NII-Electronic Library Service
-#fitrveg34tseg8e
328-334fi
(2007ff)
meereagfiifm
Function-
VersusPain-Centred
Concepts
and
Treatment
of
Low
Back
Pain:
Outcome
*
Peter
R,OESCH,MSc,
PT
**Ab$tract
Return
to
workis
the
primary
goal
in
the
treatment
ofpatients
withlow
back
pain.
Treatment
canbe
pre-scribed on
the
base
of abiomechanical
model assumingthat
aphysical
pathologic
conditionleads
to
pain
anddisability.
It
empleys a"Pain-Centered
Treatment"
(PCT)
administering various measures ofpain
therapy.
The
bTopsychosocial
model acknowledgesthe
role ofpsychological
and socialfactors
as well asphysical
factors
lead-ing
to
permanent
disability.
On
the
base
ofthis
model"Function-Centered
treatment"
(FCT}
emphasizing improve-mentin
function
and notprimarily
pain
relief weredeveloped
to
facilitate
returnto
work.It
remains unelearwhether
treatment
based
onthe
biornedical
rnodel withits
restrictive recommendationsis
more effectivein
reducing work absenteeism
than
treatment
applying thebiopsychosocial
modelprimarily
emphasizing activity.We
conducted a randomized controlled trialin
Switzerland
in
patients
with sickleave
due
to
non-specificnon-acute
lew
back
pain
(LBP)
to
evaluate
the
effect ofthree
weeks offunction-centered
compared withpain-cen-tered
in-patient
rehabilitationi'2).Inclusion
Criteria
were >6 weeks out of workdue
to
chronic non-specificLBP.
174
patients
wereincluded:
mean sickleave
was6.5
months,Groups
were comparable atbaseline.
Results
FCT
vs
PCT:
atdischarge
seff-efficacy +5.9points
vs,-7.4
points
(ES
=O,55,
p
=O.O03),
lifting
capacity +2.3kgs
vs.+O.2
kgs
(ES
=O.54,
p
=O,O04}:
after3
monthsdays
at work were25,9
vs15.8
{ES
=O.36,
p
=O.029}:
after12
month
days
at work were118
vs74
(ES
=O.35,
p
=O.Oll),
From
these
findings
we can concludethat
FCT
is
more effective
than
PCT
for
increasing
workdays.
Key
word$ Ilow
back
pain,
returnto
work, exercisetherapy,
randemized controEledtrial
lntroduction
Bacaground
Low
back
pain
(LBP)
has
become
a majorhealth
preblem
in
alldeveloped
countries, causing anincrease
in
sickness absence, rehabilization allewances anddisability
pensions3),
The
increasing
rate ofdisability
due
to
chroniclow
back
pain
(CLBP)
has
led
to
an explosionin
costs4).60-75%
ofthe
total
medical andindirect
costs ofLBP
canbe
attributedto
the
people
disabled
due
to
CLBP5).
In
Switzerland
the
num-ber
ofpensioners
in
the
last
ten
years
has
grown
annuallyby
an average of3.5%6),
Musculoskeletal
disorders
including
CLBP
were one ofthe
two
causesfor
disability
withthe
biggest
annualgrowth
and are, at31%,
the
secondlargest
***mde'iftasodikt
ntm
:
scAegzawiftut
vs.v4fimemagiaff
Correspondence:
Peter
R.
Oesh,
MSc,
PT
Rheuma-
undRehabilitationszentrum
Valens,
CH-7317
SwitzerLand
{e-mail/
[email protected])Valens,
reason
to
receive adisability
pension7),
Dicrgnosis
ofLow
Back
Pain
Only
afew
patients
have
pathoanatomically
well-defineddiseases,
Known
causesfor
specificback
pain
are vertebralfracture,
tumour,
infectTon,
inflammatory
diseases,
nerve root compression, spondylolysthesis, spinal stenosis anddefinite
instability8}.
Evidence
suggeststhat
fewer
than
15%
of indi-viduals withback
pain
canbe
assignedto
one ofthese
spe-cificback
pain
categories9),In
the
remaining85%
ofpatients
with
back
pain
a specificdiagnosis
is
impossibie.
This
has
led
to
a widediversity
of syndromesdepending
heavily
onthe
individual
physicianiO),
Patients
withback
pain
arelike-ly
to
receive'differentlabels
from
different
specialists, such asdiagnosis
ofdegenerative
disc
disease,
facet
syndrome,instability,
and sacroiliacpaTn,
There
is
little
scientificevi-dence
for
establishment ofmany ofthese
diagnostic
Iabelsii),
Besides
the
history
andphysical
examination ofpatients
with spinalproblems,
radiological examinations arefrequently
Function-
Versus
Pain-Centred
Treatment
ofusedi2).
However,
the
frequent
use of radiographyis
notjus-tified
by
the
eutcome.No
causal relationshipbetween
radi-ographic
findings
and non-specificlow
back
pain
has
been
foundi3).
Guidelines
for
7}'eatnzent
ofIVbn-Specific
Low
Back
Pain
The
failure
of modern medicineto
diagnose
the
anatomi-cal structure causinglow
back
pain
andto
relievepain
anddisabllity
in
chronicpain
patients
has
led
to
adifferent
treat-ment approach
in
thepast
two
decades,
Two
major reviewsconcluded
that
Return-To-Work
and notpain
relief mustbe
the
primary
goal
in
treatment
of chronicback
pain
patientsi4).
The
Paris
Task
Force
Report
found
consistent scientific evidencein
morethan
adozen
experimentalran-demized
studiesfor
pregrammes
combining stretching,strength and
fitness
training
reducingthe
duration
ofback-pain-related
incapacity,
Hewever,
adetailed
analysis ofthese
artlcles
indicated
that
they
generally
provided
inadequate
descriptions
ofhow
activityis
prescribed
to
patients
whohave
back
pain.
The
authors concluded,'`it
appearsthat
the
key
to
successis
physical
activityitself
-i.e,
activity of anyform-
ratherthan
any specific activity''i4).Pain-Centred
Vlersus
Funetion-Centred
Z'eatment
Physical
activity canbe
prescribed onthe
base
of a bio-mechanical medelor
a
biopsychosocial
treatment
approach.The
(traditional)
biomechanical
model ofdisease
mainlyfocus-es on somatic
Tssues.
It
is
based
on theidea
that aphysi-cal
pathologic
conditionleads
to
pain
anddisability.
Clinical
recognition and
cliagnosis
ofthe
underlyingpathologic
cen-dition
prevides
the
basis
for
rationalphysical
treatment
ofthe
illnessi5).
This
modelis
refiectedin
the
frequentiy
restric-tive
recommenclations ofphysicians
regarding activity and worki6).In
orderto
controlpain,
various measures ofpain
therapy
such astrigger
point
massage, acupuncture,physi-cal
treatment
(e,g.
electrotherapy,balneetherapy)
arepre-scribed.
Exercise
therapy
is
administeredbut
pain
intensity
is
used as aguideline
to
determine
the
intensity
ofthe
exer-cises,A
biomechanical
approachlike
this
maylead
to
overtpain
behaviouri5).
The
biopsychosocial
modeldeveloped
more recently acknowledgesthat
otherfactors
than
tissue
damage
andresulting
pain
are responsiblefor
permanent
disability.
It
emphasizes the role of
psychological
factors
such aspersonal
beliefs,
illness
behaviour
andfear
avoidance as weli as socialfacters
such asfamily,
work and wider social networkin
thedevelopment
and maintenance of syrnptomsi7),On
the
base
ofthis
model werkhardening
programmesiS)
andfunc-tional
restorationprogrammesig)
emphasizingimprovement
in
function
and notprimarily
pain
relief weredeveloped
withthe
intention
of overcomingthe
dysfunctional
illness
behav-Low
Back
Pain:
Concepts
andOutcome
329
iour
andimplementing
ergenomic and socialintervelltions
to
facilitate
returnte
work,What
is
the
Evtdence
ofExerciseto
Achieve
Return
to
Wbrke
Until
the
end ofthe
20th
centurythere
was contradicto-ry evidence whether vocational outcomes canbe
improved
by
exercises or anintensive
multidisciplinary bio-psychoso-cialintervention2e'22).
However,
two
recentlypublished
meta-analysesfound
strong evidencethat
sickdays
canbe
reducedby
exercise23'24),One
studyfound
that
93%
(14f15)
of
the
RCTs
investigated
wereperformed
in
Scandinavia
andconcluded
that
further
researchis
neededin
othercoun-tries24).
It
also remainsunciear
whethertreatrnent
based
onthe
biomedical
model withits
restrictive recommendationsis
more effectivein
reducing work absenteeismthan
treat-ment applying
the
biopsychosocial
modelprimarily
empha-slzmg actlvlty.
In
view efthese
findings
we conducted a randomizedcon-trolled
trial
in
Switzerland
in
patients
with sickleave
due
to
non-specific non-acuteLBP
to
evaluatethe
effect ofthree
weeks of
function-centered
compared withpain-centered
in-patient
rehabilitationJ'2).
Methods
lnclusion
Criteria
andRandomization
Patients
wereeligible
if
they
werebetween
20
and55
years of age,had
atleast
6
weeks of sickleave
during
the
previeus
6
menthsdue
to
non-acute non-specificLBB
andhad
suficientknowledge
ofGerman
orItalian
to
follow
the
instructions
during
the
physical
assessment,Not
eligiblewere
patients
with cardievascular,pulmonary
orpsychiatric
disease
or other comorbiditythat
would reduce working capacity.A
rheumatologistdetermined
the
eligibitity ofpatients.
Based
onthe
results of an earlier study,four
pre-dTctive
tests
fer
non-returnto
work were used andpatients
with
two
or morepositive
predictive
tests
were excludecl25).Patients
wereincluded
between
January
200e
andMay
2003.
The
study was approvedby
the
ethical committee ofthe
canton of
St
Gallen.
7}'eatment
All
patients
weretreated
sixdays
per
week andthe
length
of stay considered necessary was three weeks.
Independent
teams
oftherapists
were responsiblefor
the
twodifferent
treatments.
Function-Centered
Treatrnent
as71)
All
patients
weretreated
by
a rheurnatologist, aphysical
and eccupational
therapist
trained
in
ergonemics, a spertstherapist,
a soclal worker and a nurse.If
required, aNII-Electronic Library Service
330
mp\fiide\
was
based
on workhardening
andfunctional
restoration
grams.
The
primary
goal
in
the
FT-group
ef4
hrsfday
was
to
increase
work-related capacity.Treatment
emphasized
improving
self-efficacy,defined
as thepatients'
confidencein
their ability to carry out normal activities of
daily
living.
The
rheumatologistinformed
patients
aboutthe
results of
the
imaging
and otherdiagnostic
precedures
as well as about
the
benign
character of non-specificLBP.
Patients
weretold
that
degenerative
changes,if
diagnosed,
were withinthe
mal range
(e,g.
not causingpain
in
the
majority ofpersons).
The
therapist
performed
a werk-related assessment
ing
of ajob
profile
describing
the
physical
demands
and anevatuation of
the
iob-relevant
physical
activities suclt aslifV
ing
and carryingloads,
workingin
abent
position
or
forming
overhead activities.Activities
for
treatment
werechosen
based
onthe
patient's
requiredcapacities
idennfied
in
the
work-related assessment.Treatment
consisted of werksimulation, strength and endurance
training
through
netic exercise, cardiovascular
training
performed
by
walkingand aqua-aerobics, sports
therapy
and self-exercise,Patients
were
told
thatincreasing
activity might cause merepain
because
the
body
had
toget
usedto
the activity again.All
team
members emphasizedthat
patients
should eontinue
therapeutic
aetTvities evenif
pain
increased.
The
treatment
protocol
did
not contain massage,hot-packs
and othersive
treatments
because
these
therapies
were not considered
to
facilitate
anincrease
in
activity and selfeficacy, nordo
the
literature
prove
them
effective.'
Pain-Centered
TVeatment
(Pav
All
patients
weretreated
by
a rheumatologist, aphysical
therapist
and a nurse.If
required, apsychologist
or a socialworker was consulted.
The
primary
goal
in
the
tered
treatmentgroup
{PT-group}
wasto
reducepain,
The
secondary
goal
was toincrease
strength anddecrease
ability.
The
physiotherapist
performed
aphysical
tion to
identify
painful
movements andlimitations
in
ity,
strength and musclelength
in
the
lumbar
region and
lower
extremities,The
duratien
oftreatment
was2
if2
hrsfday
and eonsisted ofindividually
selectedpassive
andactive mobilization, stretching, strength
training
and a mini
back-schoeL
Contrary
to
the
FT-group,
patients
in
the
group
wereteld
to
step activities whenpain
increased.
Passive
pain
modulatingtreatments
such ashot
packs,
trotherapy
or massage were useddaily,
Low
intensity
movement
therapy
in
the
pool
andprogressive
muscleation
further
enhanced relaxation,Progressive
muscleation used systematic contraction and relaxation of specific
muscle
groups,
Patients
were encouragedto
incorporate
relaxation
techniques
into
daily
Iiving
as a coping skillto
reduce stress, muscle
tension
andpain.
ce34kce8e
Outcome
Mbasurements
A
blinded
research assistant(MR)
recorded thework-relat-ed
predictive
factors
andperformed
the
physieal
measure-mentsbefore
and after rehabilitation.The
research assistantwas not
involved
in
anypatient
treatment
in
the
rehabi]i-tation
center.Assessments
wereperformed
in
a separateroom to
prevent
unmasking ofthe
assessor.Patient
ques-tionnaires
were usedto
assess self-efficacy, satisfaction withtreatment
andpain.
Patients
eould notbe
blinded
to
treat-ment
but
allefforts weretaken
to
keep
patients
unaware of any expected advantagein
effectiveness, a conditionthat
is
sometimes called `naive',PrimaTv,
Outeome
The
number ofdays
at work was theprimary
outcome,Each
calendarday
withina
period
at work was counted,leading
te
a maximum of90
days
at workduring
the
3-month
follow-up
period,
This
methodis
insensitive
to
the
fact
that
patients
work atdifferent
days
ofthe
week.Because
a centraldatabase
recording sickleave
does
netexist
in
SwTtzerland,
we assesseddays
at work withques-tionnaires
sentto
the employer andthe
primary
physician
after
three
months.Inconsistencies
were solvedby
additionalphone
callswiththe
persons
involved.
SecondaT),
Outcomes
Self-efficacy,
defined
asthe
patients'
confidencein
their
ability
to
carry out normal activities ofdaily
living,
wasassessed
before
and aftertreatment
withthe
Performance
Assessment
andCapacity
Testing26).
Befere
and afterthe
rehabilitation,the
maximumlifting
capacity was assessed
from
fioor
to waist,from
waist to crown andhorizontally
en waistlevel,
The
researchassis-tant
wastrained
and experiencedin
this
method andthe
reliabiiity
has
been
confirmed27'29).
The
perceived
effect was assessed aftertreatment
and afterthree
months with aquestionnaire
coveringphysical
capacity,
general
well-being and overaUimprovement.
We
used a7-point
Likert
scale30).
Mementary,
maximal and minimalpain
during
the
last
week was rated on an
11-point
Numeric
Rating
Scale
rang-ing
from
O,
`nopain',
to
10,
`theworst
pain
I
canimagine'.
Pain
measurements weretaken
before
and aftertreatment
as well as after
three
months,Before
and aftertreatment
the
following
physical
mea-surements were
performed.
The
finger
to
fioor
distance
was used as a measure of active spinaL andhip
mobilityin
fiex-ion3i),
Spinal
mobilityin
extension was measuredin
degrees
with an
inclinometern2).
Muscle
performance
was assessedby
recordingthe
maximumduration
ofisometric
hip
andtrunk
extension andflexion
againstgravity33),
Functien-
Versus
Pain-Centred
Treatment
Table
1
Comparability
ofthe
of
Low
Back
Pain:
Treatment
Groups
Concepts
andOutcome
atBaseline
331
Function-centered
treatment
group
{n=87)
Pain-centered
treatment
group
(n=87)
Age
(SD}
Gender
(men!women)
Body
Mass
Index
(SD)
Nationality
Switzerland
Italy
Yugoslavia
Bosnia
Macedonia
Croatia
Spain,
Pertugal,
Turkey
Unemployed
CN,
%)
Heavy
work:DOT
>3
{N,
%}
No
professional
education(N,
%}
Mean
days
of sickleave
during
2
years
before
treatment
Seff-efficacy
(PACT,
SD)
Lifting
capacity(kg,
SD}
floor-waist
horizontal
waist-shouldersPain
(NRS
O-10,
SD}
Muscle
performance
(sec.
SD)
Back
extensionFlexion
Finger
tofioor
distance
(cm)
Lumbar
extension(degrees)
(SD)
41.6
(8.4)
1816926.7
(4.2)
38
17
11
5
5
4
7
18
{21)
68
{78}
38
{44}184
{156)11e
{39}15,8
(5,4}2e.4
(7,6)13,2
(4,3)
5.5
{2.0)
3e,4
{32,3)
3e,4
{28,5)
22.8
(13.5)
12,1
(7.6)
42,5
(8,4}
19f6827,2
(4,O}
35
ll
16
6
5
4
9
20
(23)
68
{78)
42
(48)199
{135}102
(42)15,6
(7,3)18.9
(7.8)13,O
(4,8}
5.7
(2.2)
25,9
(25.9)
25,5
(22.8)
26.7
(15.1)
10.6
(6.5)
Stattstical
Analysis
Ana}ysis
wasperformed
by
intention-to-treat.
Between-group
comparisons atbaseline,
aftertreatment
and at3
and12
months offollow-up
wereperformed
with chi-squaretests
for
categorical variables.Independent
samplesT-tests
wereapplied
in
continuous variables with a norrnaldistribution
and a
Mann-Whitney-U
Test
in
nen-parametric continuous variables.Effect
sizes(ES}
were computedfor
alloutcomes.In
continuous variables with a normaldistribution
Cohen's
d
was computedby
clividing
the
meandifference
in
changebetween
thetwo
groups
by
the
standarddeviation
ofthe
change
in
the controlgroup.
If
results were analyzed withthe
generai
Iinear
method, wederived
the
ES
from
eta234).Positive
values ofES's
display
desirable
effects,Effect
sizes of.20
were considered small,.50
were regarded as moder-ate, and.80
were regarded aslarge35).
Statistical
analysis wasperformed
withSPSS
Version
11,5.
Alpha
was set atO,05,
Results
Between
January
lst
2000
andMay
lst
2003,
260
eligiblepatients
were referredto
the
rehabilitation center and174
participated
in
the
study.During
the
treatment
phase
onepatient
ofthe
FT-group
dropped
outbecause
he
was diag-nosed with a necrosis ofthe
head
ofthe
femur
andunder-went surgery.
The
measurements aftertreatment
were missedin
two
patients
from
the
PT-group
due
to
areduc-tion
in
the
length
of stay oi1
and4
days
not noticedby
the
research assistant.The
number ofdays
at work was obtainedin
99%
ofthe
patients
atthree
month and94
%
and97
%
ofthe
patients
in
the
FCT
andPCT
group
respec-tively
at12
month.There
were ne significantdifferences
ofthe
mostimportant
pregnostic
and eutcome variablesbetween
thegroups
after randomization(Table
1).
Adherence
to
andSatisfhction
withthe
Pretocog
The
length
of stay was comparablein
both
groups
with22.2
days
(SD=3.7)
in
the
FT-group
and22.3
days
(SD=3.8)
in
the
PT-group.
All
patients
attended atleast
90%
ofthe
scheduled
treatments.
One
patient
in
theFT-group
was nottreated
according to thepretocol
because
sheinsisted
ongetting
hot
packs
and massagefor
pain
relief,Overall
sat-isfaction
withtreatment,
satisfacrien with advice received,knowledge
about the complaints and theperceived
possibil-ities
to
influence
the
comp!aints werethe
samein
the
two
groups
Tndicating
that
the
effortto
keep
patients
unaware of any expectedtreatment
advantage was successful.Outcome
measurementNII-Electronic Library Service
332
-"fitze
rg34tsas8e
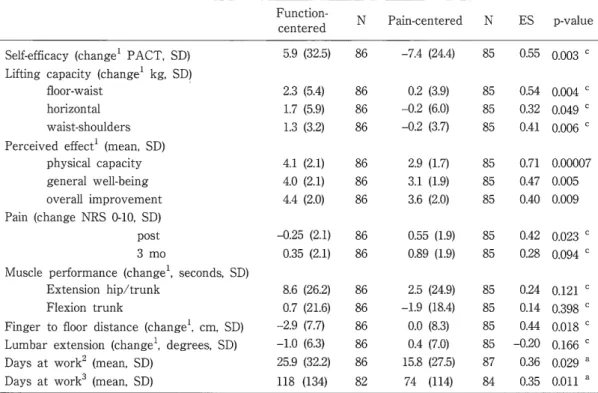
Table
2
Outcome
afterTreatment,
3
and12
Months
(a
Mann-Whitney
U-Test,
bbetween-within
Subjects
ANOVA)
Square
Test,C
Mixed
Function-centeredNPain-centeredNES
p-value
SeLf-ethcacy
{changei
PACT,
SD)
Lifting
capacity{changei
kg,
SD]
fioor-waist
horizontal
waist-shoulders
Perceived
effeeti{mean,
SD)
physical
capacity
general
well-beingoverall
improvement
Pain
(change
NRS
O-10,
SD}
post
3
rnoMuscle
performance
(changei,
seconds,SD)
Extensien
hlpltrunk
Flexion
trunk
Finger
to
floer
distance
(changei,
cm,SD)
Lumbar
extension(changei,
degrees,
SD}
Days
at work2{mean,
SD)
Days
at work3{mean,
SD)
5.9
2.3
1.7
1.3
4,l
4,O
4.4
-O.25
O,35
8.6
O.7-2.9-1.025,9118
(32.5)
(5.4)(5.9)(3.2)
(2.1)(2.1)(2.0)
(2.1)
(2.1)
(26,2)(21.6)(Z7)(6.3)(32.2)(134)
86
868686
868686
8686
868686868682
-7.4
(24.4)
O.2
(3,9)-O.2
(6.0)n2
(3.7)
2.9
(1,n
3.1
(1,9)
3.6
(2.0)
O.55
(1,9)
O.89
(1,9)
2.5
(24.9)
-1.9
(18.4)
O.O
(8,3)
O.4
(7.0)15.8
(27,5)
74
(114)
85
858585
858585
8585
858585858784
O.55
o.oo3
CO.54
o,oo4
eO.32
o.o4g
CO.41
O,O06
[O.71
O.OOO07
O.47
O,O05
O.40
O.O09
O.42
o,o23
CO.28
o,og4
CO.24
O.121
CO.14
O.3gs
CO.44
o,ols
C-O.20
o.166
CO.36
o,o2g
ao.3s
o,oll
aiMeasurement after
treatment
2Measurement after3
effect size
favoring
the
FT
wasfound
for
the
primary
and most of the secondary outcomes.After
3
monthsthere
were moredays
at workin
the
FT
group
compared withthe
PT
group
25.9
vs15.8
(ES
=
O.36,
p
=
O,029)
and after12
monthdays
at work were118
vs74
(ES
O,35,
p=
O.Oll).
Regarding
the
secondary outcomes aftertreatment,
the
FT-group
had
improved
significantly morein
selfefficacy, allthree
tests
for
1ifting
capacity andfor
the
perceived
effectThe
mod-erate effect sizes
for
the
perceived
effect after rehabilitationwere not maintained
during
the
3-month
follow-up
peried.
Pain
intenslty
was significantlylower
in
the
FT-group
after
treatment.
During
the
three-month
follow-up
peried,
pain
increased
in
both
groups
but
the
difference
in
favor
ofthe
FT-group
remained.No
difference
wasfound
in
back
andhip
extensor strength,trunk
fiexor
strength and spinalmobil-ity.
Discussion
This
is
the
first
RCT
in
Switzerland
evaluatingwork-relat-6d
rehabilitationin
patients
withLBP.
work
absence wassignificantly reduced and more
patients
had
returnedto
work after
three
months,The
PT-group
did
not achieve thegoal
ofpain
reduction.Pain
intensity
increased
in
this
group
while
it
decreased
in
the
FT-group.
The
pain
reduetionin
the
FT-group
supportsthe
hypotheses
that
fear
for
pain
may
be
meredisabling
than
pain
itself36).
Compared
with other studies,the
results ofthis
study are remarkablebecause
two
experimentaltreatments
werecom-months, 3Measurement after
12
months.pared
resultingin
a reLatively smalltreatment
contrast,In
a recent review, only one out of nine comparisens
between
two
experimentaltreatments
showed a significant effect24LThe
ES
for
work absencein
this
studyis
similarto
the
ES
in
five
studies comparingintensive
treatment
with usualcare37'4i).
usual
care essentially consisted oftreatment
by
ageneral
physician
giving
advice andprescribing
medications,
Excluding
patients
who will notbenefit
from
treatment
is
essential
to
increase
statisticalpewer
and efficiency of anRCT.
The
positive
results andthe
high
follow-up
ratein
this
study were
in
part
the
result of excludingpatients
withpos-itive
predictive
tests
for
nen-returnto
work,identified
in
aprevlous
study25).In
an attemptto
evaluate whetherexclu-sion was
justified,
we evaluated work absenceby
sendingquestionnaires
and remindersto
the
excludedpatients,
whehad
also attendedthree
weeks of rehabilitation.The
nen-response rate
in
this
group was30%
and only one ofthe
patients
had
returned to work, confirmingthe
value ofthe
predictive
tests.
Although
the
number of workdays
increased
significant-iy
in
the
FT-greup,
the
problem
ofLBP-related
work absence anddisability
is
obviously not solved.Considering
the remaining amount of work absencein
the
FT-group,
the
effect of
the
FT
treatment
canbe
considereddisappointing
andtoo
smalLThe
investigated
greup,
however,
is
charac-terizecl
by
Iong-standing
sickleave,
heavy
work andlow
edu-cation resultingin
alimited
possibiLlty
to reduce workdemands.
Return
to
workis
additionallylimited
because
less
Function-
Versus
Pain-Centred
Treatment
ofdemanding
jobs
arehardly
available onthe
employmentmar-ket,
Only
two
patients
found
a newjob.
Knowledge
ofthe
Swiss
nationallanguages
waslimited
in
morethan
50%
ofthe
patients
participating
in
our workrehabilitation
program
Treatment
wasdeveloped
to
be
applicable
te
these
patients.
The
key
element ofthe
FT
treatment was activity effered as
isokinetlc
andwerk-relat-ed training, walking and sports
therapy,
This
treatment
did
not need
proficient
verbal eommunication and couldbe
appliedto
this
greup
ofpatients,
increasing
the
external validity ofthe
study.
The
external validity ofthis
studyis
further
supportedby
the
patient
population,
representativefor
patients
in
SwitzerEand
withLBP,
who are at risk ofpermanentiy
los-ing
working capacity,becoming
unemployed orbecoming
dependent
on adisability
allowance.The
majority ofthe
patients
wereheavy
workersborn
in
other eountries,poor-ly
educated andhaving
insufficient
personal
resources,par-ticularly
insufficient
knowledge
ofthe
Swiss
nationallan-guages,
to
participate
successfullyin
vocational measures.other
studies 3S'40' 42'43) onlyincluded
patients withproficient
knowledge
of the nationaltanguage,
giving
them
abetter
perspeetive
to
participate
in
vocational measures andto
find
lighter
work.Assessments
in
this
studyhad
to
be
eitheravailable
in
allrequiredlanguages
orbe
independent
oflan-guage,
The
PACT
selfefficacy assessmentdoes
not requireproficient
knowledge
oflanguage
because
it
usespictures
efphysical
activlties.
Conclusion
Function-centered
rehabilitationdecreases
work-relateddisability.
The
effect sizes were smallto
moderate.The
num-ber
ofdays
at workduring
the
three
months offollow-up
was
10
days
higher
in
the
FT-group
and44
days
higher
after
12
months.Selfefficacy,
lifting
capacity andpain
inten-sity
impreved
significantlyin
the
FT-group.
The
number ofdays
at workdid
notdepend
on sex, age, workload andnationality.
Function-celltered
treatment
shouldbe
usedinstead
ofthe
still widespreadpain-centered
treatments,
References
O
Kool
JP,
Bachmann
S,
et al./Function-centred
rehabilitationincreases
werkdays
in
patients
wlth non-acute non-specific lowback
pain/one-year resuttsfrom
a randomised controlledtrial,
2006
CSubmitted
for
Publication},
2)
Kool
JP,
Oeseh
PR,
et al;Increasing
clays
at work usingtion-centered rehabilitation
in
nonacute nonspecificIow
back
pain/
arandomized controLLed
triaL
Arch
Phys
Med
Rehabil
86/
857-64,
2005.
3)
Murphy
PL,
Volinn
E/
Is
occupationallow
back
pain on therise?
Spine
24/
691-697.
1999.
4)
Lee
P/
The
economicimpact
ofmusculoskeletaldisorders.
Qual
Life
Res
3/
S85-S91,
1994,
5)
Williams
DA,
Feuerstein
M,
et ai./Health
care andindemnity
costs across the nazural
history
ofdisabitity
in
occupationallow
Low
6)7}
8)
9)
10)
11)
12)
13)
14)
15)
16)
17)18) 19)20)
2D22)
23)
24)
25)
26) 27)28)
29)Back
Pain:
Concepts
andOutcome
333
baek
pain.Spine
23/2329-2336, 1998.BSV,
IV-Statistik
2003,Bundesamt
fur
Sozialversicherungen,
Bern,
2003.
Leuenberger
M,
Huber-Hotz
A/
Botschaft
Uber
die
4.
Revision
des
Bundesgesetzes
Uber
die
Invalidenversicherung,
20el.
Fordyce
WE/Back
Pain
in
the
WorkpLace/
Management
oiDisability
in
Nonspecific
Co"ditiolls,
IASP
Press,
Seattle,
1995.
Frymoyer
JW,
Cats-Baril
WL/
An
overview oftheincidences
andcosts of
Iow
back
pain,Orthop
Clin
North
Arn
22/
263-271,
1991.
Cherkin
DC,
Deyo
RA,
et al,/Physician
variatiollin
diagnostic
testing
for
low
back
pain.Who
you seeis
what you getArthritis
Rheum
37:
15-22,
1994.
Nachemson
A,
Vingard
E/
Assessment
of patients with neck andLow
back
painIn/
Nachemson
A,
Jonsson
E
(eds}
Neck
andBack
Pain-The
Scientific
Evidence
ofCauses,
Diagnosis,
andTreatment,
Lippincott
Williams
&
Wilkins,
Philadelphia,
2000, pp]89-236.Kendrick
D,
Fielding
K,
et al./Radiography
of thelumbar
spinein
primary
carepatients
withlow
back
pain/
randomisedcon-trolled
trial.
BMJ
322/
400-405,
2001,
van
Tulder
MW,
Assendelft
WJ,
etal:SpinaL
radiographicfind-ings and nonspecific low
back
paTn,
A systematie review ofobser-vational studies,
Spine
22:
427-434,
]997.
Abenhaim
L,
Ressignol
M,
et al:The
role of activityin
the ther-apeutic management ofback
pain,Repert
of theInternational
Paris
Ta$k
Force
enBack
Pain.
Spine
25/
IS-33S,
2eOO.
Ostelo
RW,
de
Vet
HC,
et al,/Rehabilitation
following
first-time
lurnbar
disc
surgery/ a systematic review within theframewerk
of the cochrane collaboration.
Spine
28/
209-218,
2003.
Rainvllle
J,
Cartson
N,
et al:Exptoration
of physieians'recom-mendations
for
activitiesin
chroniclow
back
pain.Spine
25/
2210-2220,
2000.
Waddetl
G/
The
Back
Pain
Revoiution.
ChurehM
Livingstone,Edinburgh,
l998,pp223-24e.Matheson
LN,
Ogden
LD,
et al,/Werk
hardening/
occupationattherapy
in
industrial
rehabilitatlon.Arn
J
Occup
Ther
39/
314-321,
]985,Mayer
TG,
Gatchel
RJ/ FunctionaL Restoration forSpinal
Disorders/
The
Sports
Medicine
Approach.
Philaclelphia,Lea&
Febiger,
l991.Guzman
J,
Esmai1
R
et al:Multidiscipiinary
rehabiEitationfor
chronicIow
back
pain/
systematic review.BMJ
322/
1511-1516,
2001.Brox
JI,
Hagen
KB,
etal:Is
exercisetherapy
and manipulationeffective in lew
baek
pain? Tidsskr NorLaegeforen
119/
2042-2050,
1999,
van
der
Weide
WE,
Verbeek
JH,
et al,/Vocatiomal
outcome ofintervention
for
Low-back
pain.
Scancl
J
Work
Environ
Health
23/
t65-178,
1997.
Schonstein
E,
Kenny,
DT
et al./Werk
conditioning, workhard-ening and
functional
restorationfor
workers withback
and neckpain
(Cochrane
Review}.
Cochrane
Dazabase
Syst
Rev/
CDOO1822,
2003,KooL
J,
de
Bie
R,
et al,/Exercise
reduces sickleave
in
patientswith non-acute non-specific
low
back
paln/ a meta-analysis.J
Rehabil
Med
36/
49-62,
2004.
Kool
JP,
Oesch
PR,
et al./Predictive
test$for
non-return teworkin
patients with chroniclow
back
pain.Eur
Spine
J
11:
258-266,
2002.Matheson
LN,
Matheson
M/
Spinal
function
sort,rating ofper-ceived capacity.
Performance
Assessment
andCapacity
Testing
PACT,
Trabuco
Canyon,
California/
Performance
Assessrment
andCapaciry
Testing
PACT, 1989.Gross
DP,
Battie
MC/
Reliability
of safe maximumlifting
deter-minations of a
functional
capacity evaluation, Phys Ther82/
364-371, 2002.
Isernhagen
SJ,
Hart
DL,
etal:ReliabiEity
ofindependent
observ-erjudgments
oflevelof lifteffortin a kinesiophysical function-alcapacity evaluation.Work
12/
145-150,
1999.
Brouwer
S,
Reneman M, et al: Test-retest re!iabilitv ofthe
Isernhagen
work systemsiunctional
capacity evaluationin
NII-Electronic Library Service
334
mp#ut?ft#
patients with chronie Low
back
pain.J
Occup
Rehabil 13,208-218,2003.
30)
Beurskens
AJ,
de
Vet
HC,
et ai:Responsiveness
offunctional
status
in
low
back
pain/
a comparison ofdifEerent
instruments.
Pain
65/
71-76,
1996.
31)
HeikkTlaS,
ViitanenJV,
et at,/Sensitivity
to
change of mebility tests;effect of shert termintensive
physiotherapy and exerciseon spinal,
hip,
alld shoulder measurementsin
thy.
J
Rheumatol
27/
1251-1256,
2000.
32}
Ng
JK,
Kippers
V.
etal./Range
of motion andlordosis
ofthe
lumbar
spine/ reliabilityof measurement and normative values.
Spine
26/53-60,
2eOl,
33)
Oesch
P,
Kool
JP,
etal:Die
Zuverlassigkeit
unclEmpfindlichkeit
von
4
isometrischen
Muskeltests.
Physiotherapie
6/
4-]2,
1994.
34)
Rosenthal
R/
Parametric
measures ofeffect size,In:
Ceoper
H,
Heclges
L
{eds)
The
Handboolc
ofResearch
Synthesis.
Ru$selL
Sage
Foundation,
New
York,
1994,
pp231-244.
35)
Cohen
J:
Statistical
power analysisfor
thebehavioral
scTences,
2nd.
Lawrence
Erlbaum,
New
Jersey,
1988.
36)
Vlaeyen
JW,
de
Jong
J,
et al./The
treatment offear
ofmentf(re)injury
in
chroniclow
back
pain/further
evidence onthe effectiveness of exposure
in
vivo,Clin
J
?ain
18:
251-261,
2002.
37)
Hagen
KB,
HoLte
HH,
et al:Socioeconomic
facters
andty retirernent
from
back
pain/ a1983-1993
population-basedeg34tseg8e
prospective study inNorway.
Spine
25/2480-2487,2000.
38)
Skouen
JS,
Grasdal
AL,
et al:Retative
cost-effectiveness ofsive and
light
multidisciplinary treatmentprograms
versusment as usual
for
patients
with chronicIow
back
pain
on
term
sickleave/
randomized controLled study,Spine
27/9el-909,
2002.
39)
TorstensenTA,
LjLtnggren
AE,
et al:Efficiency
and costs ofmedical exercise therapy, conventional
physietherapy,
andexercise
in
patients
with chroniclow
back
pain.
A
pragmatic,
randomized, singte-blinded,controlled
trial
with1-year
follow-up.
Spine
23,
2616-2624.
]998.
40)
Lindstr6m
I,
Ohlund
C,
et al: The effectofgracled
activity onpatients with subacute
low
back
pain:
arandomizedprospeetive
clinical study with an eperant-conditioning
behavioral
approaeh,Phys
Ther
72/
279-290,
1992,
41)
Bendix
AF,
Bendix
T,
et al:Multidisciplinary
intensive
ment
for
chroniclow
back
pain/a randomized, prospective study.
Cleve
Clin
J
Med
63:
62-69,
1996.
42)
Torstensen
TA,
Koes
B,
et al./The
effect of conservative apies on patients sufferingfrom
chronic]ow
back
pain,Spine
21/
656-657,
1996.
43)
Bendix
AE
Bendix
T,
et al:Active
treatment programsfor
patients with chroniclow
back
pain/a prospectTve, randornTzed,observer-blinded study,