O r i g i n a l lJTOK 川 山edUniv1 8 5 ()6 202~207 )5102(
Age
and
e
s
d
o
-
h
g
i
H
O
r
a
l
d
i
o
c
i
r
t
o
c
o
c
u
l
G
Therapy
e
s
a
r
e
c
n
I
e
h
t
e
v
i
t
a
l
e
R
Risk
f
o
C
y
t
o
m
e
g
a
l
o
v
i
r
u
s
Antigenemia
P
n
i
s
t
n
e
i
t
a
h
t
i
w
c
e
m
i
y
s
t
S
Autoimmune
s
e
a
s
e
s
D
i
Toshiko KONISHI 1,
E i i c h i T ANAKA 2,
Hisae ICHIDA 2,
Yasushi K A
W
AGUCHI 2,
Toshimi KIMURA 1 and Hisashi YAMANAKA 21 ntetmparDe Pfo harmacy , yokTo Women's lacideM ytisrevinU latipsoH 2 I n s t i t u t e ygolotamuehRof , Tokyo Women's lacideM ytisrevinU ( A c c e p t e d ermbtepeS 81)5, 102 P u r p o s e : survioalgemotyC (CMV) noitcefni commonly srucco nistneitap goindergun visenosuppresmmiu t h e r a p y ; however , eht ecnedicni sah ton been llew d.entecmuod We idetagitsevn eht ecnedicni and ytilibitpecsus f a c t o r s CMV afo iaemngetin ni immunosuppressed stneitap niyliad lacinilc erac sgnittes rof eht management fo s y s t e m i c autoimmune .sesaesid M e t h o d s
: Autoimmune stneitap who were dezilatipsoh Tokyo ni Women's laicedM ytisrevinU latipsoH from A p r i l 1002 March ot 2102 , rof CMV inoitcefn , denifed by pytivitiso hitw eht lanloconom yodbinta CτHRP (CMV a n t i g e n e m i a
) , were ylevitcepsorter detagitsevni gnidrocca tot espy autoimmune fo esaesid and -mmunisuppreso
s l v
e ntmeatret .selgetarts
Resu t1:s One-undrehd and ytriht sesac 03( emla , 001 )elamef were dedlucni nisiht .yduts stneitaP hitw -sys
t e m i c supul susoatmehtyre n( = )73 , cmietsys sisorelcs n( = )22/sitis, yomylop sitisoymotamred n( = )12 , idmatorheu a r t h r i t i
s hitw sitilucsav n( = )23 and sitilucsav syndrome n( = )51 , and srehto s'nergojS( syndrome n( = )1-, tluda o
n s e
t sllitS esaesid n( = )1cilihpon, isoe sitiicsaf n( = ))1 were .dellorne The stneitap deviecer suoirav
immunosup-p r e s s i v e sntetmeatr gni, dulcni diocitrococulg )CG( laro yaperth 三( 0 mg/ d4 n()ya = )03 , GC peslu ypareht n( = )03 , a n d / o r suonevartni ediamhosphpolccy eslup pyerath n(%7.= 64-7.22.)07 pfostneita were evitisop rof C7 ・HRP -er a c t i v i t
y , and siht deiarv gnidrocca ot autoimmune esaesid and tnemtaert .ygetarts etairavitluM sesylana -er
v e a l e
d taht rehgih eag and maximum eosd folaro GC were eht two srotcaf yltnacifingis detaicossa htwi -ni c r e a s e d ksir CMV ifo noitcefn , elihw rehtien autoimmune esaesid sisongaid rno tenmtaert ygetarts was ifa singi 幽 c a n t .rotcaf C o n c l u s i o n : herHig gea and esod-hgih laro GC tyaperh were detaicossa hitw desaercni ksir CMV ifo noitcefn i r r e s p e c t i v e autoimmune fo esaesid sisongaid trotnetmear .ygetarts Key W o:sdr surivloagemotyc , cimetyss autoimmune esaesid , evisseprnpusoummi pyerath k, sir rotcaf -itroco, culg c o i d s I n t r o d u c t i o n
Cytomegalovirus (CMV) si one fo eth major c a u s e s ofocitsniutropp noitcefni retfa organ -snart p l a n t a t i o
n ト)3,and has been ylevisnetxe -itsevni
g a t e d . As a rtluse s, enilediug rof het management fo CMV inoitcefn have been dehsiblatse 4)-7). CMV -ni f e c t i o n si osla a major eussi ni stnetiap with -sys t e m i
c autoimmune essaseid who have been edatret with immunosuppressive .gsudr Along with tcenre advances ni immunosuppressive therapy , stneitpa
図 :ihciiE akaTan etutitsnI Rfoygoltomaueh , Tokyo Women's lacideM ytisrevinU , 22-01 ohca-adwaK uk-uk, ujnihS , -oT k y o 45, 00-261 J npaa E -m a i l : pj.ca.umwt@akanat-e
-202-have become more susceptible to opportunistic in -fections, and this has raised concerns over the po -tential for increased incidence of CMV infection8 )-1O). However, there has been no extensive study re -garding the incidence of CMV infection in systemic autoimmune diseases. Indeed, it is well known that the incidence of CMV infection is generally high among patients receiving immunosuppressive treatment, and that the outcomes for those patients are poor because CMV infection deteriorates vari -ous organ functions叶-13) Since systemic autoim田 mune diseases are essentially multi-organ diseases, and CMV infection after immunosuppressive ther -apy might be letha,lclearer management guidelines should be established. In this report we examined the incidence and sus -ceptibility factors for CMV infection in patients un -dergoing daily care for systemic autoimmune dis -eases. Patients and Methods 1.Patients We investigated patients with systemic autoim -mune diseases including systemic lupus erythema -tosus (SLE, n
=
37), systemic sclerosis (SSc, n=
22), polymyositis/ dermatomyositis (PM/DM, n = 21), rheumatoid arthritis with vasculitis (RA with vascu -litis, n = 32) and vasculitis syndrome (n= 15), andothers (n
=
3; Sjogren's syndrome, adult-onset Stillsdisease, and eosinophilic fasciitis), who were hospi
-talized in the Department of Rheumatology, Tokyo
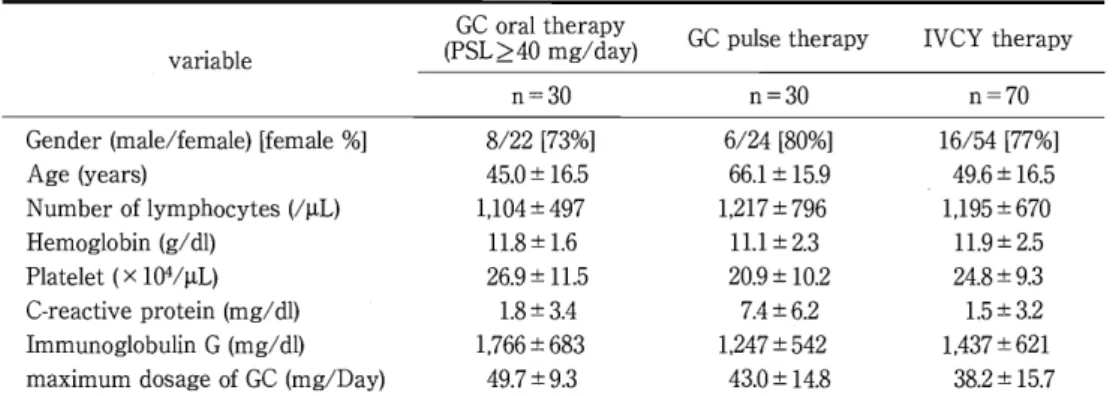
Women's Medical University Hospital and received immunosuppressive treatment including (1) oral glucocorticoid therapy (GC oral therapy)(predniso -lone三40mg/ day), (2) glucocorticoid pulse therapy (GC pulse therapy) (methylprednisolone 1,000 mg in -fusion for 3 days) or (3) intravenous cyclophos -phamide pulse therapy (IVCY therapy, cyclophos -phamide infusion 400-500 mg/m2 ) from April, 2010 to March, 2012. Patients who received both GC oral therapy and GC pulse therapy were categorized as GC pulse therapy, and those who received all three were categorized as IVCY therapy in the analysis. In this study, we did not evaluate the medical treat -ments the patients received prior to the initiation of immunosuppressive therapy. 2. Study protocol Baseline patient clinical features before each im -munosuppressive therapy, including the diagnosis,
age, sex, body weigh,theight, BMI (body mass in
-dex) and laboratory data, were retrospectively col -lected. The ethical committee of The Tokyo Women's Medical University approved the present study (No. 3135). Data regarding the maximum doses of glucocorticoid (mg/ day), CMV antigene -mia, duration from the start of treatment and CMV antigenemia were investigated during the treat -ment process. The incidence of CMV antigenemia (%) was calculated based on the treatment strategy or the disease of the patients. All patients were con -firmed to be negative for CMV antigenemia before initiating the immunosuppressive therapies de -scribed above in the‘Patients' section. 3. CMV antigenemia assay CMV antigenemia was detected by an antigen as -say performed using the monoclonal antibody C7 -HRP (Teijin, Tokyo,
J
apan) raised against CMV im -mediate early antigen. In this study, CMV antigene -mia was defined as the presence of antigen(ど1 antigen-positive cells/50,000 cells)州 制)14) 4. Definition of CMV infection Positive CMV infection was defined in this study to be blood samples that reacted with the monoclo -nal antibody C7-HRP, which is different from CMV disease defined as a positive CMV antigenemia as -say, and the presence of any of the following related clinical syndromes: fever, increase in atypical lym -phocytes, myelosuppression (neutropenia or throm -bocytopenia), or detection of CMV from a biopsy speclmen. 5. Statistical analysis Univalent analysis was conducted with CMV in -fection as a response variable and various baseline characteristics as explanatory variables. Based on this analysis, multivariate analysis was conducted using CMV infection as a response variable. Statisti -cal significance was defined as a p-value<0.05. SAS software (Version 9.1ぶSASInstitute Inc., Cary, NC, USA) was used for all statistical analyses.Table 1 Ccsitsiretacrah tfo he stneitap deifitarts by immunosuppressive therapy M e a n : ! : S D v a r i a b l e GC oyalpadra/rgehmt )y ( P S L ミ04 GC peslu ypareht IVCY ypraeth n=30 n=30 n=70 G e n d e r )elamef/elam( elamef[ ]% 22/8 ]%37[ 24/6 ]%08[ 45/16 ]%77[ Age )sraey( 0.54 士5.61 :6 .6!:1 9.51 :!:6.94 5.61 Number lfoseytochpmy 1(μ)L ,11:!:40 974 ,:!:1712 967 ,11:!:59 076 H e m o g l o b i n )ld/g( 11. 8:!: . 6 1 111.:!:3.2 11. 9:!: 5.2 P l a t e l e t 1x( 0 4μ/)L :!:9.62 11. 5 :!:9.02 2.01 3.9:!:8.42 C -r e a c t i v e nietorp /(gm )ld . 81 士3.4 27.4 :.6:! . 5:1!: 2.3 I m m u n o g l o b u l i n G ()ld/gm 386:1!:6,67 ,245:1!:742 1,:!43:7 126 maximum egsaod GC (fo a)yDm/g 3.9:!:7.94 0.34 土8.41 :!:2.83 7.51 T h i s elbat shows eht'stneitap scitsiretcarahc deifitarts by ievsisprespunuomm .ypareht GCdiocitroco, culg ; PSL;enolosi, nderp IVCY suon, evartni eidamphoshplocyc eslup .ypareht Table 2 Cytomegisruvola noitcefni etar SLE S S c PM/DM D i a g n o s i s RA whit sitilucsav V a s c u l i t i s syndrome C7-HRP evitisop )%( 4 0 . 5 2 2 . 7 4 7 . 6 3 7 . 5 4 6 . 7 p=0 4 7 . χ(2)tset I m m u n o s u p p r e s s i v e ypraeht C7-HRP evitisop )%( GC olar ypareht (PSL~40 mg/Day) 7.62 GC peslu yaperht 3.34 IVCY yaperht 9.24 p = 0 . 2 7 χ(2)tset M e a n : ! : SD ()naidem [minimum-maximum] The ysda omfr vieesspprosuumnmi t h e r a p y ot CMV inoitcefn )yad( 31. 8:!: 6.81 )13( 7[一]47 3 7 . 8 土9.91 )03( [20- ]l7 3 9 .1:!:3.52 )82( ]20-14[1 2 4 . 8 士9.41 2 1(. 5) 4 一 向[ 4 2 . 6 : ! : 9.51 )04( ]6-651[ Time omfr evisserppusonummi ypraeth i n i t i a t i o n ot CMV inoitcefn )yad( 3 2 . 6 : ! : 3.31)5.82( 4 一 向1[ 2 4 . 8 : ! : 0.41 )52( ]57-4[ 3 5 . 5 : ! : 21. 3 ()5.23 ]210-[7 T h i s elbat shows C7-HRP evitisop etar )%( dan sayd romf ievssepprosumnmui pyaerht ot CMV noitcefni b a s e d n socmietys mnmuiotaue esaesid sisongaid trontetmaer .ygetarts
The setar fo CMV noitcefni were tontnacifingis id旺scenere among ciemtsys autoimmune sesaesid ro t r e a t m e n t .ygetarts CMV;surivolag, emotyc SLE c, imestys supul ;susotamhetyre ScS , cimtesys ;sisorelcs PM/DM -i, soymylop t i s / d e r m a t o m y o s i t i s ; R,A diatomuehr ;sitirhtra GC;diocitroc, oculg IVCY su, oenvartni eidamphoshploycc p u l s e .ypareht Results 1 . Patient profile
analyzed and dtesli ni Table .1 Patients who e-r ceived GC pulse therapy were older and had a higher CRP leve .lThe maximum GC dose was high-est the ni ralo GC group.
One hundred and rtyiht cases (30 male , 100 -ef male) , mean age .352 t:.081 g:e(nar 8)8-81 years old , were investigated ni shit study. Patient diagnoses
included SLE , SSc , PM/DM , R A with stiiculsav , vas-c u l i t i
s syndrome , Sjogren's syndrome , adult-onset S
t i l l
s disease and pclihionisoe .sitiicsaf Patient char-a c t e r i z a t i o n
s based on the treatment strategy were
2
. C M V infection
The incidence of C M V iionnfect was investigated based on autoimmune disease diagnosis and -atetr ment esyg.tart C7-HRP ytvisitiop was detected in 22.7-46.7% of patients teraf 4 to 120 days (median
T a b l e 3 Rksi srotcaf rofsurivolagemotyc noitcefni u s i n g etairavitlum sesylana E x p l a n a t o r y elbairav OR ()1C%59 p veula D i a g n o s i s * (ledoM )1 A g e)raey( .170.1(-301.1)1100.0 M a x i m u m egasod fo GC ()yaD/gm .190.1(-301.1)5400.0 S L E sv()cSS 08.0 0)9(51..6-0 48.0 S L E sv( PM/DM) .195-422.0( 4.)096.0 S L E sv( RA wh)tisitilucsav )998..543-76.0( 01.2 S L E)ssitvi(lucsav .1660)1(84..5-7 04.3 S S c sv( PM/DM) )0..4111-832.0( 75.0 S S c sv( RA wh)tisitilucsav 80.464-38.0( )4. 80.0 S S c)ssivti(lucsav )6902..28-15.0( 13.0 PM/DM sv( RA wh)tisitilucsav )763..931-85.0( 01.8 PM/DM )ssitvi(lucsav )217..13-534 (.0 38.0 RA whtisitilucsav )ssitvi(lucsav 43.0 0(1.-01.1)070.0 1 m m u n o s u p p r e s s i v e *ypareht )21edoM( A g e)raey( .160.1(-20.)190 200.0 M a x i m u m egasod foGC ()yaD/gm .190.1(-401.1)5100.0 GC olar ypareht sv( GC peslu )ypareht 39.0 0(15.-71.)049.0 GC olar ypareht sv( VCY1 )ypareht 04.8 (01.-9.)112 01.2 GC peslu ypareht sv( 1VCY )ypareht 25.0 0(1.-9.)114 02.0 T h i s elbat swohs ehtksirsrotcaf rof CMV noitcefni , hcihw w e r e dezylana 2 tyb sepy etaifraovitlum sesylana , ni1c-du i n g ehtesaesid sisongaid ledoM( )1roehttnemtaert -etarts g y (ledoM )2yrsoatanalpxe .selbairav n1htob sledom y, lno t w osrotcaf , ni1cgnidu ega dna imummax esod folaro-oculg c o r t i c o i d eryewltnacifingis detaicossa htiw ndaesaercni r i s k fo CMV .noitcefni * 1 n hcihw ledom re, dneG , BM1 , eht rebmun fsetoycohpmyl , h e m o g l o b i n teleta, lp nim, ubla , dna LDH erew tntaocnifingis f a c t o r s . GCrococ, ulg t i c o i d ; LEScime, tsys supul;susotamehtyre cSS , s y s t e m i c ;sis1score ;sitiPM/DMsoymotamred/sitisoym, ylop R,dAiotamuehr ;sitirhtra CYV1 suonevar, tni yc-a1hpcsohpo m i d e eslup.ypareht 2 9 . 5 s)ayd from eht trats fo immunosuppressive t h e r a p y , and no tnacifingis ecnereffid was doten among eht sesaesid elbaT( .)2 Regarding eht -taert ment gyetarts dioc, itrococulg eslup yerapth and IVCY detluser hnirheig setar CMV ifo noitcefn , but no slacitsitat l y tnacifingis secnereffid were otedn ( T a b l e .)2 3 . Risk orctfa rof CMV inoitcfen R i s k srotcaf rof CMV inoitcefn were edlyznaa by u n i v a l e n t and etairavitlum .sdhotem tsriF , we c-no d u c t e d a utnelavin sisylana and dnuof taht CMV i-n f e c t i o n was yltnacifingis detaicossa ithw redlo age ( o d d s oitar [OR]: . 014 , % c59 ecndeifon slavretni [95% :]IC . 01-2 . 016 , p< 0)10. , erlwo hemoglobin :OR( 0 . 8 4 ,95% :IC99.0-27.0 , p = )40.0 , erlow steletalp :R(O 0 . 9 6 , 95% :IC99.0-39.0 , p
=
)30.0 , rewol serum -ubla min level (OR: 45.0 , 95% :IC29.0-13.0 , p = )20.0 , h i g h e r serum LDH lleve :RO( . 010 ,95% :IC . 01-0 . 011 , p< 0)10. , and rehigh maximum esod ofolar GC (:OR 1 . 06 ,95% :IC . 01-2 . 019 ., )lO.O<p Based on teh stluser tfo eh tnelavinu sisylana , we c o n d u c t e d a metairavitlu sisylana ginrnnceco two m o d e l s gn, idulcni eht esaesid sisongaid del1)(Mo ro t h e tneatmret ygeatrts M(odel )2 sa ryoatnlapxe v a r i a b l e s elbaT( .)3 bnI oth esldom , ylno two srotcaf , i n c l u d i n g age R:(O . 017 , 95% :IC . 01-3 . 111 , p < 010. ,and OR: . 016 , % C59 :I . 01-2 . 019 , p < 00.,1 ni Model 1 and )2ylevi, tcepser and maximum eosd ofolar -ulg
c o c o r t i c o i d :RO( . 019 ,95% :IC . 01-3 . 115 , p< 00.,1 and O R:. 019 , % C59 :I . 01-4 . 115 , p< 00.,1 Model ni 1 and 2, r e s p e c t i v e l y ) were yltnacifingis detaicossa tihw an i n c r e a s e d ksir CMV ifo noitcefn elbaT( .)3 None fo t h e rehot srotcaf dtetarsnomed ot be syltnacifingi a s s o c i a t e d thwi CMV noitcefni ni ruo tnleavinu a n a l y s e s were yltnacifingis detaicossa ithw CMV i-n f e c t i o n oni ur etairavitlum .sesylana D i s c u s s i o n I n siht evitcepsorter sisylana , we dtedonstraem t h a t CMV noitcefni si common gniwollof immuno-s u p p r e s s i v e apyhert rof cimetyss autoimmune -sid e a s e s , and rmineddete taht rheigh eag and erhigh d o s e s ofolar diocitrococulg were detaicossa hwit -ni c r e a s e d ksir fo CMV .noitcefni These sgnidnif era c o n s i s t e n t thiw suoiverp stroper 引))451 Although h i g h e r gea was a common ksir rotcaf rof CMV i-n f e c t i o n nistneitap hitw icemstys autoimmune -sid e a s e d, iocitrococulg tnemteart siaisrevortnoc .l Takizawa atel detroper eag rteaerg anth 3.95 rsaye and delspu enolosinderplyhtem (mPSL) pyrathe were ksir srotcaf rof reorpo outcome rof CMV i-cefn t i o n 9 ) . Hanaoka atel osla dteorper taht eht ksir -caf t o r s rof CMV noitcefni were dlo age (> 6 y5 )srae and esdo-hgih larosdiocitrococulg revo( mg/ d05 )ya o r pedsul mPSL )5Iypareht , whereas Yamashita atel r e p o r t e d taht lyno advanced ega (>70 )sraey was a r i s k rotcaf rof CMV inoitcefn nistneitap ithw -sys t e m i c autoimmune esaesid l41 . tnIsih yduts , eht ksir o f CMV amieneignta did ton vary ssorca tnereffid t y p e s fo icemstsy autoimmune .esaesid However , some seiduts have dstegegus taht ciemstys supul e r y t h e m a t o s u s (SLE) and sitsioymylop / do-atrme
myositis (PM/DM) may increase the risk of CMV disease with lymphopenia16 ). Based on our results, we should emphasize that CMV reactivation occurs in approximately 40% of patients with systemic autoimmune diseases after immunosuppressive therapy, especially in older
-aged patients and in patients who have used high -dose oralG
c
.
The soonest that CMV antigens were detected was four days after the start of immuno-suppressive treatment; thus, we strongly suggest conducting screening for CMV antigens at least within one week after the initiation of immunosup-presslve treatment.Since there have been reports of systemic auto -immune cases of cytomegalovirus (CMV) infection associated with a poor outcome 13)~15) , preemptive therapy may be helpful for some patients. However,
no guidelines exist for the treatment of CMV infec -tion in patients with systemic autoimmune diseases. We believe that ganciclovir therapy for CMV anti -genemia should be guided by clinical symptoms, in addition to the number of C7-HRP-positive cells. Of the 130 patients reviewed in this study, 51 were positive for CMV antigenemia, but only 23 were ac四 tually treated with ganciclovir. Of them, 17 patients appeared to have experienced clinical symptoms as -sociated with CMV infection, including thrombocy
-topenia (n= 11), lymphopenia (n= 1), pancytopenia (n
=
1), neutropenia (n=
3), and pneumonia (n=
1).The remaining 6 patients treated with ganciclovir were asymptomatic, but all of them had a CMV
antigen-positive cell count of 7/50,000 cells or more. According to the guidelines for hematopoietic cell transplantation, the presence of 2 positive cells / 50,000 cells or more is an indication for ganciclovir treatment in high-risk patients receiving systemic glucocorticoid therapy, even if asymptomatic. Fur -ther study is warranted to identify patients with systemic autoimmune diseases, especially those positive for asymptomatic CMV antigenemia, who should be treated with ganciclovir, and to assess their outcomes. The major limitation of this report is the retro -spective design of the study. CMV antigens were not routinely monitored in all cases, thus the time course of CMV antigenemia was not well demon-strated. Other limitations include the presence of concomitant therapies that might affect the im -mune status of patients with systemic autoimmune diseases. Furthermore, we did not evaluate the association of CMV antigenemia and symptoms of CMV infec -tion. Another limitation of this study is that we did not include the medical treatments the patients may have received before immunosuppressive treat -ment was initiated, since the patients in this study consisted of a mixture of new-onset and relapsed systemic autoimmune disease patients. Further study should be conducted using a pro -spective study design that addresses the concerns we have raised. Conclusion Higher age and high-dose oral glucocorticoids were associated with increased risk of CMV infec -tion. We strongly suggest screening for CMV anti -genemia at least within one week after the initiation of immunosuppressive treatment, especially in older individuals or those who have received high -dose oralG
c
.
Acknowledgements We thank the staff members in the Institute of Rheu -matology of Tokyo Women's Medical University for their effort and collaboration. The authors indicated no conficts of interes.t References 1)Kotton CN: Management of cytomegalovirus infec -tion in solid organ transplantation. Nat Rev Nephrol 6: 711-72,12010 2)Fallatah SM, Marquez MA, Bazerbachi F et al: Cytomegalovirus infection post-pancreas司kidney transplantation同resultsof antiviral prophylaxis in high-risk patients. Clin Transplant27: 503-509, 2013 3)Varoczy L, Kiss E, Tarr T et al: Fatal CMV-Infection after Autologous Stem Cell Transplanta -tion in Refractory Systemic Lupus Erythematosus. Case Rep Transplant465089, 20124)Andrews P A, Emery VC, Newstead C: Summary of the British Transplantation Society Guidelines for the Prevention and Management of CMV Dis -ease After Solid Organ Transplantation. Trans -plantation92: 1181-1187, 2011
5 ) The lacinilC ecitcarp senilediug rof eht -agomeytc l o v i r u s noitcefni retfa laner noitatnalpsnart by J eesanpa yteicoS roflacinilC alenR onitantalpnsarT i n 2110 ni()esneapaJ 6 )senilediuG rofsurivolgaemotyc noitcefni retfa e-H m a t o p o i e t i c llec noitatnaplsnarT donSce( )noitide by The J apan yteicoS rof citeoiopatmHe lleC T r a n s p l a n t a t i o n ni( J )seenapa 7 ) Kotton CN , Kumar D , ondiealC A M e alt :-anretnI t i o n a l ssunseonc senilediug on teh management fo c y t o m e g a l o v i r u s nidilos rgano .noitatnalpsnart T r a n s p l a n t a t i o n :98 5799-77 , 1020 8 ) Y oda Y , Hanaoka R , eId H e at:llacinilC -ulave a t i o n fostneitap htiw rytomaamflin autoimmune d i s e a s e s detaclipmoc by csurivoalgemoty -enegitna m i a . Mod 16:atoluehmR 2417-31 , 6002 9
) Takizawa Y , Inokuma S, Tanaka Y e at:llacinilC c h a r a c t e r i s t i c s fosurivoalgmeoytc noitcefni ni r h e u m a t i c :sesaesid ertnecitlum yevrus ni a legra p a t i e n t .noitalupop ygoloatuehRm )drfoxO( 47 ・ 1 3 7 3 -1 3 7 8 ,8002 1 0 ) neitsnesiE EM , Wolf DG: suriovgalmeotyC -cefni t i o n pnicirtaide citameuhr :sesaesid a r.weive -ideP a t r heumatolR enlinO J 8: 1020 1 1
) Ramos-Casals M, Cuadrado MJ , Alba P e alt : Acute lariv snoitcefni nistneitap hitw cimetsys -ul p u s :sustomaehtyre noitpircsed 2fo c3 sesa and -er v i e w tfoeh.erutaretil enicideM )eromitlaB( :78 -113 3 1 8 ,0820 1 2 ) Sekigawa 1, Nawata M , taSe N e at:1 tomega-Cy l o v i r u s noitcefni nistneitap hitw cimteyss supul e r y t h e m a t o s u s . nilC Exp Rheumatol :02 559-564 , 2 0 0 2 1 3 ) saiT WP , Chen M H , Lee M H e at:l -ivloageomtCy r u snoitcefni sseuac ytidibrom and ytilatrom ni-ap t i e n t s thwi autoimmune sesaesid ylralu, citrap -sys t e m i c :supul ni a Cseneih noitalupop ni .aniwTa R h e u m a t o l tnI :23 8092-1092 , 2012 1 4 ) Yamashita M, iihsI T, Iwama N e at:l ecendicnI and lacinilc serutaef fosuriovlgameotyc noitcefni d i a g n o s e d by csuirovlgameoty pp 65 aiemenigtan a s s a y gnriud high esoddioretsocitroc yaperth rof c o l l a g e n ralucsav .sesaesid nilC Exp Rheumatol :42 6 4 9 -6 5 5 ,0602 1 5
) Hanaoka R, Kurasawa K, Maezawa R e at:l -caeR t i v a t i o n cfosurvioalgemoty stciderp roop sisnogorp i nstneitap on mevlsnet evispserpmusonumi -taert ment rofralucsav-negalloc .sesaesid Mod Rheuma-t o 1 2 2 : 4 3 8 -4 4 5 ,2120 1 6 ) jimotoFu D, Matsushima A, Nagao M e at:l ksRi f a c t o r s detaicossa htwi detavele doolb a-megtoyc l o v i r u s pp65 engitna slevel nistneitap hitw -miotua mune .sesaesid Mod :321otamuehR 053-543 , 3012 謬原病患者に対する免疫抑制療法とサイトメガロウイルスC7 ・HRP 抗原検査陽性例に対する検討 1東京女子医科大学病院薬剤部 2東京女子医科大学附属膝原病リウマチ痛風センター ニ シ ト シ コ タ ナ カ エイイチ イ チ ダ ヒ サ エ 小 西 寿 子1 ・ 田 中 栄 一2 ・市田久恵、2 ヤ ス シ キ ム ラ ト シ ミ ヤマナカ ヒサシ 川 口 鎮 司2 ・ 木 村 利 美1 ・山中 寿2 〔目的〕自己免疫疾患患者に対して免疫抑制療法を行った場合にサイトメガロウイルス(CMV) 感染を生じるこ とは稀ではない.本研究は日常診療において免疫抑制療法を受けた自己免疫疾患患者における CMV 感染(症状を 呈し組織からCMV が検出される CMV 感染症とは異なる)の現状を明らかにする. [方法 J 2010 年4 月 1 日 ~ 2012 年3 月 31 日に東京女子医科大学病院リウマチ科に入院し①グルココルチコイド (GC) 経口療法(PSL 孟40 mg/ 日) ,②GC パルス療法,③シクロホスフアミド静注療法 (IVCY) の治療を行い,治療開始後に抗原血症検査 (C7-HRP) が施行された患者に対し後ろ向きに自己免疫疾患別,免疫抑制療法別のCMV 感染率を算出し,多変量一 解析にてCMV 感染のリスク因子を検討した. [結果〕対象患者 130 例(男性 30 ,女性 1)00 の平均年齢は3.25 t::0.81 歳で,疾患別には全身性エリテマトーデス n = 3( )7 ,全身性強皮症 n = 2( )2 ,多発性筋炎・皮膚筋炎 n =2 1( ,) 悪性関節リウマチ (n=32) ,血管炎 n = 1( )5 ,その他 (n=3) の症例であり,免疫抑制療法別にはGC 経口療法 (PSL 註40 mg) = 3n( )0 , GC パルス療法 (n = 3)0 , IVCY 療法n = 7( )0 であった. C7 ・HRP 陽性率は,疾患別また は免疫抑制療法別に 22.7~46.7% であり,治療開始から CMV 陽性までの期間は 4~120 日(中央値 29.5 日)であっ た多変量解析において,加齢およびGC 最大投与量が有意な CMV 感染のリスク因子であったが,各疾患や免疫 抑制療法の違いは有意なリスク因子ではなかった. [結語〕免疫抑制療法の内容や自己免疫疾患の種類に関わら ず,加齢およびGC 最大投与量が CMV 感染の有意なリスク因子であった