HIV 感染者における慢性腎臓病の有病率に関する研究
1)
東京都立駒込病院感染症科,
2)同 腎臓内科
柳澤 如樹
1)安藤 稔
2)菅沼 明彦
1)今村 顕史
1)味澤 篤
1)(平成 21 年 6 月 22 日受付)
(平成 21 年 9 月 15 日受理)
Key words : HIV, chronic kidney disease, proteinuria, hematuria, cystatin C
要 旨
背景:Human immunodeficiency virus(HIV)感染者の長期生存に伴って,慢性期の合併症が問題となっ ている.その中でも慢性腎臓病(chronic kidney disease : CKD)は重要な合併症として注目されているが,
本邦における臨床像に関する研究は少ない.方法:2009 年 2 月〜4 月までの 3 カ月間に,東京都立駒込病院 感染症科に定期通院した HIV 感染者 788 例(男性 706 例,女性 82 例)を対象にして,検尿異常と腎機能に ついて横断的解析を行った.対象者の平均年齢は 46.2 11.8 歳であった.HIV 感染者における CKD 有病率 および腎機能の低下した患者の頻度を調査するために,血清クレアチニンおよび血清シスタチン C を測定 し,検尿で尿蛋白および尿潜血を測定した.推定糸球体濾過値(estimated glomerular filtration rate : eGFR)
の推算式は日本腎臓学会 CKD 対策委員会プロジェクトが決定した最新 GFR 推算式を用いた.CKD の分類 は,米国腎臓財団の定めた stage 分類を適用した.結果:CKD の有病率は 14.9% であった.内訳は,CKD stage 1 が 15 例(1.9%),stage 2 が 28 例(3.6%),stage 3 が 66 例(8.4%),stage 4 が 1 例(0.1%),stage 5 が 1 例(0.1%),stage 5D が 6 例(0.8%)であった.血清シスタチン C 値による腎機能低下例は 182 例
(23.3%)に認められた.CKD stage 3 以上は 74 例(9.4%)で,高血圧,糖尿病の合併がそれぞれ 55.4%,27.0%
で認められた.尿蛋白は 71 例(9.1%),尿潜血は 44 例(5.6%)で認められた.結論:当院外来通院中の HIV 感染者における検尿異常と CKD の有病率を明らかにした.約 10〜20% に腎機能低下が認められ,高血圧 や糖尿病との関連性も示唆された.
〔感染症誌 84:28〜32,2010〕
緒 言
Human immunodeficiency virus(HIV)感染者の 生命予後は,多剤併用療法(highly active antiretrovi- ral therapy : HAART)の登場で劇的に改善したが
1)2), 一方で長期生存者における慢性期の合併症が新たな問 題 と し て 出 現 し て き た.そ の 中 で も,慢 性 腎 臓 病
(chronic kidney disease : CKD)は,重要な合併症と して注目されている
3).HIV 感染者における CKD の 原因として,HAART および日和見感染症治療薬等 に関連した一部の薬剤が有する腎毒性や,合併する糖 尿病や高脂血症などの代謝異常,および HIV 感染者 の高齢化などがあげられる.主に米国では CKD の増 加を反映して,透析治療が必要な末期腎不全(end- stage renal disease : ESRD)に至った HIV 感染者が
増加していることが報告されている
4)〜6).
本邦は,先進国でありながらも新規の HIV 感染者 が増加している状況にあるが,HIV 感染者における 検尿異常と CKD 有病率に関するデータは,我々が以 前に報告した論文以外にはない
7).しかし以前の報告 では,尿検査のデータが不十分であったことと推定糸 球体濾過値(estimated glomerular filtration rate : eGFR)の推算式として日本腎臓学会 CKD 対策委員 会プロジェクトが決定した最新 GFR 推算式
8)を用い ていなかったことに欠点があった.
今回我々は,本邦の HIV 感染者における最新の検 尿異常と CKD 有病率を調査するため,最新の日本人 eGFR 推算式を用いて,患者年齢別に CKD ステージ 分類を行うとともに,調査対象者全例に尿検査を施行 した.加えて,筋肉量や肝機能障害の有無に影響され ず,HIV 感染者における早期腎障害の指標として有
原 著別刷請求先:(〒113―8677)東京都文京区本駒込 3―18―22
東京都立駒込病院感染症科 柳澤 如樹
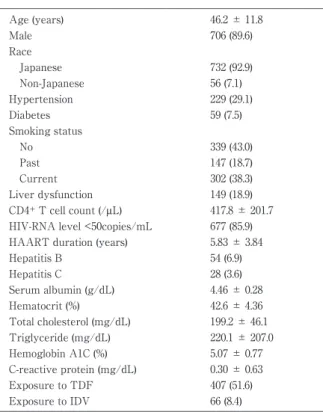
Tabl e 1 Demogr aphi c s and l abor at or y f i ndi ngs at bas e- l i ne
46. 2 ± 11. 8 Age ( year s )
706 ( 89. 6) Mal e
Rac e
732 ( 92. 9) J apanes e
56 ( 7. 1) Non- J apanes e
229 ( 29. 1) Hyper t ens i on
59 ( 7. 5) Di abet es
Smoki ng s t at us
339 ( 43. 0) No
147 ( 18. 7) Pas t
302 ( 38. 3) Cur r ent
149 ( 18. 9) Li ver dys f unc t i on
417. 8 ± 201. 7 CD4
+T c el l c ount ( / μ L)
677 ( 85. 9) HI V- RNA l evel <50c opi es /mL
5. 83 ± 3. 84 HAART dur at i on ( year s )
54 ( 6. 9) Hepat i t i s B
28 ( 3. 6) Hepat i t i s C
4. 46 ± 0. 28 Ser um al bumi n ( g/dL)
42. 6 ± 4. 36 Hemat oc r i t ( %)
199. 2 ± 46. 1 Tot al c hol es t er ol ( mg/dL)
220. 1 ± 207. 0 Tr i gl yc er i de ( mg/dL)
5. 07 ± 0. 77 Hemogl obi n A1C ( %)
0. 30 ± 0. 63 C- r eac t i ve pr ot ei n ( mg/dL)
407 ( 51. 6) Expos ur e t o TDF
66 ( 8. 4) Expos ur e t o I DV
Val ues expr es s ed as mean±SD or number ( per c ent age) . Hyper - t ens i on was def i ned as s ys t ol i c bl ood pr es s ur e > 140mmHg
_and/or di as t ol i c bl ood pr es s ur e > 90mmHg
_or t aki ng ant i hyper - t ens i ve agent s at bas el i ne. Di abet es was def i ned as di agnos i s of di abet es mel l i t us pr i or t o bas el i ne, or t aki ng or al ant i di abet i c agent s or i ns ul i n at bas el i ne. Li ver dys f unc t i on was def i ned as ei - t her as par t at e ami not r ans f er as e ( AST) > 33
_I U/L or al ani ne ami - not r ans f er as e ( ALT) > 44
_I U/L. Abbr evi at i ons : HAART, hi ghl y ac t i ve ant i r et r ovi r al t her apy; TDF, t enof ovi r di s opr oxi l f u- mar at e; I DV, i ndi navi r .
用であることが報告されている血清シスタチン C 値 についても検討を加えた
9)10).
対象と方法
2009 年 2 月から 4 月までの 3 カ月間に,東京都立 駒込病院感染症科に定期通院した HIV 感染者 788 例 を対象とした横断的解析を行った.内訳は男性 706 例,
女性 82 例で,平均年齢は 46.2 11.8 歳(範囲:18〜82 歳)であった.
HIV 感染者における CKD 有病率および腎臓障害の 有無を調査するために,採血で血清クレアチニンおよ び血清シスタチン C を測定し,検尿で尿蛋白および 尿潜血の有無を検査した.
血清クレアチニンの測定には酵素法(イアトロ LQ CRE(A)II,三菱化学メディエンス,東京)を,血 清シスタチンの測定にはラテックス免疫比濁法(イア トロ Cys-C,三菱化学メディエンス)を用いた.尿蛋 白はエームス尿検査試験紙を用いて 1+以上を,尿潜 血は 3〜5! high power field 以上を陽性とした.腎機 能 は GFR 推 算 式:eGFR(mL ! min ! 1.73m
2)=194×
Serum creatinine
−1.094×Age
−0.287×0.739(if female)に
て計算した
8).CKD は eGFR 60 mL! min! 1.73m
2未 満,もしくは尿蛋白陽性が 3 カ月以上継続するものと 定義し,分類は米国腎臓財団の定めた stage 分類を適 用した
11).血清シスタチン C は当院の臨床検査科が定 めた 0.9mg! L を上限とし,血清シスタチン C"0.9mg
! L を腎機能低下と定義した.
高血圧は,収縮期血圧"140mmHg または拡張期血 圧"90mmHg,もしくは降圧剤(アンギオテンシン 変換酵素阻害薬,アンギオテンシン II 受容体拮抗薬,
カルシウム拮抗薬)の使用と定義した.糖尿病は,こ れまでに糖尿病と診断されていること,もしくは血糖 降下薬やインスリンの使用のあることと定義した.肝 機能障害は,aspartate aminotransferase(AST) "33 IU! L,または alanine aminotransferase(ALT)"44 IU ! L と定義した.
本研究は当院倫理委員会の承認を得たものである.
結 果
対象者となった 788 例の概要を Table 1に示した.
対象患者の 732 例(92.9%)が日本人であった.高血 圧は 229 例(29.1%),糖尿病は 59 例(7.5%)で認め られた.CD4 陽性リンパ球数は 417.8 201.7! µL,HIV- RNA 量 50copies! mL 未 満 は 677 例(85.9%)で あ っ た.HAART の 使 用 期 間 は,5.83 3.84 年 で あ っ た.
HAART が使用されていた 716 例(90.9%)のうち,ten- ofovir disoproxil fumarate(TDF)の内服歴は 407 例
(うち 353 例が現在内服中),indinavir(IDV)の内服 歴は 66 例(現在内服例なし)であった.
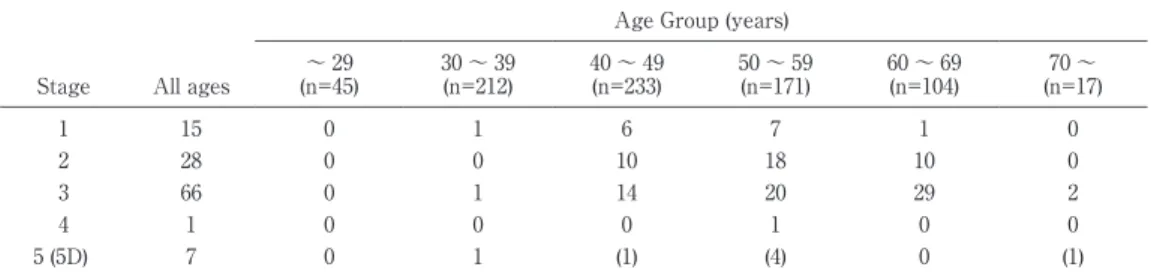
年齢別 CKD の有病率の結果を Table 2に示した.
CKD は全部で 117 例(14.9%)認められた.内訳は,
CKD stage 1が 15 例(1.9%),stage 2が 28 例(3.6%),
stage 3が 66 例(8.4%),stage 4が 1 例(0.1%),stage 5が 1 例(0.1%),stage 5Dが 6 例(0.8%)であった.
したがって,CKD stage 3以上は 74 例(9.4%;74! 788 例)であっ た.CKD stage 3以 上 の 患 者 で は,41 例
(55.4%)が高血圧を,20 例(27.0%)が糖尿病を合 併していた(Fig. 1).一方,高血圧と糖尿病のいず れも合併していない患者は全部で 531 例(67.4%)認 められたが,その中でCKD stage 3以上は26例(4.9%;
26! 531 例)であった.
Fig. 2に尿蛋白と尿潜血陽性例の結果を示した.こ の解析は,既に血液透析が導入されている(stage 5D)
6 例 を 除 く 782 例 で 行 っ た.尿 蛋 白 陽 性 は 71 例
(9.1%),尿潜血陽性は 44 例(5.6%)であった.その うち,両者陽性例が 16 例(2.0%)で認められた.同 様に,腎機能低下(血清シスタチン C"0.9mg! L)は 182 例(23.3%)に認められた.
考 察
本研究は,単一医療機関における HIV 感染者の検
Fi g. 1 Pr eval enc e of hyper t ens i on and di abet es among HI V- i nf ec t ed pat i ent s wi t h CKD > s
_t age 3.
Hyper t ens i on and di abet es wer e f ound i n 41 pat i ent s ( 55. 4%) and 20 pat i ent s ( 27. 0%) among pat i ent s wi t h CKD
>
_s t age 3, r es pec t i vel y.
Fi g. 2 The number of HI V- i nf ec t ed pat i ent s wi t h pr ot ei nur i a and hemat ur i a.
Of 782 HI V- i nf ec t ed pat i ent s wi t h ur i nal ys i s , 71 pat i ent s ( 9. 1%) had pr ot ei nur i a, and 44 pat i ent s ( 5. 6%) had hemat ur i a. Pr ot ei nur i a was def i ned as > 1+
_on ur i ne di p- s t i c k exam i n at l eas t 2 c ons ec ut i ve ur i ne anal ys es . Hema- t ur i a was def i ned as r ed bl ood c el l s > 3-
_5/hi gh power f i el d i n ur i ne anal ys i s .
Number of Patients
Tabl e 2 Pr eval enc e of CKD s t ages i n 788 HI V- i nf ec t ed pat i ent s
Age Gr oup ( year s )
70~
60~ 69 50~ 59
40~ 49 30~ 39
~ 29
( n=17) ( n=104)
( n=171) ( n=233)
( n=212) ( n=45)
Al l ages St age
0 1
7 6
1 0
15 1
0 10
18 10
0 0
28 2
2 29
20 14
1 0
66 3
0 0
1 0
0 0
1 4
( 1) 0
( 4) ( 1)
1 0
7 5 ( 5D)
Cl as s i f i c at i on of CKD s t ages was bas ed on t he Nat i onal Ki dney Foundat i on’ s gui del i nes . CKD was f ound i n 117 pa- t i ent s ( 14. 9%) , and 74 pat i ent s ( 9. 4%) had CKD > s
_t age 3. CKD s t age 5D: s t age r equi r i ng c hr oni c di al ys i s t r eat ment . Abbr evi at i ons : CKD, c hr oni c ki dney di s eas e; HI V, human i mmunodef i c i enc y vi r us .
尿異常と CKD の有病率を提示したものである.CKD の有病率は 14.9% であり,その中でも CKD stage 3
以上の有病率は 9.4% であった.我々は以前,stage 3 以上の有病率を 16.7% と報告したが,この結果は 2007 年に日本腎臓学会から発表された改訂 MDRD 式を用 いたため,今回と異なる結果が出たものと考えられ る
12).本邦以外の HIV 感染者の CKD 3 以上の有病率 に関しては,米国で 2.4〜9.7%,中国(香港)で 5.6%
と報告されており,今回の我々の結果と類似してい た
6)9)13)14).
本コホートにおける尿蛋白陽性率は 9.1% であった が,米国では 14.1〜32% と報告されており,低い傾 向が認められた
15)〜17).同様に,血清シスタチン C"0.9 mg! L で定義された腎機能低下例は 23.3% に認められ が,米国の報告では血清シスタチン C " 1.0mg ! L と定 義されているのにも関わらず,31〜42% であった
9)10). 血清シスタチン C は,非糖鎖性のアミノ酸 120 残基 からなる分子量 13.36kD の一本鎖ポリペプチドで,筋 肉量や肝機能障害の有無に影響されず,HIV 感染者 における早期腎障害の指標として血清クレアチニンよ りも有用であることが報告されている
9)10).しかし,血 清シスタチン C は GFR 以外にも,炎症や HIV-RNA 増幅にも影響されて上昇する可能性があると報告され ている
18)19).今 回 対 象 と し た 788 例 で は,HIV-RNA 量 50copies ! mL 以上は 111 例(14.1%),CRP の軽度 上 昇 例(0.4mg! dL 以 上)は 150 例(19.0%)で 認 め られていたが,今回の結果と米国での血清シスタチン C 値の相違にはこれらの比率の違いが関係している可 能性は否定できない.また,尿蛋白陽性率や腎機能低 下例の違いに関しては,調査対象とされている患者の 人種差や,高血圧や糖尿病などの腎機能に影響を与え る基礎疾患の有病率,検査法や試薬の違いなどが影響 していると考えられる.こうした要因が今回の結果と これまでの海外での報告例との相違に関係しているの であろう.
HIV 感染者における CKD 関連因子として,一般的
に知られている加齢,糖尿病,高血圧以外にもアフリ
カ系アメリカ人,CD4 陽性リンパ球数低値,TDF や
IDV の使用などが報告されている
6)13).IDV はその腎
毒性から,現在臨床現場で使用される頻度は激減して おり,本研究でも 66 例で過去に使用歴を認めたが,現 在も使用している例はなかった.しかし TDF は,現 在の HIV 治療ガイドラインで最も推奨される薬剤の 一つであり,かつ HAART は長期間内服を継続する 必要があるため,その腎毒性に関しては注意する必要 がある
20).しかし,今回の研究で末期腎不全に至った 7 例はいずれも TDF の使用歴はなく,IDV の使用歴 はわずか 1 例に留まった.多発性嚢胞腎が原因で末期 腎不全に至った 1 例を除く 6 例では,全例で高血圧,4 例で糖尿病が基礎疾患として存在し,同疾病の合併が 末期腎不全に至った要因の一つと考えられた.今後,
透析療法に至るリスクが高い CKD stage 3 以上は 74 例(既に stage 5D に至った 6 例も含む)認められた が,そのうち高血圧は 55.4%,糖尿病 27.0% 存在し ており,腎保護の観点から,HAART 薬剤選択に注 意するのみではなく,早期から高血圧や糖尿病のコン トロールにも重点を置く必要がある.
結 論
今回の調査では,HIV 感染者の 14.9% が CKD であ り,その中でも CKD stage 3 以上は 9.4% であった.
尿蛋白陽性率は 9.1%,尿潜血陽性率は 5.6% であっ た.腎機能低下(血清シスタチン C"0.9mg! L)は 182 例(23.3%)に認められた.
謝辞:本研究をまとめるに際し,データの収集,整理に おいて多大なご協力を頂いた東京医科大学臨床検査医学講 座村松崇先生,東京都立駒込病院感染症科関谷紀貴先生に 深謝致します.
文 献
1
)Mocroft A, Ledergerber B, Katlama C, Kirk O, Reiss P, dʼArminio Monforte A, et al.:Decline in the AIDS and death rates in the EuroSIDA study : an observational study. Lancet 2003;
362:22―9.
2
)Lohse N, Hansen AB, Pedersen G, Kronborg G, Gerstoft J, Sorensen HT, et al.:Survival of per- sons with and without HIV infection in Den- mark, 1995-2005. Ann Intern Med 2007;146:
87―95.
3
)Gupta SK, Eustace JA, Winston JA, Boydstun II, Ahuja TS, Rodriguez RA, et al.:Guidelines for the management of chronic kidney disease in HIV-infected patients : recommendations of the HIV Medicine Association of the Infectious Dis- eases Society of America. Clin Infect Dis 2005;
40:1559―85.
4
)Eggers PW, Kimmel PL:Is there an epidemic of HIV Infection in the US ESRD program? J Am Soc Nephrol 2004;15:2477―85.
5
)Vigneau C, Guiard-Schmid JB, Tourret J, Fla- hault A, Rozenbaum W, Pialoux G, et al.:The clinical characteristics of HIV-infected patients
receiving dialysis in France between 1997 and 2002. Kidney Int 2005;67:1509―14.
6
)Fernando SK, Finkelstein FO, Moore BA, Weissman S:Prevalence of chronic kidney dis- ease in an urban HIV infected population. Am J Med Sci 2008;335:89―94.
7
)Nakamura Y, Shibuya A, Suzuki H, Ando M:
Prevalence of chronic kidney disease (CKD) and significant contributors to CKD in HIV-infected patients. Nippon Jinzo Gakkai Shi 2008;50:
499―505.
8
)Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al.:Revised equations for esti- mated GFR from serum creatinine in Japan. Am J Kidney Dis 2009;53:982―92.
9
)Jones CY, Jones CA, Wilson IB, Knox TA, Levey AS, Spiegelman D, et al.:Cystatin C and creatinine in an HIV cohort : the nutrition for healthy living study. Am J Kidney Dis 2008;
51:914―24.
10
)Odden MC, Scherzer R, Bacchetti P, Szczech LA, Sidney S, Grunfeld C, et al.:Cystatin C level as a marker of kidney function in human immunodeficiency virus infection : the FRAM study. Arch Intern Med 2007;167:2213―9.
11
)K! DOQI clinical practice guidelines for chronic kidney disease:evaluation, classification, and stratification. Am J Kidney Dis 2002;39:S1―
266.
12
)Imai E, Horio M, Nitta K, Yamagata K, Iseki K, Tsukamoto Y, et al.:Modification of the Modifi- cation of Diet in Renal Disease (MDRD) Study equation for Japan. Am J Kidney Dis 2007;
50:927―37.
13
)Mocroft A, Kirk O, Gatell J, Reiss P, Gargalianos P, Zilmer K, et al.:Chronic renal failure among HIV-1-infected patients. AIDS 2007;21:1119―
27.
14
)Cheung CY, Wong KM, Lee MP, Liu YL, Kwok H, Chung R, et al.:Prevalence of chronic kidney disease in Chinese HIV-infected patients. Neph- rol Dial Transplant 2007;22:3186―90.
15
)Gupta SK, Mamlin BW, Johnson CS, Dollins MD, Topf JM, Dube MP:Prevalence of proteinuria and the development of chronic kidney disease in HIV-infected patients. Clin Nephrol 2004;
61:1―6.
16
)Szczech LA, Gange SJ, van der Horst C, Bartlett JA, Young M, Cohen MH, et al.:Predic- tors of proteinuria and renal failure among women with HIV infection. Kidney Int 2002;
61:195―202.
17
)Szczech LA, Hoover DR, Feldman JG, Cohen
MH, Gange SJ, Gooze L, et al.:Association be-
tween renal disease and outcomes among HIV-
infected women receiving or not receiving an-
tiretroviral therapy. Clin Infect Dis 2004;39:
1199―206.
18
)Mauss S, Berger F, Kuschak D, Henke J, He- gener P, Wolf E, et al.:Cystatin C as a marker of renal function is affected by HIV replication leading to an underestimation of kidney func- tion in HIV patients. Antivir Ther 2008;13:
1091―5.
19
)Knight EL, Verhave JC, Spiegelman D, Hillege HL, de Zeeuw D, Curhan GC, et al.:Factors in-
fluencing serum cystatin C levels other than re- nal function and the impact on renal function measurement. Kidney Int 2004;65:1416―21.
20
)Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents (No- vember 3, 2008). The DHHS Panel on An- tiretroviral Guidelines for Adults and Adoles- cents-A working Group of the Office of AIDS Research Advisory Council.
Prevalence of Kidney Disease in HIV-infected Patients in Japan
―A Single Center Study
Naoki YANAGISAWA
1), Minoru ANDO
2), Akihiko SUGANUMA
1), Akifumi IMAMURA
1)& Atsushi AJISAWA
1)1)