放射線被曝と癌の関係(131119)
ここでは、医療被曝のような、急激に被曝する場合を想定して考えていきたいと思う。(自然放射 線や原発事故の影響のある地域のような、少量で慢性的に受ける被曝についてはここでは当て はまらない可能性があるため。) 自分の不完全な知識としては、「放射線により損傷を受けた DNA は修復されるが、必ずしも完全 に修復されないこともあり、それが繰り返されることにより癌化する可能性が増大する。」なんてこ とぐらいだが、間違っていたら教えてほしい・・・。急激に大量に受けた損傷ほど修復されにくいこと や、損傷を繰り返し受けたなら、不完全に修復された DNA が蓄積することで、問題が生じるという ことはイメージとしてつかみやすい。 メルクマールになりそうな論文のいくつかを見てみる。 文献 1、2、3 は被爆者のデータ。もとの論文を入手できなかったので、抄録と対応する別論文な どの図表を眺めてみることにした。 文献 1 によると、0∼150mSV の被曝でも固形癌のリスクが増す可能性を指摘している。We estimate that about 440 (5%) of the solid cancer deaths and 250 (0.8%) of the noncancer deaths were associated with the radiation exposure. The excess solid cancer risks appear to be linear in dose even for doses in the 0 to 150-mSv range. While excess rates for radiation-related cancers increase throughout the study period, a new finding is that relative risks decline with increasing attained age, as well as being highest for those exposed as children as noted previously. A useful representative value is that for those exposed at age 30 the solid cancer risk is elevated by 47% per sievert at age 70.
文献 2 では 5mSv 以上の被曝が癌の発生と関連している可能性を指摘している。
For all solid cancers as a group, it was estimated that about 850 (about 11%) of the cases among cohort members with colon doses in excess of 0.005 Gy were associated with atomic bomb radiation exposure. The data were consistent with a linear dose response over the 0- to 2-Gy range, while there was some flattening of the dose response at higher doses. Furthermore, there is a statistically significant dose response when analyses were limited to cohort members with doses
of 0.15 Gy or less.
Radiation Effects Research Foundation のホームページに、文献 1、2 のデータをもとにした図表 が記載されている。これを見ると、被爆者のように急激な被曝を受けた場合には、少量の線量で もリスクが増大するように思える。しきい値は無い。もちろん、リスクが増すといっても、その大きさ を考慮する必要がある。リスクの大きさを無視した過剰な心配はむしろ有害にさえなると思う。医 療被曝のように管理された被曝であれば、そのリスクの絶対値は少ないケースがほとんどだと思 う。それでも、根拠もなく「問題ない」と説明したり、医療被曝について「意識をしない」というのはプ ロフェッショナルとしては通用しない。
Table. Excess risk of developing solid cancers in LSS, 1958-1998
Weighted colon dose (Gy) LSS subjects Cancers Attributable risk Observed Estimated excess
0.005 - 0.1 27,789 4,406 81 1.80% 0.1 - 0.2 5,527 968 75 7.60% 0.2 - 0.5 5,935 1,144 179 15.70% 0.5 - 1.0 3,173 688 206 29.50% 1.0 - 2.0 1,647 460 196 44.20% >2.0 564 185 111 61.00% Total 44,635 7,851 848 10.70% (参考文献 6 より引用)
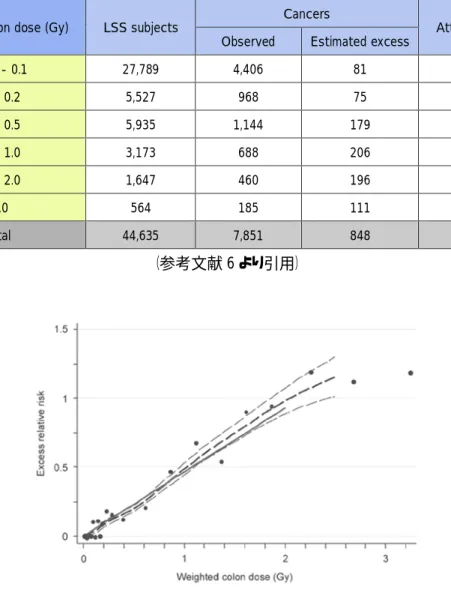
Figure 1. LSS solid cancer incidence, excess relative risk by radiation dose, 1958-1998. The thick solid line is the fitted linear sex-averaged excess relative risk (ERR) dose response at age 70 after exposure at age 30. The thick dashed line is a non-parametric smoothed estimate of the dose category-specific
risks and the thin dashed lines are one standard error above and below this smoothed estimate. (参考文献 6 より引用)
文献 3 も 0∼0.1Sv の少量の被曝でも癌のリスクが増すことを示している。
There is a statistically significant risk in the range 0-0.1 Sv, and an upper confidence limit on any possible threshold is computed as 0.06 Sv. It is indicated that modification of the neutron dose estimates currently under consideration would not markedly change the conclusions.
この論文のデータをもとにした図が文献 4 に記載されていた。これを見ても、線量が少ないから 影響がないとは言えない。線量が少なくても癌リスクの増加はあるととらえるのが普通だ。ただ、 常識的な医療被曝であれば、そのリスクは極めて小さいと考えるのが妥当だ。必要性を無視して、 造影 CT を毎年何度も受けるような馬鹿げた被曝はかなり問題だと思うが・・・。例えば単純 CT を 1 回受けて 10mSv、造影をするともう 1 回で 20mSv だとする。1 年に 4∼5 回撮影して 5 年続けた とすると、これだけであっという間に 400mSv∼500mSv(0.4∼0.5 Sv)になる。
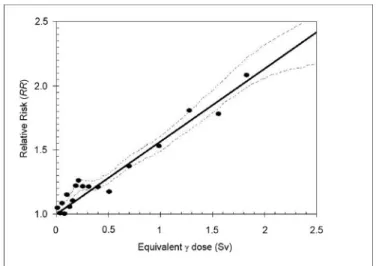
Figure 4: Illustration of the relationship between dose and relative risk, based on data from the atomic bomb survivor cohort; adapted from Pierce and Preston (2000).[21]Note in particular that the extension
to low doses (<0.5 Sv), whilst consistent with a linear fit, appears to underestimate the relative risk (参考文献 4 より引用)
放射性作業従事者は、被曝線量が精確に管理されている。文献 5 は平均 19.4mSv の被曝を 認める放射線作業従事者のデータ。100mSv あたり、白血病を除く癌による死亡リスクは 9.7%ず つ増加すると報告されている。この研究の対象になった集団でも 1∼2%の癌による死亡が放射 線の被曝によるものと推定している。
The excess relative risk for cancers other than leukaemia was 0.97 per Sv, 95% confidence interval 0.14 to 1.97. Analyses of causes of death related or unrelated to smoking indicate that, although confounding by smoking may be present, it is unlikely to explain all of this increased risk. The excess relative risk for leukaemia excluding chronic lymphocytic leukaemia was 1.93 per Sv ( < 0 to 8.47). On the basis of these estimates, 1-2% of deaths from cancer among workers in this cohort may be attributable to radiation.
The overall average cumulative recorded dose was 19.4 mSv.
Our estimates suggest that a cumulative exposure of 100 mSv would lead to a 9.7% (1.4 to 19.7%) increased mortality from all cancers excluding leukaemia and a 5.9% ( -2.9 to 17.0%) increased mortality from all cancers excluding leukaemia, lung, and pleura compared with background rates. The corresponding figure is 19% ( < 0 to 84.7%) for mortality from leukaemia excluding chronic lymphocytic leukaemia.
(参考文献 5 より引用)
(参考文献 5 より引用)
量被曝なのだから、むしろ 100mSv までの間の被曝量と癌のリスクの直線的な関係を示したグラフ が示されるとスッキリするのだけれど・・・。他の論文のように、これを明示しないのには理由があ るのだろうか。この点は少量の被曝の影響はハッキリしないといわれる隙を与えているような気が する。(気づいていないだけかもしれないので、詳細が分かる人がいたら教えてほしい・・・) そもそも、しきい値が無いことを認めるなら結論は単純。不要なリスクはあるより無い方がいいに 決まっている。CT を撮らなかったばかりに失敗した経験もあるので、何とも説得力がないが、「取 り敢えず CT」というのもやはり慎むべきなのだと思う。 参考文献
1. Preston DL, Shimizu Y, Pierce DA, Suyama A, Mabuchi K. Studies of mortality of atomic bomb survivors. Report 13: Solid cancer and noncancer disease mortality: 1950-1997. Radiat Res. 2003 Oct;160(4):381-407. PubMed PMID: 12968934.
2. Preston DL, Ron E, Tokuoka S, Funamoto S, Nishi N, Soda M, Mabuchi K, Kodama K. Solid cancer incidence in atomic bomb survivors: 1958-1998. Radiat Res. 2007 Jul;168(1):1-64. PubMed PMID: 17722996.
3. Pierce DA, Preston DL. Radiation-related cancer risks at low doses among atomic bomb survivors. Radiat Res. 2000 Aug;154(2):178-86. PubMed PMID: 10931690.
4. Taylor ML, Kron T. Consideration of the radiation dose delivered away from the treatment field to patients in radiotherapy. J Med Phys. 2011 Apr;36(2):59-71. doi: 10.4103/0971-6203.79686. PubMed PMID: 21731221; PubMed Central PMCID:PMC3119954. 5. Cardis E, Vrijheid M, Blettner M, Gilbert E, Hakama M, Hill C, Howe G, Kaldor J, Muirhead CR,
Schubauer-Berigan M, Yoshimura T, Bermann F, Cowper G, Fix J, Hacker C, Heinmiller B, Marshall M, Thierry-Chef I, Utterback D, Ahn YO, Amoros E, Ashmore P, Auvinen A, Bae JM, Solano JB, Biau A, Combalot E, Deboodt P, Diez Sacristan A, Eklof M, Engels H, Engholm G, Gulis G, Habib R, Holan K, Hyvonen H, Kerekes A, Kurtinaitis J, Malker H, Martuzzi M, Mastauskas A, Monnet A, Moser M, Pearce MS, Richardson DB, Rodriguez-Artalejo F, Rogel A, Tardy H, Telle-Lamberton M, Turai I, Usel M, Veress K. Risk of cancer after low doses of ionizing radiation: retrospective cohort study in 15 countries. BMJ. 2005 Jul 9;331(7508):77. Epub 2005 Jun 29. PubMed PMID: 15987704; PubMed Central PMCID: PMC558612.
6. Solid cancer risks among atomic-bomb survivors. Radiation Effects Research Foundation ホ ームページ http://www.rerf.jp/radefx/late_e/cancrisk.html