 1 or 11 o clock position to reconstruct the AMB in the single-bundle procedure. Therefore, the graft would likely impinge on the notch or PCL. In contrast, because both AMB and PLB were recon-structed in D group, the PLB, located more laterally, would compensate for knee instability in cases of AMB failure.
The limitations of our study are to not be random-ized study and follow up period is short. Some authors have reported long-term clinical results after single-bundle ACL reconstruction using hamstring tendons, but in double-bundle reconstruction they were not reported. Further study is required to clarify whether the double-bundle reconstruction procedure has superior long-term stability and the prevention of re-rupture of the ACL,meniscal tear,or progression of osteoarthritis.
In conclusion, both ACL-reconstruction proce-dures produced good clinical results. However,more reliable improvement of anterior knee laxity was found with the double-bundle procedure.
References
1. Adachi N, Ochi M, Uchio Y et al. Reconstruction of the anterior cruciate ligament: Single-versus double-bundle multistranded hamstring tendon. J Bone Joint Surg 2004; 86-B: 515-520.
2. Amis AA,Dawkins PC.Functional anatomy of the anterior cruciate ligament: Fibre bundle actions related to ligament replacements and injuries. J Bone Joint Surg 1991; 73-B: 260-267.
3. Colombet P, Robinson J, Christel P et al.Morphology of anterior cruciate ligament attachments for anatomic recon-struction : A cadaveric dissection and radiographic study. Arthroscopy 2006; 22: 984-992.
4. Ferretti M,Ekdahl M,Shen W et al. Osseous landmarks of the femoral attachment of the anterior cruciate ligament: An anatomic study. Arthroscopy 2007; 23: 1218-1225. 5. Hamada M, Shino K, Horibe S et al. Single-versus
bi-socket anterior cruciate ligament reconstruction using autogenous multiple-stranded hamstring tendons with en-dobutton femoral fixation : A prospective study.
Arthros-copy 2001; 17: 801-807.
6. Howell SM, Gittins ME, Gottlieb JE et al. The relation-ship between the angle of the tibial tunnel in the coronal plane and loss of flexion and anterior laxity after anterior cruciate ligament reconstruction. Am J Sport Med 2001; 29 : 567-574.
7. Keays SL, Bullock-Saxton JE, Keays AC et al. A 6-year follow-up of the effect of graft site on strength, stability, range of motion, function, and joint degeneration after anterior cruciate ligament reconstruction : Patellar tendon versus semitendinosus and gracilis tendon graft.Am J Sport Med 2007; 35: 729-739.
8. Liden M, Ejerhed L, Sernert N et al. Patellar tendon or semitendinosus tendon autografts for anterior cruciate liga-ment reconstruction : A prospective randomized study with a 7-year follow-up. Am J Sport Med 2007; 35: 740-748. 9. Loh JM,Fukuda Y,Tsuda E et al. Knee stability and graft
function following anterior cruciate ligament reconstruc-tion : Comparison between 11 o clock and 10 o clock femor-al tunnel placement. Arthroscopy 2003; 19 : 297-304. 10. Mae T, Shino K, Miyama T et al. Single-versus
two-femoral socket anterior cruciate ligament reconstruction technique: Biomechanical analysis using a robotic simu-lator. Arthroscopy 2001; 17: 708-716.
11. Mochizuki T, Muneta T, Nagase T et al. Cadaveric knee observation study for describing anatomic femoral tunnel placement for two-bundle anterior cruciate ligament recon-struction. Arthroscopy 2006; 22: 356-361.
12. Muneta T, Sekiya I, Yanagishita K et al. Two-bundle reconstruction of the anterior cruciate ligament using semitendinosus tendon with endobutton : operative tech-nique and preliminary results.Arthroscopy 1999 ; 15: 618-624.
13. Muneta T, Koga H, Morito T et al. A retrospective study of the midterm outcome of two-bundle anterior cruciate ligament reconstruction using quadrupled semitendinosus tendon in comparison with one-bundle reconstruction. Arthroscopy 2006; 22: 252-258.
14. Rosenberg TD, Graf B. Techniques for ACL reconstruc-tion with multi-trac drill guide. Mansfield, MA : Acufex Microsurgical Inc. 1994.
15. Scopp JM, Jasper LE, Belkoff SM et al. The effect of oblique femoral tunnel placement on rotation constraint of the knee reconstructed using patellar tendon autografts. Arthroscopy 2004; 20: 294-299.
16. Woo SL,Kanamori A,Zeminski J et al. The effectiveness of reconstruction of the anterior cruciate ligament with hamstrings and patellar tendon : cadaveric study comparing anterior tibial and rotational loads. J Bone J Surg 2002; 84-A : 907-914.
17. Yagi M, Wong EK, Kanamori A et al. Biomechanical analysis of an anatomic anterior cruciate ligament recon-struction. Am J Sports Med 2002; 30: 660-666.
18. Yasuda K, Kondo E, Ichiyama H et al. Clinical evalua-tion of anatomic double-bundle anterior cruciate ligament reconstruction procedure using hamstring tendon grafts: Comparisons among 3 different procedures. Arthroscopy 2006; 22: 240-251.