( 66 )
Non-Woven PGA Fabrics for the Treatment of Pancreatic Juice Leakage -A Preliminary Report-
Yutaka KOTANI*, Zhen WANG*, Atsushi TAMURA*, Akari KAWASUMI*, Misaki TSUJI*, Maho HAYASHI*, JunkiIKEDA **, Taichi ORIKASA**, Hideki TAKAMORI**, ***, Hiroko TORII**, ****, Yuki OZAMOTO****,
Shinichiro MORITA ***, Hiroyuki TSUJIMOTO **, Mamoru URABE**, **** and Akeo HAGIWARA**
(Received Janualy21, 2013)
We developed sheets of non-woven poly (glycolic acid) PGA fabric that can act as a scaffold to form smoothly dense granulation tissue for barrier walls to localize leakage of pancreatic juice. In this study, we tested three kinds of materials: poly (L- lactide-ε-caprolactone) (copolymer) film, PGA fabric-0.9 with a mean fiber diameter of 0.9µm and PGA fabric-20 with a mean fiber diameter of 20 µm. Under general anesthesia, the pancreatic surface of rats was cauterized with an electric scalpel. Then, the pancreas was wrapped with one of the three kinds of sheets and the sheet was fixed onto the surrounding tissues. Survival was observed for five days after surgery. The survival rates were higher in the two groups of fabric-treated rats than in the other groups, although the differences were significant only for the film-treated group. Macroscopically, severe pathologic findings such as accumulation of ascites, tumor formation in whole intraperitoneal organs and generalized peritonitis occurred at a significantly lower incidence in the two fabric-treated groups than in the film-treated group. Microscopically, granulation tissue was formed along the fabrics throughout the full thickness of the fabric scaffolds of fabric-0.9 and fabric-20. In these groups, injurious tissue changes and inflammatory reactions were reduced in the outer zone of the fabric wall compared to that observed in the inner zone. Therefore, the new PGA fabrics successfully localized pancreatic juice leakage. In contrast, in the no treatment group and the film-treated group, injurious tissue changes and severe inflammation were spread out to places distant from the cauterized pancreas. In the film-treated group in particular, the accumulation of mono nuclear inflammatory cells was spread along the film, even into the outer zone of the sheet, and granulation formation of a barrier wall was suppressed around the film. Therefore, in the film-treated group, tissue injury and inflammation caused by pancreatic juice extended more widely and granulation formation of a barrier wall was strongly suppressed, even compared with that observed in the no treatment group. In conclusion, these fabrics can be a more suitable and effective material for the treatment of leakage of pancreatic juice.
Key words: leakage of pancreatic juice, non-woven fabrics, scaffold, granulation tissue, localization
* Undergraduate Senior, Department of Medical Life System, Doshisha University, Kyoto Telephone:+81-774-65-6878,E-mail: [email protected]
** Department of Medical Life System, Doshisha University, Kyoto
*** Research and Development Department, Gunze Ltd., Ayabe-shi, Kyoto, Japan
**** Kusatsu General Hospital, Shiga Corresponding Author: Akeo HAGIWARA
Telephone:+81-774-65-6878,E-mail: [email protected]
( 67 ) 1.Introduction
Leakage of pancreatic juice and the development of pancreatic fistula, which occur as a result of pancreatic injury, pancreatic autolysis and anastomotic breakdown of the pancreatic duct, constitute one of the most striking pathologic states due to the injurious effects of pancreatic juice. In response to the leaking pancreatic juice, the body takes defensive reactions to form barrier walls composed of granulation tissue. This process is induced by inflammatory reactions that promote the development of granulation barrier walls to localize and block leaking of pancreatic juice. It is, however, difficult for granulation barrier walls to localize pancreatic juice and to block the leakage because the granulation barrier walls are digested and broken down by a variety of digestive enzymes such as pepsin and lipase that are contained in pancreatic juice.
Therefore, unlike leakage of other substances, leakage of pancreatic juice is difficult to be localized and sometimes spreads over the abdominal cavity, where it digests the body’s own tissues and induces severe injurious tissue damage. Once leakage of pancreatic juice occurs, the process can be prolonged and exacerbated and is associated with intestinal dilation, intra-abdominal abscess formation, wound infections, sepsis, hemorrhage, the need for reoperation, extended hospitalization and mortality1-4). Much of the morbidity associated with pancreatic resection can be attributed to the development of postoperative pancreatic fistula (POPF) 5). The incidence of POPF varies depending on the definition applied, although it ranges between 10%
and 30%1, 6-12). These complications also increase costs associated with pancreatic surgery. Therefore, the leakage of pancreatic juice is a common and potentially devastating complication whose management is very important for the treatment of pancreatic diseases.
The usual effective treatment for leakage of pancreatic juice involves the suppression of pancreatic
secretion by mechanisms such as fasting, the administration of proteinase inhibitors and drainage of discharge. However, there are no established methods to effectively localize and prevent the spread of leakage.
Therefore, we developed a new scaffold that functions as a granulation barrier wall. The new scaffold is a non- woven PGA fabric made of submicron fibers. PGA is not degraded enzymatically and submicron-fibered fabric supplies dense and uniform granulation tissue smoothly13). The aim of this experiment was to evaluate whether this new scaffold of PGA fabric could achieve successful localization of pancreatic juice leakage.
2.Materials and Methods
2.1 Materials
In this study, we tested three kinds of materials:
poly (L-lactide-ε-caprolactone) (copolymer) film and two types of non-woven poly (glycolic acid) (PGA) fabrics. One of these fabrics was fabric-0.9, which had a mean fiber diameter of 0.9 µm, and the other was fabric-20, which had a mean fiber diameter of 20 µm.
2.2 Preparation of non-woven PGA fabrics and copolymer
Fabric-0.9 was created using the melt-blowing method.14) PGA polymer was extruded through dies with small nozzles, attenuated with heat and high- velocity air streams and spun into fibers. The fibers were then deposited on to a collector in a random manner to from non-woven fabric.
Fabric-20 was created using the needle punch method15). The needle punch method is a two step process. PGA resin was extruded into fibers, then stretched and crimped. The PGA fibers were carded, needle-punched and then thermally interlocked.
Copolymer film with a thickness of 0.1 mm was created by melt pressing under 15MPa at 110℃ for five minutes followed by subsequent quenching in ice water.
To remove water, the resultant film was dried under a vacuum at room temperature for one day.
( 68 ) 2.3 Fiber diameter and spacing size of the non-woven PGA fabrics
The PGA fibers were analyzed morphologically using a scanning electron microscopy (SEM). The fiber diameter was determined with the SEM by measuring 30 fibers at random per sample. The data were presented as the mean ± standard deviation (SD). The distance between the edges of neighboring fibers on the same plain was defined as the fiber spacing (spacing size) 16). The spacing size was also determined using SEM by measuring 30 fiber spacing sizes at random and presenting the data as the mean ± SD.
2.4 Preparation of square sheets of non-woven PGA fabrics and copolymer film for the animal experiments
Each of the two types of non-woven PGA fabric was cut into square-shaped sheets (square sheet) measuring 20 mm × 20 mm in size and weighing 15.0 mg. The copolymer film was also cut into square sheets of 20 mm × 20 mm in size weighing 50.0 mg.
The square sheets were sterilized by soaking in 99.5% ethanol for 60 seconds followed by rinsing twice in saline just prior to implantation into the tissues of the rats.
2.5 Animals and experimental design
The animal experiments were approved by the Doshisha University Animal Experimentation Committee. All surgical and anesthetic procedures were performed in accordance with the animal care guidelines of Doshisha University.
Twenty-four female Wistar rats ranging from 200 to 220 g in weight were used in this study. During the experimental period, all rats were housed separately and maintained under standard specific pathogen-free conditions (a light-dark cycle of 12:12 hours, a mean temperature of 23 degrees Celsius and a mean humidity of 50%). Standard laboratory rodent chow and water were available ad libitum. Before the study, the rats were housed in the laboratory for one week. On the experimental day, all rats were checked for the condition of their health, concerning diarrhea, body hair
condition (hair loss and filthy hair), mucous discharge from the eyes and anus and emaciation.
Twenty four rats were randomly assigned into four groups of six rats each: the PGA fabric-0.9 group, the PGA fabric-20 group, the copolymer film group and the no treatment group.
2.6 Surgical technique
All operations were performed under sterile conditions. The surgical procedures were divided into four processes, and each process was performed by one surgeon.
The rats were given Isoflurane (Escain®, Mairan Seiyaku, Inc., Osaka, Japan) inhalation anesthesia.
Sodium pentobarbital at a dose of 6.48 mg (Somnopentyl®, Kyoritsu Seiyaku, Inc., Tokyo, Japan) was diluted in 1 ml of physiological saline solution then administered intraperitoneally to each rat using a tuberculin syringe and 23-G injection needles. Under the aforementioned general anesthesia, the rats were placed in the dorsal position. In each rat, a 5-cm long median trans-abdominal incision was made.
Then, the stomach, spleen and omental sac, including the pancreas in the posterior wall, were pulled out of the abdominal cavity, and the anterior wall of the omental sac was opened to expose the anterior surface of the pancreas. The pancreatic surface was cauterized with an electric scalpel (PROG®, MORITA, TOKYO, MFG, CORP) in COAG mode (high-frequency output 18W) in a square shape (measuring 1.2 mm × 1.2 mm in size) on the inner side of the omental sac, as shown in Fig. 1.
In the three groups in which treatments were given, the pancreas was wrapped by a square sheet of one of the three kinds of fabrics, and the sheet was sutured at all four corners onto the surrounding tissue (Fig. 2) in order to cover the cauterized portion with 7/0 polyvinylidene fluoride monofilament sutures for microsurgery (Asflex®, Kono Seisakusyo Co., Chiba, Japan). In the no treatment group, no square sheets were applied.
( 69 ) After completing these procedures, the laparotomy incision was closed with 4/0 polyamide sutures using two-layered sutures, the muscle layer was closed with continuous sutures and the skin was closed with interrupted sutures. These 24 rats were housed under the standard conditions for five days.
Fig. 1. Cauterization of the pancreatic surface.
Fig. 2. A PGA (fabric-20) square sheet sutured on the pancreas.
2.7 Mortality due to pancreatic cauterization
The survival rate of the rats was observed during five days after surgery because a preliminary examination showed that all deaths should occur within five days after surgery in this experimental model. The survival rates were compared between the groups.
2.8 Macroscopic and microscopic evaluations
The survivors were sacrificed on day 5. They were given ethyl ether inhalation anesthesia followed by a lethal dose of sodium pentobarbital (97.2 mg/kg of body weight). All of the surviving and mortal rats were autopsied to macroscopically assess the pathologic
findings of the cause of death and the spread of injurious tissue changes caused by pancreatic juice. The inflammatory tumors of the adhering intraperitoneal organs were surgically excised en bloc as specimens for microscopic examination. The specimens were fixed with a 10% neutral formalin solution and prepared into thin sections (4 µm in thickness) stained with hematoxylin-eosin using standard procedures for histological examination. All specimens were assessed microscopically from two points of view: the presence of infiltrating cells and granulation formation based on the scaffold of the square sheet, and the differences in injurious tissue changes caused by pancreatic juice between the outside and inside zones of the sheet.
3.Results
3.1 Mortality rate
Table 1. Survival after five days.
Dead rats / All rats No treatment
group 2/6
Fabric-20 group 0/6*
Fabric-0.9 group 0/6#
Film group 3/6*#
*~*,#~#: p<0.05
The number of rats that died during the observation period was two, zero, zero and three in the no treatment group, the fabric-20 group, the fabric-0.9 group and the film-treated group, respectively. There were significant differences between the film-treated group and the two fabric-treated groups (p<0.05), whereas there were no significant differences between the no treatment group and any of the other three groups (Table 1).
( 70 ) 3.2 Macroscopic evaluatio
Severe pathologic findings such as accumulation of ascites, tumor formation in whole intraperitoneal organs and generalized peritonitis were seen at significantly higher incidences in the dead rats than in the surviving rats (Table 2). The total number of these pathologic findings was significantly smaller in the two fabric groups than in the film-treated group (Table 4).
Table 2. Incidence of intraperitoneal symptoms.
*~*: p<0.001
Table 3. Intraperitoneal symptoms.
Table 4. Intraperitoneal symptoms.
**~**: p<0.001; +~+, *~*, #~#: p<0.05 Pathologic
findings Surviving Dead
Ascites 2/19 4/5
Tumor of whole
organ 0/19 4/5
Intestinal dilation 1/19 0/5
Generalized
peritonitis 2/19 4/5
Totals 5/76* 12/20*
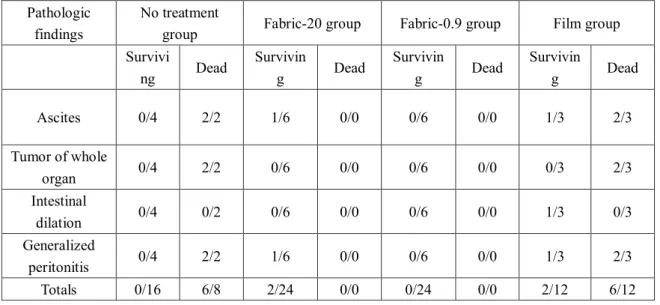
Pathologic findings
No treatment
group Fabric-20 group Fabric-0.9 group Film group Survivi
ng Dead Survivin
g Dead Survivin
g Dead Survivin
g Dead
Ascites 0/4 2/2 1/6 0/0 0/6 0/0 1/3 2/3
Tumor of whole
organ 0/4 2/2 0/6 0/0 0/6 0/0 0/3 2/3
Intestinal
dilation 0/4 0/2 0/6 0/0 0/6 0/0 1/3 0/3
Generalized
peritonitis 0/4 2/2 1/6 0/0 0/6 0/0 1/3 2/3
Totals 0/16 6/8 2/24 0/0 0/24 0/0 2/12 6/12
Pathologic Findings
No treatment
group
Fabric- 20 group
Fabric- 0.9 group
Film group
Ascites 2/6 1/6 0/6# 3/6#
Tumor of
whole organ 2/6 0/6 0/6 2/6
Intestinal
dilation 0/6 0/6 0/6 1/6
Generalized
peritonitis 2/6 1/6 0/6* 3/6*
Totals 6/24 2/24+ 0/24** 9/24**+
( 71 ) 3.3 Microscopic evaluation
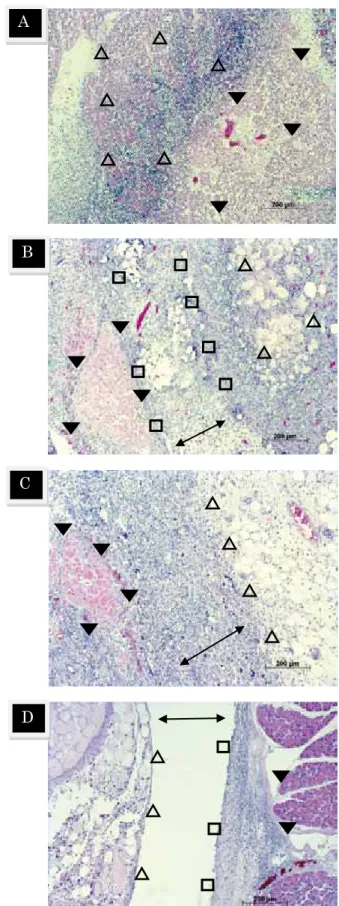
Microscopically granulation tissue was formed throughout the full thickness of the fabric scaffold of fabric-0.9 as well as fabric-20. In both the fabric-0.9 and fabric-20 groups, injurious tissue changes and the spread of inflammation induced by leaking pancreatic juice were less severe in the outer zone of the fabric wall than in the inner zone. Therefore, walls of granulation were formed along both fabric-0.9 and fabric-20 in the shape of a barrier that blocked the injurious tissue changes into the inner part enclosed by the fabric.
In the fabric-0.9 group, granulation was formed uniformly throughout the full thickness of the wall (Fig.
3A). In contrast, in the fabric-20 group, the granulation formation was irregular and depended on the fiber distribution; between the fiber bundles, the formation was sometimes rough, while injurious tissue changes were recognized on the outside of the rough wall, which suggested breakdown of the wall by pancreatic juice (Fig.
3B).
In the no treatment group (Fig. 3C) and the film- treated group, injurious tissue changes and severe inflammation were spread out to the places distant from the cauterized pancreas, as compared with that observed in the fabric-0.9 group and the fabric-20 group. In the film-treated group in particular (Fig. 3D), accumulation of mono nuclear inflammatory cells was found spreading along the film, even into the outer zone of the sheet, and granulation formation of a barrier wall was suppressed around the film. Therefore, in the film-treated group, the tissue injury and inflammation caused by pancreatic juice was extended more widely, and granulation formation of the barrier wall was strongly suppressed, when compared with that observed in the no treatment group, fabric-0.9 and fabric-20 groups.
Fig. 3. The presence of infiltrating cells on each of the three kinds of square sheets on day 5. (A: no treatment) ▼:
Necrotic pancreas-tissues. △ : Severe necrosis and A
B
C
D
( 72 ) inflammation reached the surrounding pancreas-tissues. (B:
fabric-20) ↕: A barrier wall of non-uniform granulation tissue formed in the scaffolds of PGA fabric with fiber diameter of 20μm. ▼:Necrotic pancreas tissues. □:Fiber bundle.
△:Necrotic and degenerative changes reached the outside of the barrier wall. These changes were caused by pancreatic juice which spread though the space of rough granulation tissue that formed between the fiber bundles. (C: fabric-0.9) ↕:A barrier wall of dense and uniform granulation tissue formed in the scaffolds of PGA fabric with a fiber diameter of 0.9μm. ▼:
Necrotic pancreas-tissues. Tissue injury was blocked by the barrier wall, and outside of the barrier the tissue injury and inflammation were relieved (△). (D: film) ↕:Space where the film was located. ▼ :Degenerative pancreas-tissues.
□:On the inside of the film, no granulation tissue formed although a lot of inflammatory mono-nuclear cells were found to have accumulated. △:Severe necrosis and inflammation were recognized outside of the film.
4.Discussion and Conclusion
In response to leaking pancreatic juice, the body takes defensive reactions to form barrier walls composed of granulation tissue to localize and block the leakage of the pancreatic juice. However, unlike leakage of other substances, leakage of pancreatic juice is difficult to be localized or blocked with barrier walls composed of granulation tissue because the granulation tissue is digested and the barrier wall is broken down by a variety of digestive enzymes such as pepsin and lipase that are contained in the pancreatic juice. Therefore, leakage of pancreatic juice is difficult to be localized and sometimes spreads over the abdominal cavity where pancreatic juice digests the body’s own tissues, resulting in severe inflammation. Hence, the leakage of pancreatic juice is sometimes prolonged and can go severe.
There are currently no artificial materials that can successfully localize and prevent the spread of the leakage. In order to form granulation tissue as a barrier wall to effectively localize leakage, we have developed a
new scaffold composed of non-woven PGA fabric, a biodegradable aliphatic polyester that has been applied as a scaffold for tissue regeneration in a variety of medical fields. PGA exhibits high strength, and its degradation rate is very predictable17) because its degradation does not depend on the actions of pancreatic juice, unlike the usual sealant fibrin glue. The characteristics of PGA fabric are suitable for use as a scaffold to form stable granulation as a barrier wall to protect against pancreatic juice.
In this study, the macroscopic findings in the dead rats showed that inflammation caused by leakage of pancreatic juice was not localized and instead spread throughout the entire abdomen. The microscopic examinations of the dead rats revealed that inflammatory changes and severe tissue digestion extended over the abdominal cavity. In contrast, in most of the surviving rats, the inflammation was localized both macroscopically and microscopically. This indicates that the deaths were caused by generalized peritonitis induced by pancreatic juice that widely spread throughout the abdomen.
In the mortality rate, the rats in the two fabric groups showed better survival rates than those in the other groups, although the difference was significant only in the film-treated group because the number of animals was too small. In the two fabric groups, macroscopically, the inflammation was localized, and a microscopic examination revealed that barrier walls of granulation were formed along the fabrics that blocked the spread of injurious and inflammatory tissue-changes induced by pancreatic juice in the inner part enclosed by the fabric. Therefore, fabric-0.9 and fabric-20 formed granulation barrier walls that successfully localized the leakage within the neighboring site of the cauterized pancreas. The macroscopic and microscopic examinations showed that both types of PGA fabric acted as scaffolds to form granulation walls as stable barriers against pancreatic juice. This means that both types of PGA fabric are useful for localizing the
( 73 ) discharge of pancreatic juice and treating leakage.
Usually, the minimal size of PGA fibers is 10 µm in diameter18), which is larger than the fibers of the extracellular matrix (50 to 500 nm in diameter) 19-21). Recently, we devised PGA fibers with diameters of submicron sizes. We prepared two types of PGA fabrics:
a clinically used fabric made of 20 micrometer-sized fibers and a newly developed fabric made of submicron- sized fibers. We have already shown that the latter supplies dense granulation tissue more smoothly than the former13). Indeed, in the present examination, the fabric- 0.9 formed a dense and uniform granulation wall that was difficult to break down, as compared with fabric-20.
These results suggest that fabric-0.9 can be a more suitable and effective material for the treatment of leakage of pancreatic juice.
Mortality and macroscopic localization of intraperitoneal pathologic changes were the worst in the film-treated group. In the film-treated group, microscopically, acute inflammatory changes extended widely, and granulation formation of a barrier wall was strongly suppressed, even when compared with that observed in the no treatment group. These findings suggest that the film does not act as a barrier wall to block leaking of pancreatic juice, but rather functions as a guide wall along which the pancreatic juice can flow and spread. The results observed in the film-treated group indicate that the pancreatic juice was not localized, but instead spread widely and induced severe inflammation throughout the peritoneal cavity. This difference may arise from differences in the forms of the film and fabric and/or differences in the raw materials of PGA and copolymer 22, 23).
Further examinations are necessary to elucidate this issue.
References
1) C. J. Yeo, J. L. Cameron, T. A. Sohn, K.D. Lillemoe, H. A. Pitt, M. A. Talamini, R. H. Hruban, S. E. Ord,
P.K. Sauter, J. Coleman, M. L. Zahurak, L. B.
Grochow, R. A. Abrams. Six hundred fifty consecutive pancreaticoduodenectomies in the 1990s: pathology, complications, and outcomes. Ann Surg. discussion , 57–60, 226:248–257(1997).
2) K. M. Reid-Lombardo, M. B. Farnell, S. Crippa, M.
Barnett, G. Maupin, C. Bassi, L. W. Traverso.
Pancreatic anastomotic leakage after pancreaticoduodenectomy in 1507 patients: a report from the Pancreatic Anastomotic Leak Study Group.
J Gastrointest Surg, discussion 9, 11:1451–
1458(2007).
3) E. Lermite, P. Pessaux, O. Brehant, C. Teyssedou, I.
Pelletier, S. Etienne, J. P. Arnaud. Risk factors of pancreatic fistula and delayed gastric emptying after
pancreaticoduodenectomy with
pancreaticogastrostomy. J Am Coll Surg, 204:588–
596(2007).
4) C. M. Schmidt, J. Choi, E. S. Powell, C. T.
Yiannoutsos, N. J. Zyromski, A. Nakeeb, H. A. Pitt, E. A. Wiebke, J. A. Madura, K. D. Lillemoe.
Pancreatic fistula following
pancreaticoduodenectomy: clinical predictors and patient outcomes. HPB Surg, 404520(2009).
5) G. Veillette, I. Dominguez, C. Ferrone, S.P. Thayer, D. McGrath, A. L. Warshaw, C. Fernández-del Castillo. Implications and management of pancreatic fistulas following pancreaticoduodenectomy: the Massachusetts General Hospital experience. Arch Surg, 143:476–481(2008).
6) M. P. Callery, W. B. Pratt, C. M. Vollmer., Jr Prevention and management of pancreatic fistula. J Gastrointest Surg, 13:163–173(2009).
7) R. F. Payne, J. A. Pain. Duct-to-mucosa pancreaticogastrostomy is a safe anastomosis following pancreaticoduodenectomy. Br J Surg.
93:73–77(2006).
8) C. Bassi, G. Butturini, E. Molinari, G. Mascetta, R.
Salvia, M. Falconi, A. Gumbs, P. Pederzoli.
Pancreatic fistula rate after pancreatic resection. The importance of definitions. Dig Surg, 21:54–59(2004).
9) S. R. Grobmyer, D. E. Rivadeneira, C. A. Goodman, P. Mackrell, M. D. Lieberman, J. M. Daly. Pancreatic anastomotic failure after pancreaticoduodenectomy.
Am J Surg, 180:117–120 (2000).
10) M. I. van Berge Henegouwen, L. T. De Wit, T. M.
Van Gulik, H. Obertop, D. J. Gouma. Incidence, risk factors, and treatment of pancreatic leakage after
( 74 ) pancreaticoduodenectomy: drainage versus resection of the pancreatic remnant. J Am Coll Surg, 185:18–
24(1997).
11) J. J. Cullen, M. G. Sarr, D. M. Ilstrup. Pancreatic anastomotic leak after pancreaticoduodenectomy:
incidence, significance, and management. Am J Surg, 168:295–298(1994).
12) Y. M. Yang, X. D. Tian, Y. Zhuang, W. M. Wang, Y.
L. Wan, Y. T. Huang. Risk factors of pancreatic leakage after pancreaticoduodenectomy. World J Gastroenterol, 11:2456–2461(2005).
13) T. Orikasa, J. Ikeda, A. Tanzawa, M. Matoba, Y.
Iwame, C. Yoshida, H. Torii, Y. Ozamoto, A.
Hashimoto, H. Tsujimoto, A. Hagiwara, ”changes in granulation-formation induced by different fiber- diameters and fiber-spacing in scaffolds for tissue- regeneration -Preliminary study-” , The science and engineering review of Doshisha University, 53, 42- 48(2012).
14) F. Zhou, R. Gong, “Manufacturing technologies of polymeric nanofibres and nanofibre yarns.”, Polymer International, 57, 837-845 (2008).
15) JP 2005-3664367 (June 22, 2005).
16) J. E. Sanders, S. E. Lamont, S. B. Mitchell and S. G.
Malcolm, “Small fiber diameter fibro-porous meshes: Tissue response sensitivity to fiber spacing”, Journal of Biomedical Materials Research Part A, 72A, 335–342 (2005).
17) Y. Dong, S. Liao, M. Ngiam, C. K. Chan and S.
Ramakrishna, “Degradation behaviors of electrospun resorbable polyester nanofibers”, Tissue Engineering Part B, Reviews, 15, 333-351 (2009).
18) D. Mooney and R. Langer, “Engineering biomaterials for tissue engineering: the 10–100 micron size scale”, J. Bronzino (Ed.), The Biomedical Engineering Handbook, CRC Press, Boca Raton, pp, 1609–1618 (1995).
19) E. D. Hay, “Cell biology of extracellular matrix” 2nd edition, Plenum Press, New York (1991).
20) T. Elsdale and J. Bard, “Collagen substrata for studies on cell behavior”, J Cell Biology, 54, 626–
637 (1972).
21) E. Karl, F. David and A. John, “Collagen fibril formation”, Biochem. J, 316, 1-11 (1996).
22) K. Ceonzo, A. Gaynor, L. Shaffer, K. Kojima, C. A.
Vacanti, G. L. Stahl, “Polyglycolic acid induced inflammation”, Tissue Eng, 12(2): 301–308(2006).
23) J. Jin, K. K. Zhou, K. Park, Y. Hu, X. Xu, Z. Zheng,
P. Tyagi, U. B. Kompella, and J. Ma, “Anti- inflammatory and Antiangiogenic Effects of Nanoparticle-Mediated Delivery of a Natural Angiogenic Inhibitor”, Invest Ophthalmol Vis Sci, 52(9): 6230–6237(2011).