緒 言 抗 リ ン 脂 質 抗 体 症 候 群(Antiphospholipid syn-drome: APS)は病原性自己抗体である抗リン脂質抗 体(antiphospholipid antibodies(aPL)) の 存 在 下 で 認められる血栓傾向を示す疾患である1−3).報告に よっても異なるが,aPL は全身性エリテマトーデス (systemic lupus erythematosus (SLE))の 40%程度に
合併するとされる4, 5).APS の血栓症は再発傾向が 強いため,予防治療(2 次予防)が必須だが6, 7), 一方で画一的な治療は不適切である.例えば,aPL は感染症や自己免疫疾患,悪性疾患や肝疾患や健常 人でも出現することがあるが8−10),健常人で偶発的 に検出されたaPL の血栓症発症リスクは低く(年
間1%)11),aPL 陽性の SLE が APS を続発するのは 40%とされている12, 13).一方,APS では 2 次予防下 でも血栓症を繰り返し,著しい生活の質の低下を認 める一群もある14).そのため,APS における最も重 総 説
抗リン脂質抗体症候群における血栓症リスクのスコア化
奥 健 志
The scoring system for the risk-stratification in patients with the antiphospholipid syndrome
Kenji OkuDepartment of Medicine II, Hokkaido University Graduate School of Medicine, Sapporo, Japan
(Accepted October 17, 2017)
summary
Antiphospholipid syndrome (APS) is a clinical disorder characterized by thrombosis and/or pregnancy morbidity in the persistence of the pathogenic autoantibodies, the antiphospholipid antibodies (aPL). Recurernt thrombosis is often observed in patients with APS which requires persistent prophylaxis. However, an uniform prophylactic treatment for APS patients is inad-equate and stratification of the thrombotic risks is important as aPL are prevalently observed in other various diseases or elderly population. It is previously known that the multiple positivity or high titre of aPL correlate to the thrombotic events. To prog-ress the stratification of the thrombotic risks and to quantitatively analyze them, antiphospholipid score (aPL-S) and the Global Anti-Phospholipid Syndrome Score (GAPSS) were defined as the scoring-systems. Both of these scoring-systems were raised from the large patient cohort data and either aPL profile classified in detail (aPL-S) or simplified aPL profile with classical thrombotic risk factors (GAPSS) were put into scoring system. They have shown a degree of accuracy in identifying high-risk APS patients, especially those at a high risk of thrombosis. However, there are several areas requiring improvement, or at least that clinicians should be aware of, before these instruments are applied in clinical practice. One such issue is standardisation of the aPL tests, including general testing of phosphatidylserine dependent antiprothrombin antibodies (aPS/PT).
Key words antiphospholipid syndrome; antiphospholipid antibodies; antiphospholipid score; GAPSS
抄 録
抗リン脂質抗体症候群(APS) は病原性自己抗体である抗リン脂質抗体(aPL)の存在下で出現する血栓性疾患で
ある.APS にともなう血栓症は難治性で再発傾向が高いため,通常永続的な 2 次予防治療が必要だが,画一的な治
療は問題が多い.実際に高力価のaPL や多の aPL が併存する場合はより血栓症のリスクが高くなることが知られ
ている.すなわち,aPL のプロファイルの違いが血栓リスクの違いにつながるわけだが,その血栓リスクの違いを 定量化するために抗リン脂質抗体スコア(aPL-S)と Global Anti-Phospholipid Syndrome Score(GAPSS)が樹立され た.これらはいずれも大規模な患者コホートのデータをもとに作成され,aPL-S は,aPL の力価や種類の違いによ る血栓リスクにより注目し,GAPSS は aPL プロファイルを極めて単純化して,更に古典的血栓リスク因子を加え
たものである.これらは,高リスクのAPS 患者(もしくは aPL 陽性非 APS 患者)を抽出する機能が高いことが示
されている.ただし,これらが臨床応用されるにはaPL 測定系の標準化や現在は国際分類基準に含まれていない
ホスファチジルセリン依存性抗プロトロンビン抗体の取り扱いなど解決しなければ問題がいくつかある.
要な関心事は,血栓症リスクの多寡を適切に評価 し,治療の適正化を図ることである. 血栓症リスク因子としての抗リン脂質抗体 抗リン脂質抗体と総称されるもののうち,病原性 を有する自己抗体は,抗カルジオリピン抗体(anti-cardiolipin antibody(aCL)IgG/IgM),抗 β2グリコプ ロテインI 抗体 anti-β2 glycoprotein I(anti-β2GPI anti-body(aβ2GPI))IgG/IgM とループスアンチコアグラ ント(lupus anticoagulant(LAC))が分類基準に挙 げられている1).β 2GPI に続いてプロトロンビンも aPL のターゲットであることが判明しており15−17), 陰性荷電リン脂質であるホスファチジルセリンと プロトロンビンの複合体に対する自己抗体を検出 するELISA が樹立され18−20),ホスファチジルセリ ン依存性抗プロトロンビン抗体(phosphatidylserine/ prothrombin complex(aPS/PT))と名付けられ,同抗 体のAPS 症状との強い相関性が示された18, 21).さら に,β2GPI domain I に対する自己抗体が非常に強力 な血栓症との関連を認めることが判明し22),これら を含む新しい分類基準の作成が求められている. 一方,これら多種のaPL をルーチンで検査する ことによって,各症例で認められる多彩なaPL プ ロファイルをどの様に治療応用するのかという点に ついては以前より様々な議論があった.様々な症例 ─コホート研究の結果から中~高力価のaCL IgG が APS 及び非 APS-aPL 陽性患者において独立した血 栓リスク因子であると報告された23, 24).それに加え て,システマティック・レビューの結果から,LAC も血栓症の強力な独立的リスク因子であることが報 告された25).De Groot らは,LAC が陽性でも aβ
2GPI
及びaPS/PT が陰性の場合には,深部静脈血栓症
(DVT)の発症リスクを上昇させないが,LAC と
aβ2GPI の両者が陽性の際には,そのリスクが著し
く上昇すると報告している(odds ratio [OR] = 10.1, 95% confidence interval [CI]: 1.3−79.8)26).他の報告
でも,aβ2GPI は凝固時間の延長(LAC)と相関し
血栓症の強力なリスクとなると報告されていて27),
最近ではその内でもよりspecific な aβ2GPI domain I ではより強力に血栓イベントと相関すると考えられ ている28).さらに,もう一方のnon-criteria aPL であ るaPS/PT についても APS の血栓リスクとの相関を 示すデータが多く報告されている21, 29, 30). こういった各aPL の血栓リスクについての知見 を元に,aPL 陽性患者において血栓リスクを層別化 する試みがなされた.Pengo らは連続する 618 例を 6 年間にわたり観察し aPL プロファイルと血栓イベ ントとの相関を解析した結果,aCL,aβ2GPI,LAC のいずれもが陽性の場合(triple positivity)は,最 も強力な血栓リスクであると報告した(HR = 33.3, 95% CI: 7.0−157.6)31).このtriple positivity は非 APS- aPL 陽性例や32),2 次性 APS(SLE に合併した APS) 患者でも同様に血栓症発症に相関することが判明し た33).一般的に非APS-aPL 陽性者では画一的な血 栓症の1 次予防治療は推奨されないが,triple posi-tivity 症例では血栓リスクが強力であることを認識 しておく必要がある. 古典的血栓リスクとAPS 患者 血栓症は多因子病態であり,aPL 以外にも高血圧, 高脂血症などの古典的血栓リスクがaPL キャリア でどのように血栓症に関与するか検討が進められて きた.それら古典リスクの中では,高血圧はAPS 患者34)や非APS-aPL 陽性者24)で血栓症の独立した リスクと報告されている.Erkan らは 77 例の APS 患者と56 例の非 APS-aPL 陽性者で横断研究を行 い,古典的リスク因子の中で高血圧と喫煙のみが動 脈血栓症のリスク因子として抽出され,静脈血栓症 のリスクとしては有為な相関を認めるリスク因子は なかったと報告した.近年,triple positivity や LAC
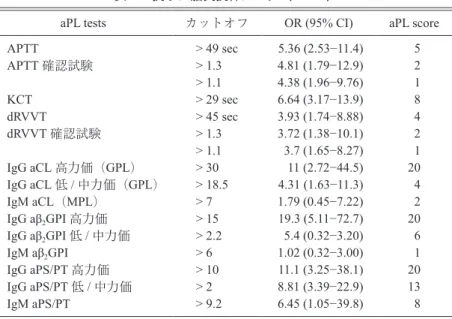
の存在が,喫煙と関連し,かつ喫煙者でLAC 陽性 の際には静脈血栓症の発症と相関すると報告してい る35). APS 血栓症のスコアシステム APS における血栓リスクの層別化を一歩進める形 で,aPL プロファイルが示す血栓リスクを定量的に 評価しようとの試みが進められた.Otomo らは anti-phospholipid score(aPL-S)を提唱した(表 1 )36). これは,aPL プロファイルから APS の血栓症リス クを定量化しようとする最初の試みであったが,適 切なカットオフ値を設定することによって高い相関 性で血栓症の発症リスクを検出することができた. このstudy では 233 例の自己免疫疾患患者の APS 症状とaPL プロファイルを検討した.全症例で下 記全てのaPL が測定された.LAC については,3
種類の凝固検査 (activated partial thromboplastic time [APTT], diluted Russell viper venom time [dRVVT], kaolin clotting time [KCT]) が国際血栓止血学会のガ イドラインを元に施行され,3 種類の中和試験と 2
種類の確認試験が施行された37).aCL(IgG/IgM), aβ2GPI(IgG/IgM),aPS/PT(IgG/IgM) は ELISA で
測定され,過去の各study と同様に,低力価から中
~高力価例を分類するためにsecond cut-off が設定さ れている18, 38, 39).そしてAPS 症状に対する各 aPL 結
果OR が計算され,抗リン脂質抗体スコア(aPL-S)
= 5 × exp ([OR] − 5)/4 として計算された.各種 aPL
検査結果から算出されたaPL-S の合計を症例毎の aPL-S と定義した.aPL-S と血栓症発症リスクとの 関連を検定するために,validation cohort が設定さ れ,62ヶ月間の観察研究の結果,やはり aPL-S 高値 は血栓症リスクと強力に相関することがわかった. 血栓症発症の高リスクはaPL-S ≥ 30 とカットオフが 設定され,新規血栓症発祥のハザード比(HR)は aPL-S of ≥ 10 と ≥ 30 で,それぞれ 2.86(95% CI: 1.33−6.6, P < 0.006)と 5.27(95% CI: 2.32−11.95, P < 0.0001)だった.また,陽性予測値は,aPL-S ≥ 10 と≥ 30 でそれぞれ 20%と 31%で,陰性的中率は, 両者ともに92%だった.さらに,APL ≥ 30 の高リ スク例は39 例(原発性 APS 14 例,2 次性 APS 15 例,他疾患 10 例)で,そのうち 34 例(87%)は抗 血栓療法下での血栓発祥であった.APL-S 値による 血栓症発症リスクの違いを検討したところ,aPL-S ≥ 30 症例では aPL-S 低値例に比べて HR5.40 の高い リスクを認めた(95% CI: 2.38−12.23, P < 0.005). そしてvalidation cohort において,古典的血栓リス ク因子や膠原病において報告されている血栓リスク 因子(グルココルチコイド治療,関節リウマチなど) を含めて単解析し,血栓症との関連が有為なものを 抽出し,多因子Cox 解析したて.その結果 aPL-S ≥ 30 が最も有為な関連リスク因子として抽出された (hazard ratio [HR] = 3.144, 95% CI: 1.383−7.150, P <
0.006).一方,血栓症の既往も独立したリスク因子 と判明したが,他の古典的血栓リスク因子を含め た各種因子は相関を認めなかった.その後,aPL-S は多くの患者コホートでvalidation が行われてい る40−42). 一方,aPL-S のコンセプトに類似して,Sciascia らは,新たなスコアシステムを作成し,Global Anti- Phospholipid Syndrome Score(GAPSS)と名付けた43)
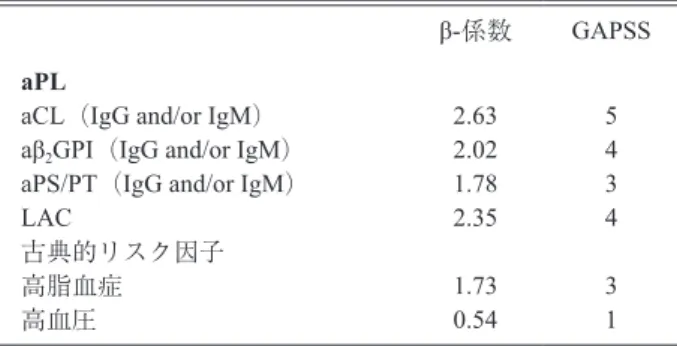
(表2 ).GAPSS は aPL のみでなく,古典的な血栓 リスクを並列してスコアシステムに含め,aPL-S と 同様に,自己免疫疾患患者コホートで,各種aPL と 古典的リスク因子の存在と血栓症発症と高い相関を 持つリスク因子を抽出してスコア化した.GAPSS ではaPL は非常に簡略化されて解析されている. すなわち,aPL-S では各 aPL-S のイムノグロブリン タイプ(IgG/M)や力価の違いによってスコアが設 定されているのだが,GAPSS ではそれらを全て無
視し,例えばaCL であれば高力価の aCL IgG も低
力価のaCL IgM も同様に aCL 陽性として画一的に
血栓リスクを検討するというものである.GAPSS は,aPL-S と同様,血栓症を有する例で,非血栓症 例に比べ有為に高値であった[GAPSS = 9.5 ± 5.6,
表1 抗リン脂質抗体スコア(aPL-S)
aPL tests カットオフ OR (95% CI) aPL score APTT APTT 確認試験 KCT dRVVT dRVVT 確認試験 IgG aCL 高力価(GPL) IgG aCL 低 / 中力価(GPL) IgM aCL(MPL)
IgG aβ2GPI 高力価
IgG aβ2GPI 低 / 中力価
IgM aβ2GPI
IgG aPS/PT 高力価 IgG aPS/PT 低 / 中力価 IgM aPS/PT > 49 sec > 1.3 > 1.1 > 29 sec > 45 sec > 1.3 > 1.1 > 30 > 18.5 > 7 > 15 > 2.2 > 6 > 10 > 2 > 9.2 5.36 (2.53−11.4) 4.81 (1.79−12.9) 4.38 (1.96−9.76) 6.64 (3.17−13.9) 3.93 (1.74−8.88) 3.72 (1.38−10.1) 3.7 (1.65−8.27) 11 (2.72−44.5) 4.31 (1.63−11.3) 1.79 (0.45−7.22) 19.3 (5.11−72.7) 5.4 (0.32−3.20) 1.02 (0.32−3.00) 11.1 (3.25−38.1) 8.81 (3.39−22.9) 6.45 (1.05−39.8) 5 2 1 8 4 2 1 20 4 2 20 6 1 20 13 8 aPL: 抗リン脂質抗体,OR: オッズ比,CI: 信頼区間,APTT: 活性化部分トロンボプラスチン 時間,KCT: カオリン凝固時間,dRVVT: 希釈 Russell 蛇毒時間,aCL: 抗カルジオリピン抗体, GPL: IgG phospholipid units,MPL: IgM phospholipid units,aβ2GPI: 抗 β2-グリコプロテイン I
range: 0−20; and 3.9 ± 4.1, range: 0−17, P < 0.001]. GAPSS はいくつかの施設で validation もされた44, 45). Zuily ら は,137 例 の SLE 患 者 と aPL キ ャ リ ア を 43.1ヶ月に渡ってフォローアップして,16 点以上の GAPSS は血栓症の予測因子として有用(HR = 6.17, 95% CI: 1.70−22.40))だが,各 aPL の陽陰性は血栓 症発症の予測因子となり得ないと報告した44). スコアシステムの実臨床への応用 スコアシステムが示すデータは非常に意義深いが, aPL-S も GAPSS も実臨床での応用は極めて限定的 である.その1 つの原因は,スコアの算出に多くの 検査が必要になることである.特に,現在,分類基 準に含まれていないaPS/PT が両スコアで共に必須 の検査となっている.最近,Amengual らは,国際 抗リン脂質抗体学会のタスクフォースとして,aPS/ PT の APS 分類能を国際多施設検定し,APS 症状と 高度に相関する自己抗体であると報告した46).Zuily らは,前向き多施設研究の結果からaPS/PT IgG は, SLE 患者において血栓イベントの予測因子として すぐれると報告した44).こういった知見の蓄積を元 に,近い将来,aPS/PT 測定の意義が更に認識され, APS 分類基準にもその測定が含まれる公算が高い. そうするとやはり多くのaPL 検査が必要となるが,
modified aPL-S は,aPL-S と比べて少ない検査項目 で同等の血栓予測能を持つように作成されたスコ
アである.著者らは47),自己免疫疾患患者コホート
を用いて検定することで,2 個の凝固検査(aPTT, dRVVT) と 4 種 の ELISA 検 査(IgG tests for aCL, aβ2GPI and aPS/PT and IgM aPS/PT)を行うことでも,
オリジナルのaPL-S と同等の血栓予測因子(血栓リ スク因子)となりうることを報告した.しかし,と りわけ本邦の保険診療や検査室の実情ではこれだけ の検査を行える施設は極めて限定的である.また, 第2 には aPL の標準化がされていない状況ではス コアの一般化は困難ということである.現時点では aPL の各種 ELISA はキット間,あるいは施設間に おいてもデータの標準化が進んでいない48, 49).LAC は更に施設間・試薬間・測定機器間の標準化が難し い50−52).現在,こういった問題を解消すべく日本血 栓止血学会のAPS 部会及び抗リン脂質抗体症候群 ワークショップ(APS-WS: http://aps-ws.com/?page_ id=12)が協働し,aPL 測定系標準化のため,基礎 データを集積している.近年では,複数のaPL を 自動測定する機器が開発され,その正確性(結果の 一致率が高い)が報告されており,今後は施設間に おけるデータの差異を解消する目的にこういった機 器も有効に利用する必要がある53−56).最後に,スコ ア自体の標準化も必要である.aPL-S, GAPSS 双方 とも単一施設の患者コホートデータから樹立したも のである.理想的には標準化されたaPL 測定系を 用いて測定した多施設患者のコホートデータをスコ ア化すべきである.また,両スコアは共に自己免疫 疾患患者コホートを用いて作成されたスコアシステ ムであることにも注意が必要であり,非自己免疫疾 患患者の血栓症リスクを検定する際にはカットオフ 値が異なる可能性がある.実際,GAPSS のカット オフは自己免疫疾患の中でもSLE と非 SLE では大 きく異なることが報告されており,aPL-S でもその 傾向はある.これはSLE では非 APS-aPL 陽性例が 多いからであり,カットオフの設定には基礎疾患に 留意しなくてはいけない44, 45). GAPSS と aPL-S のどちらが優れるのかというの も興味ある点である.GAPSS は比較的簡便にスコ アを算出できる点がaPL-S にすぐれる(aPL 測定検 査が少なく済む)が,一方,スコアシステムの本来 の特徴や目的である血栓予測能もしくは血栓リスク の定量化という点ではaPL-S に劣る.血栓症は確か にaPL のみでなく古典的リスク因子など複数のリ スク因子の蓄積で発症するが,前述の通り,aPL-S 高値は血栓症の既往と並んで抽出される強力な血栓 リスク因子であり,他の一般的な血栓リスク因子と 比較してその血栓イベントへの関与は大きい.即ち aPL 陽性例では,一度は注意深く aPL プロファイル を検討し血栓リスクを予測することで将来の血栓リ スクを把握できる可能性が高い.modified aPL-S は より少ない検査数でaPL-S 並みの血栓予測能を有 し,GAPSS より優れることも知られている57).た
表2 Global Anti-Phospholipid Syndrome Score (GAPSS) β-係数 GAPSS aPL
aCL(IgG and/or IgM) aβ2GPI(IgG and/or IgM)
aPS/PT(IgG and/or IgM) LAC 古典的リスク因子 高脂血症 高血圧 2.63 2.02 1.78 2.35 1.73 0.54 5 4 3 4 3 1 aPL: 抗リン脂質抗体,aCL: 抗カルジオリピン抗体,aβ2GPI: 抗 β2
グリコプロテインI 抗体,aPS/PT: ホスファチジルセリン依存性抗 プロトロンビン抗体,LAC: ループスアンチコアグラント
だし,こういったデータは標準化されたaPL 測定 系を用いて多施設検討によって再検すべきと考えら れる.スコアシステムの意義はむしろaPL 測定の 持つ意味を変えたことであり,それまで定性的な測 定系(APS の診断目的に測定し,aPL はどれか 1 項 目でも陽性であればいい)であったaPL 測定が, 血栓症のリスクを算定できる定量的検査として捉え られるようになった. 結 論
aPL-S と GAPSS の双方が APS もしくは非 APS-aPL 陽性例における血栓症リスクを高い確度で検出 できるが,これらが実用化されるにはaPL 測定系 の標準化などいくつかの改善が必要である.一方, スコアの概念は重要で,aPL プロファイルは血栓 症リスクを示すため,APS を疑う症例では一度は aPS/PT も含めた網羅的な解析をするのが有用と考 えられる. 文 献
1) Miyakis, S., et al.: International consensus state-ment on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. 4: 295−306, 2006.
2) Bohgaki, M., et al.: The p38 mitogen-activated pro-tein kinase (MAPK) pathway mediates induction of the tissue factor gene in monocytes stimulated with human monoclonal anti-beta2Glycoprotein I antibodies. Int Immunol. 16: 1633−1641, 2004. 3) Oku, K., et al.: Essential role of the p38 mitogen-
activated protein kinase pathway in tissue factor gene expression mediated by the phosphatidylser-ine-dependent antiprothrombin antibody. Rheuma-tology (Oxford). 52: 1775−1784, 2013.
4) Long, A.A., et al.: The relationship of antiphos-pholipid antibodies to thromboembolic disease in systemic lupus erythematosus: a cross-sectional study. Thromb Haemost. 66: 520−524, 1991. 5) Mok, C.C., et al.: Incidence and risk factors of
thromboembolism in systemic lupus erythemato-sus: a comparison of three ethnic groups. Arthritis Rheum. 52: 2774−2782, 2005.
6) Vianna, J.L., et al.: Comparison of the primary and secondary antiphospholipid syndrome: a European Multicenter Study of 114 patients. Am J Med. 96: 3−9, 1994.
7) Derksen, R.H., et al.: Patients with antiphospho-lipid antibodies and venous thrombosis should
receive long term anticoagulant treatment. Ann Rheum Dis. 52: 689−692, 1993.
8) Ambrozic, A., et al.: Anti-beta(2)-glycoprotein I antibodies in children with atopic dermatitis. Int Immunol. 14: 823−830, 2002.
9) Giron-Gonzalez, J.A., et al.: Antiphospholipid syndrome and asymptomatic carriers of antiphos-pholipid antibody: prospective analysis of 404 individuals. J Rheumatol. 31: 1560−1567, 2004. 10) Pengo, V., et al.: Survey of lupus anticoagulant
diagnosis by central evaluation of positive plasma samples. J Thromb Haemost. 5: 925−930, 2007. 11) Lim, W., et al.: Management of antiphospholipid
antibody syndrome: a systematic review. JAMA. 295: 1050−1057, 2006.
12) Tektonidou, M.G., et al.: Risk factors for thrombo-sis and primary thrombothrombo-sis prevention in patients with systemic lupus erythematosus with or without antiphospholipid antibodies. Arthritis Rheum. 61: 29−36, 2009.
13) Ruiz-Irastorza, G., et al.: High impact of antiphos-pholipid syndrome on irreversible organ damage and survival of patients with systemic lupus ery-thematosus. Arch Intern Med. 164: 77−82, 2004. 14) Zuily, S., et al.: Impairment of quality of life in
patients with antiphospholipid syndrome. Lupus. 24: 1161−1168, 2015.
15) Fleck, R.A., et al.: Anti-prothrombin antibodies and the lupus anticoagulant. Blood. 72: 512−519, 1988.
16) Bevers, E.M., et al.: Lupus anticoagulant IgG’s (LA) are not directed to phospholipids only, but to a complex of lipid-bound human prothrombin. Thromb Haemost. 66: 629−632, 1991.
17) Oosting, J.D., et al.: Antiphospholipid antibodies directed against a combination of phospholipids with prothrombin, protein C, or protein S: an ex-planation for their pathogenic mechanism? Blood. 81: 2618−2625, 1993.
18) Atsumi, T., et al.: Association of autoantibodies against the phosphatidylserine-prothrombin com-plex with manifestations of the antiphospholipid syndrome and with the presence of lupus anticoag-ulant. Arthritis Rheum. 43: 1982−1993, 2000. 19) Matsuda, J., et al.: Phosphatidyl serine-dependent
antiprothrombin antibody is exclusive to patients with lupus anticoagulant. Br J Rheumatol. 35: 589− 591, 1996.
20) Galli, M., et al.: Different anticoagulant and immu-nological properties of anti-prothrombin antibodies in patients with antiphospholipid antibodies.
Thromb Haemost. 77: 486−491, 1997.
21) Oku, K., et al.: Antiprothrombin antibody test-ing: detection and clinical utility. Semin Thromb Hemost. 34: 335−339, 2008.
22) de Laat, B., et al.: The association between circu-lating antibodies against domain I of beta2-glyco-protein I and thrombosis: an international multi-center study. J Thromb Haemost. 7: 1767−1773, 2009.
23) Finazzi, G., et al.: Natural history and risk factors for thrombosis in 360 patients with antiphospholip-id antibodies: a four-year prospective study from the Italian Registry. Am J Med. 100: 530−536, 1996.
24) Ruffatti, A., et al.: Risk factors for a first throm-botic event in antiphospholipid antibody carriers. A multicentre, retrospective follow-up study. Ann Rheum Dis. 68: 397−399, 2009.
25) Galli, M., et al.: Lupus anticoagulants are stronger risk factors for thrombosis than anticardiolipin antibodies in the antiphospholipid syndrome: a systematic review of the literature. Blood. 101: 1827−1832, 2003.
26) de Groot, P.G., et al.: Lupus anticoagulants and the risk of a first episode of deep venous thrombosis. J Thromb Haemost. 3: 1993−1997, 2005.
27) De Laat, B., et al.: An international multicentre- laboratory evaluation of a new assay to detect specifically lupus anticoagulants dependent on the presence of anti-beta2-glycoprotein autoantibodies. J Thromb Haemost. 9: 149−153, 2011.
28) De Craemer, A.S., et al.: Role of anti-domain 1-beta2 glycoprotein I antibodies in the diagnosis and risk stratification of antiphospholipid syn-drome. J Thromb Haemost. 14: 1779−1787, 2016. 29) Sciascia, S., Bertolaccini, M.L.: Antibodies to
phosphatidylserine/prothrombin complex and the antiphospholipid syndrome. Lupus. 23: 1309−1312, 2014.
30) Heikal, N.M., et al.: Laboratory evaluation of anti-phospholipid syndrome: a preliminary pro-spective study of phosphatidylserine/prothrombin antibodies in an at-risk patient cohort. Clin Exp Immunol. 180: 218−226, 2015.
31) Pengo, V., et al.: Antibody profiles for the diagno-sis of antiphospholipid syndrome. Thromb Hae-most. 93: 1147−1152, 2005.
32) Becarevic, M., et al.: The IgM isotype of anti- annexin A5 antibodies and multiple positivity of conventional antiphospholipid antibodies: increas-ing the number of clinical manifestations of
pri-mary antiphospholipid syndrome. Clin Rheumatol. 35: 1361−1365, 2016.
33) Sciascia, S., et al.: Clinical accuracy for diagnosis of antiphospholipid syndrome in systemic lupus erythematosus: evaluation of 23 possible combina-tions of antiphospholipid antibody specificities. J Thromb Haemost. 10: 2512−2518, 2012.
34) Saraiva Sda, S., et al.: Recurrent thrombosis in antiphospholipid syndrome may be associated with cardiovascular risk factors and inflammatory response. Thromb Res. 136: 1174−1178, 2015. 35) Gustafsson, J.T., et al.: Cigarette smoking,
anti-phospholipid antibodies and vascular events in Systemic Lupus Erythematosus. Ann Rheum Dis. 74: 1537−1543, 2015.
36) Otomo, K., et al.: Efficacy of the antiphospho-lipid score for the diagnosis of antiphosphoantiphospho-lipid syndrome and its predictive value for thrombotic events. Arthritis and Rheumatism. 64: 504−512, 2012.
37) Brandt, J.T., et al.: Criteria for the diagnosis of lupus anticoagulants: an update. On behalf of the Subcommittee on Lupus Anticoagulant/Antiphos-pholipid Antibody of the Scientific and Standard-isation Committee of the ISTH. Thrombosis and Haemostasis. 74: 1185−1190, 1995.
38) Amengual, O., et al.: Specificity of ELISA for antibody to beta 2-glycoprotein I in patients with antiphospholipid syndrome. British Journal of Rheumatology. 35: 1239−1243, 1996.
39) Harris, E.N., et al.: Evaluation of the anti-cardio-lipin antibody test: report of an international work-shop held 4 April 1986. Clinical and Experimental Immunology. 68: 215−222, 1987.
40) Sciascia, S., et al.: Independent validation of the antiphospholipid score for the diagnosis of anti-phospholipid syndrome. Ann Rheum Dis. 72: 142− 143, 2013.
41) Sciascia, S., et al.: Thrombotic risk assessment in systemic lupus erythematosus: validation of the global antiphospholipid syndrome score in a pro-spective cohort. Arthritis Care Res (Hoboken). 66: 1915−1920, 2014.
42) Chen, J., et al.: Elevated partial antiphospholipid score is a strong risk factor for thrombosis in patients with systemic lupus erythematosus: a vali-dation study. Clin Rheumatol. 35: 333−340, 2016. 43) Sciascia, S., et al.: GAPSS: the Global Anti-
Phospholipid Syndrome Score. Rheumatology (Oxford). 52: 1397−1403, 2013.
44) Zuily, S., et al.: Validity of the global anti- phospholipid syndrome score to predict thrombo-sis: a prospective multicentre cohort study. Rheu-matology (Oxford). 54: 2071−2075, 2015.
45) Oku, K., et al.: An independent validation of the Global Anti-Phospholipid Syndrome Score in a Japanese cohort of patients with autoimmune dis-eases. Lupus. 24: 774−775, 2015.
46) Amengual, O., et al.: Evaluation of phosphatidyl-serine-dependent antiprothrombin antibody testing for the diagnosis of antiphospholipid syndrome: results of an international multicentre study. Lupus. 2016.
47) Oku, K., et al.: Antiphospholipid scoring: signifi-cance in diagnosis and prognosis. Lupus. 23: 1269− 1272, 2014.
48) Devreese, K.M.: Standardization of antiphospho-lipid antibody assays. Where do we stand? Lupus. 21: 718−721, 2012.
49) Willis, R., et al.: Standardization of antiphospho-lipid antibody testing–historical perspectives and ongoing initiatives. Semin Thromb Hemost. 40: 172−177, 2014.
50) Devreese, K.M.: Antiphospholipid antibody testing and standardization. Int J Lab Hematol. 36: 352− 363, 2014.
51) Chantarangkul, V., et al.: Laboratory diagnostic outcome applying detection criteria recommended by the Scientific and Standardization Committee of the ISTH on Lupus Anticoagulant. Thromb Hae-most. 110: 46−52, 2013.
52) Pengo, V., et al.: Interpretation of laboratory data and need for reference laboratories. Lupus. 21: 732−733, 2012.
53) Urbanus, R.T., de Groot, P.G.: Antiphospholipid antibodies–we are not quite there yet. Blood Rev. 25: 97−106, 2011.
54) Reber, G., et al., European Forum on Antiphospho-lipid Antibodies Standardization G: Variability of anti-beta2 glycoprotein I antibodies measurement by commercial assays. Thromb Haemost. 94: 665− 672, 2005.
55) P DEM, et al.: Analytical and clinical performance of a new, automated assay panel for the diagnosis of antiphospholipid syndrome. J Thromb Haemost. 8: 1540−1546, 2010.
56) Oku, K., et al.: Significance of fully automated tests for the diagnosis of antiphospholipid syn-drome. Thromb Res. 146: 1−6, 2016.
57) Oku, K., et al.: Markers of Thrombotic Events in Autoimmune Diseases: Comparison of Antiphos-pholipid Score (aPL-S) and Global Anti-Phospho-lipid Syndrome Score (GAPSS). Arthritis Rheuma-tol. 66: S1251, 2014.