T
/NK 細胞リンパ腫ガイドライン
鈴 木 律 朗
Key words : T-cell lymphoma, NK-cell lymphoma, CHOP, SMILE
緒
言
「悪性リンパ腫の分類は,正常由来細胞に基づくべき である」とする REAL/WHO 分類の考え方は定着し, WHO分類第 4 版(2008)には現在 23 の成熟 T/NK 細 胞腫瘍がリストアップされている1)。これらすべての病 型で別々の対応が必要ではないが,かと言って画一的な 対応でも不都合がある。T/NK 細胞リンパ腫は,未分化 大 細 胞 型 リ ン パ 腫(anaplastic large cell lymphoma, ALCL)を除いて B 細胞リンパ腫より予後不良とされて きたが2, 3),CD20 抗体製剤 rituximab の登場以降予後の 差は拡大しており,B 細胞リンパ腫とは全く異なる診療 体系が必要である。米国では National Comprehensive Cancer Network (NCCN)によるガイドラインが 2003 年から公開されて,毎年アップデートされている4)。本 邦でも皮膚 T 細胞リンパ腫に関するガイドラインが日 本皮膚科学会などにより作成されている5)。日本血液学 会では「造血器腫瘍ガイドライン」を作成することにな り,本稿では T/NK 細胞リンパ腫について解説する。対象と分類
米国ネブラスカ大が中心となって,世界中から T/NK 細胞リンパ腫を調査した International T-cell Lymphoma Project(iTCLP)は 1,153 例とこれまでに最多の症例数 を集めた国際共同研究であった6)。日本や東アジア諸国 の症例も含まれるため,節外性 NK/T 細胞リンパ腫, 鼻 型(ENKL)お よ び 成 人 T 細 胞 白 血 病 /リ ン パ 腫 (ATLL)といった,欧米白人では極めて少ない病型の一 定の割合を占めている。一方,本邦では,B 細胞リンパ 腫も含めた 3,000 例の調査研究が 2000 年に公表されて い る7)。こ の 研 究 で は,未 分 化 大 細 胞 型 リ ン パ 腫 (ALCL)を ALK の陽性/陰性で分けていないなど,直接 の比較は困難ではあるが,ATLL を除いた主要病型の割 合を Fig. 1 に示す。日本では,血管免疫芽球性 T 細胞 リンパ腫(AITL)と腸症関連 T 細胞リンパ腫(EATL) の相対的頻度が低く,一方で PTCL,非特定(PTCL-NOS)および ENKL の相対的頻度は高い。 いずれでも,次の 6 つが多数病型として挙がってい る。 ・PTCL,非特定(PTCL-NOS) ・血管免疫芽球性 T 細胞リンパ腫(AITL) ・節外性 NK/T 細胞リンパ腫,鼻型(ENKL) 名古屋大学大学院医学系研究科 造血細胞移植情報管理・生物 統計学 第 75 回日本血液学会学術集会 リンパ系腫瘍:ALL/ML EL-27 ガイドライン(標準治療)Fig. 1 Distribution of subtypes in T/NK-cell lymphoma Figures show the relative percentage of each subtype excluding adult T-cell leukemia/lymphoma (ATLL). International T-cell Lymphoma Project (iTCLP) data also contain Japanese data. The incidences of AITL and ALCL are lower in Japan. In contrast, the incidences of PTCL-NOS and ENKL are higher.
・成人 T 細胞白血病/リンパ腫(ATLL)
・ALK 陽性未分化大細胞型リンパ腫(ALK+ ALCL) ・ALK 陰性未分化大細胞型リンパ腫(ALK, ALCL) ATLLについては別稿で扱い,本稿ではそれ以外の 5 病型を対象とする。疾患別の推奨される 初回治療を Table 1に,造血幹細胞移植の位置づけを Table 2 に示 す。
ALK
陽性 ALCL
ALCLは独特の anaplastic と呼ばれる腫瘍細胞が増殖 する節性リンパ腫で,もともとは形態的に定義された8)。 細胞傷害性分子が発現するエフェクター T 細胞の腫瘍 である。特徴的な t(2;5)(p23;q35)転座から NPM-ALK 融合遺伝子がクローニングされ,通常リンパ系細胞では 発現しない ALK のキナーゼ活性が腫瘍化に関与している9, 10)。ALK 陽性 ALCL の臨床像は ALK 陰性 ALCL と
は全く異なり,現在は別病型とされている11)。ALK 陽 性 ALCL の発症年齢中央値は 20 歳前後で,主要リンパ 腫病型の中では B 細胞リンパ腫まで含めても最も若年 発症である12∼14)。 70%前後が進行期例であるが,CHOP 療法などの an-thracyclineを含む化学療法で予後は良好である12, 13)。こ のため,比較試験は存在しないが同療法が推奨される。 初回治療で完全または部分奏効が得られた例に対する, 地固めとしての自家または同種造血幹細胞移植は,行う べきでない。限局期例に関する情報は少ないが,化学療 法後の放射線療法が推奨される。
PTCL-NOS
,AITL,ALK 陰性 ALCL
PTCL-NOSは T/NK 細胞リンパ腫の最大病型である
Table 1 Recommended treatment for each subtype of T/NK-cell lymphoma
Subtype Limited stage Extensive stage
ALK+ ALCL CHOP×3 courses followed by radiotherapy CHOP×6 to 8 courses
PTCL-NOS
Chemotherapy(*)followed by radiotherapy
Clinical trial
Chemotherapy(*)
Clinical trial AITL
ALK− ALCL
ENKL Concurrent or sequential radiotherapy and
chemotherapy SMILE chemotherapy
* No superior regimen of chemotherapy is evidenced. CHOP can be an option, but other
regimens are permitted.
** For other subtypes not in this list, no recommendation can be made because of the lack of
evidences.
Abbreviations: ALCL, anaplastic large cell lymphoma; PTCL-NOS, peripheral T-cell lymphoma, not otherwise specifi ed; AITL, angio-immunoblastic T-cell lymphoma; ENKL, extranodal NK/ T-cell lymphoma, nasal type
Table 2 Hematopoietic stem cell transplantation for frontline treatment of T/NK-cell lymphoma
Subtype Limited stage Extensive stage
ALK+ ALCL Not recommended. Not recommended.
PTCL-NOS
No information Recommended as clinical trials.
Not recommended for clinical practice. AITL
ALK− ALCL
ENKL Not recommended.
Recommended.
Allogeneic transplant if suitable donor exists. Autologous transplant is an option for all patients. Abbreviations: ALCL, anaplastic large cell lymphoma; PTCL-NOS, peripheral T-cell lymphoma, not otherwise specifi ed; AITL, angio-immunoblastic T-cell lymphoma; ENKL, extranodal NK/ T-cell lymphoma, nasal type
が,B 細胞リンパ腫におけるびまん性大細胞型 B 細胞 リンパ腫と同様にヘテロな集団である15)。節性・節外性 リンパ腫の双方を含み,細胞傷害性分子の発現や16), Epstein-Barrウイルスの有無など多くの臨床病理学的 マーカーが不均質である。AITL は節性リンパ腫で,高 内皮細静脈や濾胞樹状細胞の樹枝状増殖を特徴とす る17)。細胞傷害性分子は基本的に陰性の,濾胞 T 細胞
由 来 の 腫 瘍 で あ る18)。ALK 陰 性 ALCL は,ALK 陽 性
ALCLと同様の形態と表現型を持つ節性リンパ腫で,細 胞傷害性分子も陽性となる11)。PTCL における病期分類
は,ほかの非ホジキンリンパ腫と同様に Ann Arbor 分 類が用いられ,予後予測モデルとしては国際予後指標 (International prognostic index,IPI)が有用である19)。
PTCL-NOSに関してはイタリアの研究グループから提 唱された予後予測モデルである PIT (Prognostic Index for PTCL-U)がある20)。PIT では,年齢,performance status,血清 LDH 値,骨髄浸潤陽性の 4 因子で規定さ れるが,最近発表された ESMO ガイドラインでは IPI の使用を推奨している21)。PTCL に対する効果判定規準
と し て は,効 果 判 定 に positron emission tomography (PET)を組み込んだ改訂国際ワークショップ基準22)が
推奨される。この基準も,あいまいな点を明確にする再 改訂が近く予定されている。
これら 3 病型の T 細胞性リンパ腫は,形態は違うが 予後や臨床病態は共通点があり,治療方針も同じであ る。International T-Cell Lymphoma Project で示されたよ うに CHOP 療法などの anthracycline を含む治療の優位 性はないが,これを凌駕する治療法がないのも事実であ る6)。標準治療は存在しないが CHOP 療法のほか23),
etoposideを加えた CHOEP 療法24),CHOP+ICE のよ
うな白金製剤を加えたレジメン25)が選択肢となる。臨 床試験への参加も,同様に選択肢となり得る。 初回治療における完全または部分奏効例に対して,地 固め療法として自家造血細胞移植を行う単アームの臨床 試験がいくつか報告されている26∼28)。2012 年の北欧か らの報告は参加者数も多く成績も良好であるが28),既存 の過去の試験との線引きも明瞭でない。無作為化比較試 験のない現状では,初発症例における造血幹細胞移植は 一般診療としては推奨されず,臨床試験として実施すべ きである。初回治療で部分奏効が得られない場合,治療 選択に関するエビデンスは乏しい。臨床試験および新規 薬剤,造血幹細胞移植が実施されているのが現状であ る。
ENKL
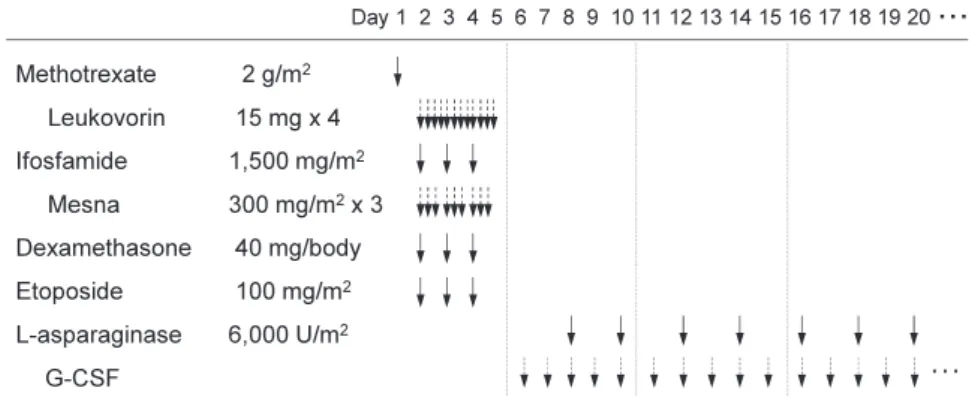
鼻腔周囲を好発部位とする節外性リンパ腫で,ほとん どは NK 細胞由来である29)。一部に細胞傷害性 T 細胞 由来のリンパ腫もあるが,パラフィン標本で正確に NK 細胞型と T 細胞型を鑑別することが困難であることか ら,“NK/T”という用語により「節外性 NK/T 細胞リ ン パ 腫,鼻 型(extranodal NK/T-cell lymphoma,nasal type)」という病型名称になっている30)。リンパ腫細胞 中に Epstein-Barr ウイルス(EBV)が存在することから, EBVの存在が診断の一助になっている。NK 細胞型・T 細胞型のいずれでも細胞傷害性分子は陽性となる31)。 NK細胞型と T 細胞型の識別はフローサイトメトリーあ るいは T 細胞受容体再構成の遺伝子解析で可能である ため,十分な検体量を採取困難な鼻咽頭以外の原発例で は識別可能なことが多い。細胞型によって予後が異なる という報告もあるため32∼34),可能であれば鑑別が推奨 される。病期分類には,ほかの悪性リンパ腫と同様に Ann Arbor分類が用いられているが,節外性リンパ腫に この分類をあてはめることの問題点もある。ENKL では 約 70%が限局期である35∼37)。日本37)および韓国36)から 予後予測モデルがそれぞれ提唱されている。他のリンパ 腫と異なり診断時年齢は予後因子とならない。治療効果 の判定に際しては,特に鼻腔周辺は解剖学的に複雑であ ること,腫瘍が消失しても粘膜肥厚などの非腫瘍組織の 残存がありうること,ENKL では positron emission to-mography (PET)において高率に18fluoro-2-deoxyglucose(FDG)の取り込みが認められることから38),FDG-PET が有用である。末梢血中 EBV-DNA 断片が腫瘍量を反映 することが知られており39),予後予測や有害事象の予測 にも有用であるが40, 41),本邦ではまだ保険承認されてい ない。 ENKLは放射線感受性が高いため,限局期例では放射 線療法を組み込む。腫瘍細胞は,正常 NK 細胞とともに 多剤薬剤耐性(multi-drug resistance,MDR)に関係す る P 糖蛋白を発現している42∼44)。ドキソルビシン,ビ ンクリスチン,エトポシドなどの抗腫瘍薬剤は短時間で 細胞外に排出されるため,CHOP 療法の有効性は低 い37)。日本および韓国から,同時化学放射線療法の良好 な臨床試験結果が報告されており,推奨される治療であ る45, 46)。比較試験がなされていないため,放射線療法先 行後の化学療法も選択肢の一つである47)。2008 年に発 表された日本・韓国・台湾からの matched pair 解析で は,限局期高リスク例で初回完全奏効(CR)後の自家 造血幹細胞移植の有用性を示しているが48),その後の治 療戦略の進歩により予後は改善してきており,限局期例 では初回治療時の造血幹細胞移植は推奨されない。 進行期例では,MDR 関連 P 糖蛋白の影響を受けない 薬剤を主体とする SMILE 療法が推奨される(Fig. 2)49)。
GELA/GOELAMS による初回再発/治療抵抗性 ENKL を 対象とした AspaMetDex 療法(L-asp,MTX,DMS)も
報告されているが50),限局期例や CHOP 療法後の再発 例が多く本邦の現実と合致しない。治療強度および再現 性 の 観 点 か ら も,SMILE 療 法 の 方 が 推 奨 さ れ る 。 SMILE療法で完全または部分奏効が得られた場合,患 者の年齢や全身状態が問題なければ造血幹細胞移植の実 施が推奨される29)。自家移植か同種移植かの選択に関し ては,本邦の後方視的解析ではいずれの移植でも遜色は ないことが示されている51)。
その他の病型
頻度が低いその他の T/NK 細胞リンパ腫には腸管症 関連 T 細胞リンパ腫(enteropathy-associated T-cell lym-phoma,EATL)52),肝脾 T 細胞リンパ腫(hepatosplenicT-cell lymphoma,HSTL)53)が あ る 。EATL は Celiac 病 の頻度の高い欧米では相対頻度が高いが,本邦では少な くほとんどが Celiac 病と関係ない type II である。HSTL は gamma/delta 型 T 細胞由来のものが多いが alpha/ beta型も含まれ,若年男性に多く,著明な肝脾腫を特 徴とする。EATL,HSTL ともに CHOP 療法など既存の 化学療法での予後は不良である。皮膚原発 ALCL,皮下 脂肪織炎様 T 細胞リンパ腫は,皮膚/皮下組織を主な病 変部位とするリンパ腫で,予後は良好である。 著者の COI(conflicts of interest)開示:鈴木律朗;寄付講座(造 血細胞移植学会) 文 献
1)Swerdlow SH, Campo E, Harris NL, et al. eds. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Fourth Edition, Lyon, IARC Press; 2008.
2)A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin>s lymphoma. The Non-Hodgkin>s Lymphoma Classification Project. Blood. 1997; 89: 3909-3918.
3)Gisselbrecht C, Gaulard P, Lepage E, et al. Prognostic signifi-cance of T-cell phenotype in aggressive non-Hodgkin>s lym-phomas. Groupe d>Etudes des Lymphomes de l>Adulte (GELA). Blood. 1998; 92: 76-82.
4)Zelenetz AD, Wierda WG, Abramson JS, et al. Non-Hodgkin>s Lymphomas, version 3.2012. J Natl Compr Canc Netw. 2012; 10: 1487-1498.
5)Sugaya M, Hamada T, Kawai K, et al. Guidelines for the management of cutaneous lymphomas(2011): A consensus statement by the Japanese Skin Cancer Society - Lymphoma Study Group. J Dermatol. 2013; 40: 2-14.
6)Vose J, Armitage J, Weisenburger D; International T-Cell Lymphoma Project. International peripheral T-cell and natu-ral killer/T-cell lymphoma study: pathology findings and clinical outcomes. J Clin Oncol. 2008; 26: 4124-4130. 7)Lymphoma Study Group of Japanese Pathologists. The
World Health Organization classification of malignant lym-phomas in Japan: Incidence of recently recognized entities. Pathol Int. 2000; 50: 696-702.
Fig. 2 SMILE chemotherapy for NK-cell malignancy
SMILE consists of 5 drugs which are effective for NK-cell malignancy. Methotrexate is given on the 1st day of the SMILE chemotherapy, accompanied by a 3-day course of etoposide, ifosfamide and dexamethasone (days 2─4). Because of the absence of myelosuppressive adverse reaction and a half-life of 1.3 days, L-asparaginase is given on every other days from day 8 to day 20(7 doses). The SMILE chemotherapy can be repeated with an interval of 28 days.
8)Stein H, Mason DY, Gerdes J, et al. The expression of the Hodgkin> s disease associated antigen Ki-1 in reactive and neoplastic lymphoid tissue: evidence that Reed-Sternberg cells and histiocytic malignancies are derived from activated lymphoid cells. Blood. 1985; 66: 848-858.
9)Morris SW, Kirstein MN, Valentine MB, et al. Fusion of a kinase gene, ALK, to a molecular protein gene, NPM, in non-Hodgkin>s lymphoma. Science. 1994; 263: 1281-1284. 10)Shiota M, Fujimoto J, Semba T, Satoh H, Yamamoto T, Mori
S. Hyperphosphorylation of a novel 80 kDa protein-tyrosine kinase similar to Ltk in a human Ki-1 lymphoma cell line, AMS3. Oncogene. 1994; 9: 1567-1574.
11)Savage KJ, Harris NL, Vose JM, et al. ALK-anaplastic
large-cell lymphoma is clinically and immunophenotypically different from both ALK+ ALCL and peripheral T-cell lym-phoma, not otherwise specified: report from the Internation-al PeripherInternation-al T-Cell Lymphoma Project. Blood. 2008; 111: 5496-5504.
12)Suzuki R, Kagami Y, Takeuchi K, et al. Prognostic signifi-cance of CD56 expression for positive and ALK-negative anaplastic large-cell lymphoma of T/null cell phenotype. Blood. 2000; 96: 2993-3000.
13)Falini B, Pileri S, Zinzani PL, et al. ALK+lymphoma:
clinico-pathological findings and outcome. Blood. 1999; 93: 2697-2706.
14)Benharroch D, Meguerian-Bedoyan Z, Lamant L, et al. ALK-positive lymphoma: a single disease with a broad spectrum of morphology. Blood. 1998; 91: 2076-2084.
15)Weisenburger DD, Savage KJ, Harris NL, et al. Peripheral T-cell lymphoma, not otherwise specified: a report of 340 cases from the International Peripheral T-cell Lymphoma Project. Blood. 2011; 117: 3402-3408.
16)Asano N, Suzuki R, Kagami Y, et al. Clinicopathologic and prognostic significance of cytotoxic molecule expression in nodal peripheral T-cell lymphoma, unspecified. Am J Surg Pathol. 2005; 29: 1284-1293.
17)Federico M, Rudiger T, Bellei M, et al. Clinicopathologic Characteristics of Angioimmunoblastic T-Cell Lymphoma: Analysis of the International Peripheral T-Cell Lymphoma Project. J Clin Oncol. 2013; 31: 240-246.
18)de Leval L, Rickman DS, Thielen C, et al. The gene ex-pression profile of nodal peripheral T-cell lymphoma demonstrates a molecular link between angioimmunoblastic T-cell lymphoma(AITL) and follicular helper T (TFH) cells. Blood. 2007; 109: 4952-4963.
19)The International Non-Hodgkin>s Lymphoma Prognostic Fac-tors Project. A predictive model for aggressive non-Hodgkin>s lymphoma. N Engl J Med. 1993; 329: 987-994.
20)Gallamini A, Stelitano C, Calvi R, et al. Peripheral T-cell lym-phoma unspecified(PTCL-U): a new prognostic model from a retrospective multicentric clinical study. Blood. 2004; 103: 2474-2479.
21)Dreyling M, Thieblemont C, Gallamini A, et al. ESMO Consensus conferences: guidelines on malignant lymphoma. part 2: marginal zone lymphoma, mantle cell lymphoma, peripheral T-cell lymphoma. Ann Oncol. 2013; 24: 857-877. 22)Cheson BD, Pfistner B, Juweid ME, et al. Revised response
criteria for malignant lymphoma. J Clin Oncol. 2007; 25: 579-586.
23)Savage KJ, Chhanabhai M, Gascoyne RD, Connors JM.. Characterization of peripheral T-cell lymphomas in a single North American institution by the WHO classification. Ann Oncol. 2004; 15: 1467-1475.
24)Schmitz N, Trümper L, Ziepert M, et al. Treatment and prognosis of mature T-cell and NK-cell lymphoma: an analy-sis of patients with T-cell lymphoma treated in studies of the German High-Grade Non-Hodgkin Lymphoma Study Group. Blood. 2010; 116: 3418-3425.
25)Lunning MA, Horwitz S. Treatment of Peripheral T-cell Lymphoma: Are We Data Driven or Driving the Data? Curr Treat Options Oncol. 2013; 14: 212-223.
26)Rodríguez J, Conde E, Gutiérrez A, et al. Frontline autologous stem cell transplantation in high-risk peripheral T-cell lymphoma: a prospective study from The Gel-Tamo Study Group. Eur J Haematol. 2007; 79: 32-38.
27)Reimer P, Rüdiger T, Geissinger E, et al. Autologous stem-cell transplantation as first-line therapy in peripheral T-stem-cell lymphomas: results of a prospective multicenter study. J Clin Oncol. 2009; 27: 106-113.
28)d>Amore F, Relander T, Lauritzsen GF, et al. Up-front autologous stem-cell transplantation in peripheral T-cell lym-phoma: NLG-T-01. J Clin Oncol. 2012; 30: 3093-3099. 29)Suzuki R. NK/T-cell lymphomas: pathobiology, prognosis and
treatment paradigm. Curr Oncol Rep. 2012; 14: 395-402. 30)Jaffe ES, Chan JK, Su IJ, et al. Report of the Workshop on
Nasal and Related Extranodal Angiocentric T/Natural Killer Cell Lymphomas. Definitions, differential diagnosis, and epidemiology. Am J Surg Pathol. 1996; 20: 103-111. 31)Suzuki R, Takeuchi K, Ohshima K, Nakamura S. Extranodal
NK/T-cell lymphoma: diagnosis and treatment cues. Hematol Oncol. 2008; 26: 66-72.
32)Cheung MM, Chan JK, Lau WH, et al. Primary non-Hodgkin>s lymphoma of the nose and nasopharynx: clinical features, tumor immunophenotype, and treatment outcome in 113 pa-tients. J Clin Oncol. 1998; 16: 70-77.
33)Kim GE, Koom WS, Yang WI, et al. Clinical relevance of three subtypes of primary sinonasal lymphoma characterized by immunophenotypic analysis. Head Neck. 2004; 26: 584-593.
34)Pongpruttipan T, Sukpanichnant S, Assanasen T, et al. Extranodal NK/T-cell Lymphoma, Nasal Type, Includes Cases of Natural Killer Cell and ab, gd, and ab/gd T-cell Origin: A Comprehensive Clinicopathologic and Phenotypic Study. Am J Surg Pathol. 2012; 36: 481-499.
35)Chim CS, Ma SY, Au WY, et al. Primary nasal natural killer cell lymphoma: long-term treatment outcome and relation-ship with the international prognostic index. Blood. 2004; 103: 216-221.
36)Lee J, Suh C, Park YH, et al. Extranodal natural killer T-cell lymphoma, nasal-type: a prognostic model from a retrospec-tive multicenter study. J Clin Oncol. 2006; 24: 612-618. 37)Suzuki R, Suzumiya J, Yamaguchi M, et al. Prognostic factors
for mature natural killer(NK) cell neoplasms: aggressive NK cell leukemia and extranodal NK cell lymphoma, nasal type. Ann Oncol. 2010; 21: 1032-1040.
38)Kako S, Izutsu K, Ota Y, et al. FDG-PET in T-cell and NK-cell neoplasms. Ann Oncol. 2007; 18: 1685-1690.
39)Kimura H, Ito Y, Suzuki R, Nishiyama Y. Measuring Epstein-Barr virus(EBV) load: the significance and application in each EBV-associated disease. Rev Med Virol. 2008; 18: 305-319.
40)Suzuki R, Yamaguchi M, Izutsu K, et al. Prospective measurement of Epstein-Barr virus-DNA in plasma and peripheral blood mononuclear cells of extranodal NK/T-cell lymphoma, nasal type. Blood. 2011; 118: 6018-6022. 41)Ito Y, Kimura H, Maeda Y, et al. Pretreatment EBV-DNA
copy number is predictive of response and toxicities to SMILE chemotherapy for extranodal NK/T-cell lymphoma, nasal type. Clin Cancer Res. 2012; 18: 4183-4190.
42)Yamaguchi M, Kita K, Miwa H, et al. Frequent expression of P-glycoprotein/MDR1 by nasal T-cell lymphoma cells. Can-cer. 1995; 76: 2351-2356.
43)Egashira M, Kawamata N, Sugimoto K, Kaneko T, Oshimi K. P-glycoprotein expression on normal and abnormally expand-ed natural killer cells and inhibition of P-glycoprotein func-tion by cyclosporin A and its analogue, PSC833. Blood. 1999; 93: 599-606.
44)Ando M, Sugimoto K, Kitoh T, et al. Selective apoptosis of natural killer-cell tumours by l-asparaginase. Br J Haematol. 2005; 130: 860-868.
45)Yamaguchi M, Tobinai K, Oguchi M, et al. Phase I/II study of concurrent chemoradiotherapy for localized nasal natural
killer/T-cell lymphoma: Japan Clinical Oncology Group Study JCOG0211. J Clin Oncol. 2009; 27: 5594-5600.
46)Kim SJ, Kim K, Kim BS, et al. Phase II trial of concurrent radiation and weekly cisplatin followed by VIPD chemothera-py in newly diagnosed, stage IE to IIE, nasal, extranodal NK/ T-cell lymphoma: Consortium for Improving Survival of Lymphoma Study. J Clin Oncol. 2009; 27: 6027-6032. 47)Li YX, Coucke PA, Li JY, et al. Primary non-Hodgkin>s
lym-phoma of the nasal cavity: prognostic significance of paranasal extension and the role of radiotherapy and chemotherapy. Cancer. 1998; 83: 449-456.
48)Lee J, Au WY, Park MJ, et al. Autologous hematopoietic stem cell transplantation in extranodal natural killer/T cell lympho-ma: a multinational, multicenter, matched controlled study. Biol Blood Marrow Transplant. 2008; 14: 1356-1364. 49)Yamaguchi M, Kwong YL, Kim WS, et al. Phase II study of
SMILE chemotherapy for newly diagnosed stage IV, relapsed, or refractory extranodal natural killer(NK)/T-cell lymphoma, nasal type: The NK-cell Tumor Study Group study. J Clin Oncol. 2011; 29: 4410-4416.
50)Jaccard A, Gachard N, Marin B, et al. Efficacy of L-asparaginase with methotrexate and dexamethasone (Aspa-MetDex regimen) in patients with refractory or relapsing extranodal NK/T-cell lymphoma, a phase 2 study. Blood. 2011; 117: 1834-1839.
51)Suzuki R, Kako S, Hyo R, et al. Comparison of autologous and allogeneic hematopoietic stem cell transplantation for extranodal NK/T-cell lymphoma, nasal type: Analysis of The Japan Society for Hematopoietic Cell Transplantation (JSHCT) Lymphoma Working Group [abstract]. Blood. 2011; 118. Abstract 503.
52)Delabie J, Holte H, Vose JM, et al. Enteropathy-associated T-cell lymphoma: clinical and histological findings from the international peripheral T-cell lymphoma project. Blood. 2011; 118: 148-155.
53)Weidmann E. Hepatosplenic T cell lymphoma. A review on 45 cases since the first report describing the disease as a distinct lymphoma entity in 1990. Leukemia. 2000; 14: 991-997.