Implementation
to Leprosy
Control
in Thailand.
Pongrama Ramasoota1)* Tassanee Intaratitaya2)
1) National Institute for Leprosy Research, Tokyo, Japan and Faculty of Tropical Medicine, Mahidol University, Thailand.
2) Division of Leprosy Control, Department of Communicable Disease Control. Ministry of Public Health, Thailand.
[Received: 1995, 10, 17]
This paper report the progress and impact of MDT implementation to leprosy control in Thailand since 1984 until 1994. By ten years of MDT implementation, number of registered cases dropped from 44,406 in 1984 to only 4,878 cases in 1994. Which made prevalence rate declined 90% from 8.8 to 0.83 per 10,000 population, the detection rate of new case declined from 6.2 to 1.97 per 100,000 population. Total 39,372 cases have been completely covered by MDT and 22,821 cases are under post MDT surveilance with the low relapse rate only 1.46%,
other indicators showing natural decline of leprosy were increasing in proportion of
mutibacilary leprosy and mean age at onset of new case of leprosy together with decreasing
in proportion of children among new case. Other impact of MDT showing increasing trend
of proportion of new case of patient who voluntarily attend treatment centers. However,
there were still no satisfactory impact on decreasing in proportion of deformity and duration since onset to the first detection of new case of leprosy.
Thailand is A Kingdom of 513,115 km2 of the
Southeast Asia. Which has 4 geographical
regions, the central (including Bangkok as the capital city), the northern, the northeastern and
the southern region. There are 76 provinces
* Corresponding author:
Faculty of Tropical Medicine, Mahidol university. 420/6 Rajvithii Road, Phayatai,
Bangkok 10400, Thailand. Present actress;
4-2-1, Aobacho, Higashimurayama-shi, Tokyo, Japan 189.
Tel: 0423-91-8211
with population of 58,995,000 in 1994. Leprosy is one of the public health problems in Thailand, it was estimated by WHO in 1953 that there were about 140,000 cases in Thailand with prevalence rate of 50 per 10,000 population. Leprosy is
hyperendemic in northeastern region,
mesoen-demic in central and northern region, and
hypoendemic in southern region. The leprosy
control programme based on the active case
finding survey and domiciliary Dapsone
monotherapy was launch as a pilot project in 1955 and has been gradually expanded as
verti-Jpn.J.Leprosy 64, 214-219(1995)
cal programme to cover total 72 provinces by 1976. The partial integration of leprosy control activities into provincial health services began in 1971 and gradually expanded to covered 67
hypoendemic provinces (low prevalence rates)
(Fig. l) out of 73 provinces in 1976. Meanwhile 6
hyperendemic provinces were remained as the
specialized leprosy control services. They are Mahasarakam, Kalasin, Roi-et, Surin, Saraburii
and Nakornsawan Provinces.
Fig. 1 Leprosy control in Thailand 1955 - 1994.
With the problem of bacterial resistance to
Dapsone, the standard multidrug therapy
(MDT) regimen recommended by the WHO
study group (Table 1) was implemented since
1984 and has been gradually expanded to cover total 73 provinces in 1989. The leprosy control
and progress of MDT in Thailand until 1989
was reported previously(1).
MDT is the breakthrough and represent a
great step foreward in the history of leprosy
control. Technical advantage of MDT include
1. The low frequency of drug toxicity in the field; 2. The high level of acceptance; 3. Patient
satisfaction with clinical response; 4.
Significant-reduction in frequency and severity of ENL reactions and 5. Very low relapse rates following completion of treatment(2).
By the end of 1994, the total cumulative number of detected and registered patients all over the country was 169,880 out of whom 164, 303 had been released from control. There are only 4,883 registered case with distribution of 45% in north-eastern region (zone 5-7), 31% in central region (zone 1-4, 8) and each of 12% in
Northern and Southern region. (zone 11-12)
(The zone of province and zonal leprosy center are shown in Table 4)
MDT was implemented as a preprogramme
study pilot project in three provinces in 1984
before gradually expanded to cover total 73
provinces in 1989 (Table 2).
Table 2. Coverage of MDT in the treatment of lep-rosy patients in Thailand from 1984-1994.
Table 1. Mulltidrug therapy (MDT) as recommend by WHO and leprosy control programme in Thailand, 1984-1994.
* Pre - programme pilot study at Mahasarakam,
Kalasin and Roi - et provinces in the northeast of Thailand.
**
Newly expanded 3 provinces from previous 3 provinces.
Success of MDT implementation of leprosy control programme in Thailand from 1984
-of MDT implementation, number of regestered cases drop from 44,406 in 1984 to only 4,878
cases in 1994. Which made prevalence rate
declined 90% from 8.8 to 0.83 per 10,000 popula-tion. Total 39,732 cases have been completely
covered by MDT and 22,821 cases are still
under post-MDT surveillance with the low
relapse rate of only 1.46%.
these two criteria of elimination of leprosy as a public health problem.
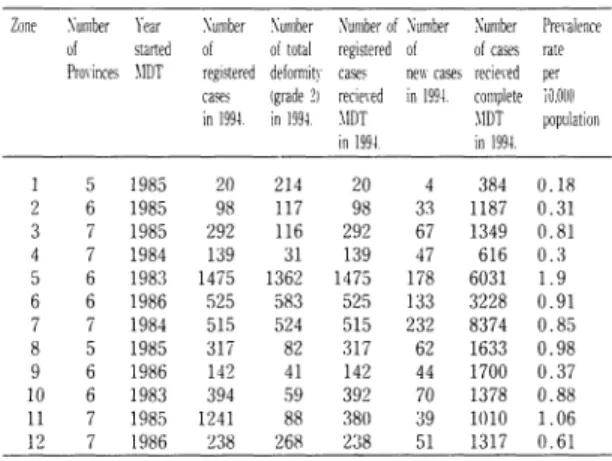
Table 4. The Progress of MDT in Thailand up to the end of 1994.
Table 3. The success of MDT to leprosy control programme in Thailand from 1984 - 1994.
zone 1. Nonthahurii, zone 2. Saraburii, zone 3. Chonburii, zone 4. Rajchaburii, zone 5. Nakornrachasiima, zone 6. Khon Khan, zone 7. Ubonrachatanii, zone 8. Nakornsawan, zone 9. Pissanulok, zone 10. Lampang, zone 11. Nalornsiitamaraj, zone 12. Song Kla
Detail informations on progress of MDT implementation in 12 zones of Thailand are shown in Table 4 . In each zone, there is zonal leprosy center to monitor and evaluated the operation of MDT implementation by integrat-ed health servicesin each province. MDT has good impact to decrease the prevalence rate to the level of less than 1 per 10,000 population in 10 zone or 52 provinces which met with the criteria of WHO that leprosy could be eliminat-ed as a public-health problem. However, the leprosy control programme in Thailand has established other criteria of elimination that the detection rate of new case of leprosy should be less than 1 per 100,000 population. Up to
As resulted from experiences of MDT in
many countries as evaluated by WHO,
when-ever MDT coverage was more than 80% of
existing registered cases, the prevalence of
leprosy will decline 10% per year. In Fig.2, shows the great impact of MDT on decline of leprosy in Thailand during the second five year after completion of MDT coverage. There were 58% of decline in prevalence rate from 3 to 1.24 per 10,000 popultion with the annual declineing rate of 11.73%. Meanwhile, the detection rate of new case also declined 30% from 3 to 2.1 per
Fig.2 Decline of prevalence rate of leprosy case after MDT implementation.
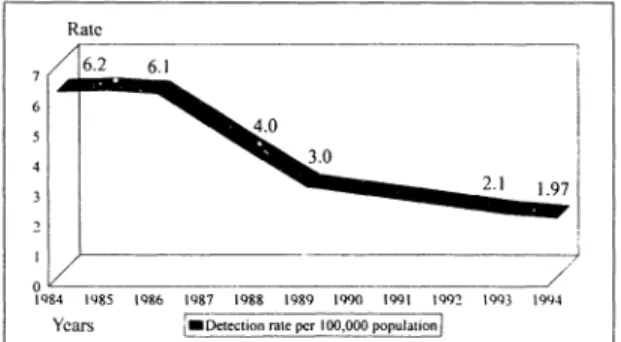
100,000 population with the declining rate of 6% per year (Fig. 3).
Fig. 3 Decline of new case detection after MDT implementation.
These indicated clearly good impact of MDT on reduction of transmission of leprosy in the community which have been resulted in natural decline of leprosy in Thailand as resulted from good impact of MDT implementation.
Apart from decline in prevalence and detec-tion rate of new case of leprosy as mentioned above, others indicators showing natural decline of leprosy were increasing in proportion of multibacillary leprosy and mean age at onset
Table 5. Impact of MDT on natural decline of lep-rosy in the second five years (1989-1993) after
MDT coverage 82% of total registered cases.
Jpn.J.Leprosy 64, 214-219(1995)
of new case of leprosy together with decreasing
in proportion of children among new
cases(Table 5.)
Other good impact of MDT also have been
found on operational aspect of leprosy control
by showing increasing trend of proportion of
new case of patient who voluntarily attened
treatment centers. However, there were still no satisfactory impact on decreasing in proportion of deformity and duration since onset to the first detection of new case of leprosy. In order
to improve these limitation. More effective
health education, disabillity prevention and
community based rehabilitation programme
will have to be intensified in the leprosy control activities so that leprosy could be not only eliminated as a public health problems but also as a social problems.
I have made my attempt to review the
prog-ress and impact of MDT implementation in
Thailand for the first ten years. In fact MDT is only the beginning of success of leprosy control but not the end of the solution. Because leprosy is lot more than the microscopic organism that cause leprosy. We still need research for better effective MDT, vaccine and better intervention
for early detection, limiting and preventing
disability and rehabilitatton in order to enable us to reach definitely the goal of elimination of leprosy as a public health problem and social problem by the year of 2000.
References
1. C. Chantaraprachoom. K. Kittiampol:
Lep-rosy control programme in Thailand, Jpn. J.
Lepr 60: 85-96(1991).
2. T. Ramasoota: Leprosy Text Book(Thai
Language), Newtummada Printing (1992).
Acknowledgement
encouragement. Thanks the Science and Tech-nology Agency of Japan (STA) for providing
Jpn.J.Leprosy 64, 214-219(1995)