mp\fiit\ac32kig8e
504-510H
(2005ff)
Seminar
2
Cardiovascular
Clinical
and
Pulmonary
Physical
Therapy
Education
in
the
United
States
Implications
for
Japanese
Physical
Therapists
over
the
Next
Decade*
LawrenceP.
CAHALIN'*
Abstract
Cardiovascu!ar
andpulmonary
diseases
are comrnon among many physical therapy(PT>
patients
asprimary,
secondary, or even combined
diagnoses,
Despite
the
fact,
that
theincidence
ofcardiovasculardisease
has
decreased
slightly,the
incidence
andprevulence
ofpulmonary
disease
and chronic cardiovasculardisease
is
increasing,
Both
disorders
are responsiblefor
a substantialdegree
of morb{dity, mDrtality, anddisability.
Physical
therapists
arein
apivotal
position
te
favorably
affect the morbidity,disability,
andpossibly
mortality ofpatients
suffering withthese
clisorders
via seeondary andprimary
prevention.
However,
few
North
American
physical
therapists
spe-eializein
this
area andfew
routinely assessthe
cardiovascular andpulmonary
systemsduring
PT.
This
is
con-cerning since cardiovascular andpulmonary
diseases
arethe
leading
causes of rnorbidity, mortality, anddisability
worlclwide,
The
results of aquestionnaire
survey of cardiovascular andpulmonary
PT
educationin
the
USA,
Canada,
United
Kingdorn,
Australia,
andNew
Zealand
reveaiedthat
cardiovascular andpulmonary
educationin
the
USA
lags
behind
thatin
other countries andin
the
USA
they
receivefar
less
attentionthan
otherdomains
ofPT
(e,g,
musculoskeletal and neuromuscular},It
appearsthat
PT
educationin
the
USA
is
not commensuratewith
the
health
care needs ofthe
USA
erthe
world,PT
for
patients
withpulmonary
disease
is
routinelypro-vided
by
Japanese
physical
therapists,
but
it
is
uncertainif
Japanese
physical
therapists
provide
optimal careto
patients
with cardiovasculardisease.
Greater
focus
onthe
health
care needs of each country andthe
worldis
neededin
the
educationalprograms
ofthe
USA
andJapan.
Providing
optimal academic and clinicalexperi-ences
in
cardiovascular andpulmonary
areas arelikely
to
ensurethat
PT
is
commensurate withthe
health
careneeds of
the
worlcl.Not
providing
optimalPT
academic and clinical experiencein
cardiovascular andpulmonary
areas will allow others
less
qualified
to
fulfill
the
needto
carefor
the
increasing
numbers ofindividuals
through-outthe
worlddiagnosed
with cardiovascular andpulmonary
disorders.
Key
word:physical
therapy
education, cardiovascular,pulmonary
lntroduction
The
theme
ofthe
40th
Congress
ofthe
Japanese
Physical
Therapy
Association
(JPTA)
was "ClinicatSensitivity".
This
is
a criticallyimportant
issue
asphysical
therapy(PT)
pro-****mo:tset4op-tszaeatho)eeiffitaetff-eftloffe:tslt6N
$Age7fita-
±okthovapttskza
7-xi-xS)Vk\pa\rkza#rv
CXN}
Correspondence/
Lawrence
P.
Cahatin
MA,
PT.
CCS,
Northeastern
University.
Department
ofPhysical
Therapy,
6
Robinson
HalL
Boston,
Massachusetts
e2J15,
USA
(e-mail,
[email protected])
gresses
into
the
new millennium.However,
defining
clinicalsensitivity
in
PT
is
diencult
because
ofdifferent
cultures,backgrounds,
interests,
responsibilities, and roles.For
the
purpose
ofthis
paper,
I
have
defined
clinical sensitivity asbeing
sensitive tothe
educational and clinical needs ofphys-ical
therapists,
otherhealth
careproviders,
andpatients
emphasizing
the
trajectory ofthe
physical
therapist
andPT
profession.
I
willfocus
onthe
educational and clinical needs efphysical
therapists,
otherheatth
careproviders,
andpatients
while emphasizingthe
career ofthe
physical
Cardiovascular
andPulmonary
Pbysical
1
willhopefully
help
you
to avoid sorne ofthe
mistakesthat
we
have
madein
theUSA
in
the
areas of cardiac andpul-monary
PT,
I
woutdlike
to
tell
you
atrue
story about cardiovascularand
pulmonary
PT
in
the
USA.
While
telling
this
storyI
would
like
to
discuss
(1)
the
role of thephysical
therapist
in
cardiovascular andpulmonary
disease
-
worldwide and theUSA
dilemma,
(2)
pulmonary
PT
educationin
theUSA,
Canada,
UK,
Australia,
andNew
Zealand
andhow
pulmonary
education and clinical
practice
in
these countries relate toJapan,
and(3)
theimportance
and needfor
international
col-laboration
and "ClinicalSensitivity".
I
would
like
te
addresseach of these
primary
objectives andbegin
withthe
role of thephysical
therapTstin
cardiovascular andpulmonary
dis-ease.
The
Rele
efthe
Physical
Therapist
in
Cardiovascular
and
Pulmonary
Disease
The
role ofthe
physical
therapistin
cardiovascular andpulmonary
disease
was very clearlypresented
in
an articleby
aninternational
collaborativegroup
ofphysical
therapists
representing
12
different
countriesfrom
aroundthe
globei).
The
purpose
ofthis
articlewas tohighlight
the
high
preva-lence
andincidence
of cardiovascular andpulmonary
disease
in
industrialized
and non-industrialized countries andthe
major role and
impact
thatphysical
therapiszs shouldhave
in
rhe examination and management ofpersons
withcar-diovascular
andpulmonary
diseasesi).
This
paper
hightighted
thefact
that
heart
disease,
hyper-tension, stroke, smoking-relatedlung
conditions such as can-cer and chronic obstructivepulmonary
disease
(COPD),
anddiabetes
arethe
leading
causes of mortality, morbidity, anddisability,
However,
the
international
team ofphysical
ther-apists who wrotethis
paper
indicated
that
these
diseases
are notleading
practice
areasfor
PT
in
their
respectivecountriesi),
In
fact,
they
saidthat
''This
essential area ofphysical
ther-apypractice
<cardiovascular
andpuimonary
PT)
riskssink-ing
into
oblivion as otherstess
qualified
attemptto
fi11
thisvoid" and emphasized
the
fact
that
"physical
therapists
arenoninyas{ve
practitioners
whohave
the
ethicalresponsTbili-ty
to
educatehealth
care colleagues as welL asthe
public
about
the
power
of andpreference
for
noninvasive inter-ventiens wheneverpossible."i}
These
are extremely imper-tuntissues
as we continueto
develop
clinical sensitivityin
the
USA,
Japan,
andthe
world.
Other
issues
addressedin
thisinternationally
diverse
paper
included
(1)
historical
factors
thathave
contributedte
the
relativeinvisibility
of cardiovascuLar andpulmonary
PT,
(2)
rationalefor
carcliovascular andpulmonury
PT
tobe
morevisible, and
(3)
strategiesto
make cardiovascular andpul-Therapy
Education
in
the
United
States
505
monary
PT
more visiblei).Each
ofthese
issues
willbe
briefiy
discussed
belew.
Historical
Factors
Contributiug
to theRelative
Invisibility
of
Cardiovascular
andPulmonar),
Physical
71}Leram,
in
the
Wbrld
The
historical
fuctors
thathave
contributedto
the
tive
invisibility
of cardiovascular and pulmonaryPT
aresurned under
the
fragmented
ratherthan
systematietion
of cardiovascular andpulmonary
PT
andinclude
the
(l)
developrnent
of chestphysical
therapy andthe
primary
focus
on secretion removal techniquesbetween
the
early1900's
to
the
l950's.
(2)
development
of cardiac rehabiiitationin
the
1960's,
{3)
frequent
separation of cardiacfrom
putmonary
PT
and not a combined cardiopulmonary
PT
approachfrom
the
1960's
to
the
present
(4)
greater
academicfocus
onloskeletal
and neurologicalphysical
therapy
due
mostlikely
to
the
poliomyelitis
epidemics andinjuries
of warout
the
1900's,
and(5)
lack
of allegianceto
physician
groupsand relative
independence
from
physicians
throughout thehistory
ofNorth
American
PTi'2).
All
of thesefactors
have
separated cardiovascular andpulmonary
PT
andhave
ed
in
a separation ef cardiovascular andpulmonary
ogy,physiology,
andthe
clinical examinalion andrnent of
patients
withthese
disorders.
These
factors
have
also separated cardiovascular and
pulmonary
PT
from
other
domains
ofPT
andhave
made cardiovascular andpulmonary
PT
less
visible.
The
result of such separationis
afragmented
physical
therapist
andPT
profession
that
have
evolvedin
aseparateand
fragmented
manner.Combining
cardiovascular andmonary
PT
practice
with agreater
emphasis withinPT
catien and clinical
practice
willlikely
stimulate a
ic
evolurion of cardievascular and pulmonaryPT
withinthe
PT
profession.
Combined
examination and management skMs
in
both
cardiovascular andpulmonary
PT
willprovide
the
heaith
care systerns of the world animportant
health
careprovider
{the
physicaltherapist)
whois
able to addressthe
disablement
associated withthe
majordiseases
ofthe
worldand
possibly
prevent
orpostpone
thedevelopment
efability
due
to cardiovascular andpuimonary
diseases.
The
interrelatedness
of the cardiovaseular andpulmenary
tems
demand
a comprehensive understanding ofbeth
tems
by
everyphysieal
therapist
whichis
Iikely
to
improve
the management of cardiovascular,pulmonary,
or combinedcardiopulrnonary
disorders,
Furthermore,
developing
professional
relationships with
physician
and otherhealth
careprofessional
groups
in
asubservient manner
is
Iikely
to
promote
anintegrated
lution
ofcardiovascular andpu]monary
PT
with needed506
ge"utza\
apists
in
theUSA
have
limited
their
relationships withcians
because
of aproblematic
histery
ofphysician
ownedPT
practices,
respiratorytherapists
in
the
USA
have
oped such a
physician
support systemthat
has
enabledthe
respiratory
therapy
professionto
be
quite
successfulin
the
USAZ),
Physical
therapists
werking withinthe
lar
and pulmonarydomains
whohave
developed
suchsubservient
professional
relationships withphysicians
andother
health
careprofessionals
have
censistentlybeen
cessful and
have
stimulated a cohesive evotving aiPT
practice culminatingin
greater
responsibility andtice
opportunities withinthe
health
care arena3'5).It
is
sible that
the
doctor
ofPT
(DPT)
whichhas
been
readilyaccepted as
the
terminal
degree
in
PT
in
the
USA
wMther
facilitate
non-subservientPT-physician
relationships.Attempts
to
correct the abovehistorical
problems
arely
to
make cardiovascutar andpulmonary
PT
more visible.Correcting
the abeveproblems
willrequire substantialicat
sensitivity".Rationale
for
Cardiovascular
andPulmonaT:y
Physical
71hercury
tobe
bfore
Visible
The
rationalefor
cardiovascular andpulmonary
PT
to
be
more visible
is
quite
strong andincludes
(1)
the
escalatingcost of medical care,
{2)
thefact
that
physical
therapists
arelicensed
health
careproviclers,
(3)
the
noninvasive nature ofPT,
and(4)
an expandingliterature
supporting exerciseapy and
physical
therapy as atreatment
for
cardiovascularand
pulmonary
disorders
that
has
the
potential
to
reversecardiovascular
disease,
enhance oxygentransport
andimprove
cardiovascular andpulmonary
function,
prevent
diovascular
and pulmonarydisorders,
andimprove
the
ability of cardiovascular and
pulmonary
diseasei).
Strategies
to
Mahe
Cardiovascular
andPulmonary
Physical
Thercope,
Mbre
Visible
The
strategies to make eardiovascular andpulmonary
PT
Table
1
Strategies
to
Make
Cardiovascular
E32tsrg8e
and
more visible are relatively simple,
but
veryimportant,
andconsist of several specific skills
listed
in
Table1i).
Of
these,
the
skillin
articuiating the scope of cardiovascular andput-monary
PT
practiceto
otherhealth
careproviders,
health
insurance
companies, andlegislators
via clinicalpractice
andresearch
is
mostimportant.
Cardiovascular
andpulmonary
PT
witlbe
mest visible through communication withphysi-cians, nurses, other
health
careproviders,
insurance
compa-nies, andpolicy
makers.The
forms
of communication are numerous andperhaps
the
most effective mode ofcommu-nication
is
through
publication
ofPT
research.One
final
issue
that
was addressedin
the
abovepaper
by
the
internationally
diverse
group ofphysical
therapists
wasclinical education.
The
authors of this articlestated "ThePT
profession
must ensurethat
cardiovascular andpulmonary
PT
develops
commensurate with globalhealth
care needs andthat
thisis
refiectedin
PT
academic curricuta across areas ofpractice
and research"i).However,
the
authors con-cludedthat
"In
part,
the
profession
has
failed
toprovide
ade-quate
continuing education"i).Greater
attentien
to
cardio-vascular andpulmonary
disorders
in
PT
education will makePT
education commensurate withglobal
health
care needsand
increase
the
visibility of cardiovascular andpulmonary
PT.
To
summarizethe
Trnportant
issues
presented
in
this
paper
published
at thebeginning
ofthe
new millennium, cardiovaseular andpulmonary
PT
shouldbe
more visiblebased
on(1)
the
overwhelming evidence-base ofthe
effects exercise andphysical
therapy
ondisablement,
(2>
the
agingpopulation
andincreasing
incidence
andprevalence
ofcar-diovascutar
andpulmonary
disease,
(3}
the
escalating costsof medical care with the potential
fer
physical
therapists
to
provide
less
expensiveinterventions
with afocus
onprimary
prevention,
{4)
usingthe
above strategiesto
promote
car-diovascular
andpulmonary
PT
visibility, and{5)
attemptingto
correctthe
abovehistorical
problems
that
have
separat-ed cardiovascular and
pulmonary
PT
from
otherdomains
ofPulmonary
Physical
Therapy
More
Visible
1,
Skill
in
articulatingthe
scepe ofpractice
as well asthe
benefits
andlimitations
oftheir
care suchthat
others understand that cardiovascular and
pulmonary
PT
is:
a.
holistic,
evidence-based, andhas
long-term
benefits
b.
Iow
risk,has
few
side efiects, andis
cost-effectivec. not subservient
to
invasive
medical care orbiotechnology,
but
complimentsthem
2.
Skill
in
initiating
and endorsinghealth
and wellness campaigns3.
Participate
in
public
health
forums,
health
carepolicy
making,health
fairs,
public
health
events, and
health-related
organizations4,
Participate
in
clisease
managementprograms
5.
Be
visiblein
the media&
practice
in
an eviclence-based manner6.
Exploit
existingtechnologies
&
develop
new ones7,
Devetop
non-subservientprofessionat
relationships withphysicians
and otherhealth
careprofessionals
8.
Develop
agreater
focus
in
cardiovascular andpulmonary
PT
in
PT
education9.
Develop
more clinical aenliationsin
cardiovascular andpulmonary
PT
with welltrained
mentors
Cardiovascular
andPulmonary
Physical
PTi).
Therefore,
cardiovascular andpulmonary
PT
shou]dbe
more visible via "clinical sensitivity''.The
Uhited
States
Dilemma
The
dilemma
in
cardiox,ascular andpulmonary
PT
in
the
Unired
States
is
a simpleprobtem,
but
withdramaric
con-sequences
for
PT
due
to thepowerful
effects of supply anddemand,
In
the yearsbetween
1950
and1980
fewer
USA
physica] therapists wereinterested
in
intensTve
care unit(ICU}
care and cardiovascular orpulmnnary
PT
{because
ofa
greater
interest
in
musculosketetat, and neurologicalI]T)
despite
the
continuingpoliomyetitis
epidemics andthe
res-piratory
complications associated withpoliomyelitis6).
As
a result,fewer
physical
therapists were available tomanage
patients
in
theICU
or thosepatlents
withcardie-vascular and pulmonary
problems.
This
resuttedin
the
devei-opment of the respiratory
therapist
andthe
Respiratory
Therapy
AssociationL),
There
was a need tocarefor
patients
in
theICU
andpatients
with cardiovascular andpulmonary
disorders
and respiratorytherapists
fulfitled
the
need.This
is
aperfect
example of suppty andclemand
betzveen
the
PT
and respiratory therapy professions,
Unfortunately,
noleg-islative
effbrts or practice actions were undertakenby
theAmerican
Physical
Therapy
Association
(APTA)
or theIJSA
PT
educationat programste
keep
USil
physical
therapists
in
theICU,
Because
of the abovediscordance
in
cardievascular andpulmonary
PT
practice,
aBritish
trainedphysical
therapist
(May
Watrous}
workingin
theUSA
became
x,ery concernedabout the
USA
dilemma7),
May
Watrous
was very concernedbecause
physical
therapists
had
been
criticizedfor
ignoring
patients with acute or chronic chestdiseases
at atime
whenincreasing
numbers ofpatients
having
chestdiseases
werechattenging
the
health
professions.
Because
ofthis,
she sentasimple
questionnaire
surveyto
the
63
USA
PT
schoo]sto
determine
the
pulmonary
educatienprovided
to
physical
therapists
in
19747).
She
found
that
a majority ofPT
schoolsdid
not offer a coursein
pulmonary
PT
and a number ofPT
schoolsfailed
to
teach
disease
specifictreatments
and allowedtoo
littie
preparation
time
in
puimnnary
PT7).
As
a resutt of rhe above study)vlrs.
"iatrous
stated"to
send even one
physical
therapist
outpoorly
prepared
zo
treat
patients
with chestdiseases
is
regrettabte/to
have
schoots minimizethis
areain
the
face
oftoday's
needis
deplorable"7).
She
also wrote that''physical
therapists'back-grounds
allowthem
toCl)
make a unlque contributionto
the
welt-being of
patients
with chestdiseases,
(2}
teach
patientshow
to
prevent
chestdamage
andphysicat
deterioration,
and(3)
bring
about maximum recovery within thelimits
ofthe
cendition"7).
These
words were true then and even moretrue
today
withthe
increasing
incidence
andprevalence
ofTherapy
Education
in
the
United
States
507
lung
diseases
throughout
the
wortd.
Mrs,
Watrous
continued to addressher
concernfur
monary
}'T
by
stating"schools
ofPT
shouldpresent
diovascular
andpulmonary
PT
as one ofthe
most
tant,
interesting,
and stimulating thut ourprofession
offers"and "if we uontinue to
ignore
chestPT
in
ourhospitals
andschools, or
fail
to acquire excellencein
our treatrnent skills.a
fascinating
and rewarding area maybe
tost
te
the
PT
fession"7).
She
concluded with''Worst
of alt,the
chestpaticnt
who needs
PT
will missthe
vitalhelp
we cangive"7).
Her
words again are criticat
to
teday'sphysical
therapist,to
the
PT
profession,
and to t{)day'spatients.
Furthermere,
in
the
LJSA,
the above statement regarding the pessibility ofing
pulmonary
eare as aPT
practice
areahas
ly
become
partly
true
andit
maybecome
completeLy trueif
specific actions are nottaken
by
USiX
physical
rherapists.
IJSA
PT
educationatprograms,
andthe
iXPTA.Therefore,
the
specific actions rhatUSA
physical
therapists,
USiX
PT
educationprograms,
andthe
APTA
mustperform
are
Ly
relatedto
''clinical
sensitivity".Pulmonary
PT
Education
in
the
USA,
Canada,
UK,
Australia,
and
New
Zealand
-Clinical
Implications
for
Japane$e
Physical
Therapists
Because
ofthe
current status uf cardioi,ascular and monaryPT
in
the
USA
discussed
above andthe
results of
the
1977
studyby
}v'Tay
Watreus,
",e studiedPT
education
in
the
USA
and several otherEnglish
speaking countries to
determine
the
current status ofpulmonary
PT
educutioncornpared to that
in
1977Si.
t'Xlthough)vtay
Watrous
did
notstudy
{nternational
pulmonary
PT
education webelieved
it
of
greai
valueto
compareputmonary
PT
educationbetween
the
LjSA
and otherEngtish
speaking countries.Of
lar
importance
fer
this
puper
I
willdiscuss
lhe
implications
this
data
has
fer
Jupanese
PT
andinternational
"Clinical
Sensitivity".
Survey
quastionnaires
were sent to all200
USA
P'1'
cational
programs
and to thePT
educationalpr"grams
in
Canada,
the
United
Kingdom
(UK),
Australia,
andNew
ZealandS).
The
response ratesfrom
Canada
andthe
[/K
wera15%
andl8%,
respectively.The
response rateirom
both
Australia
andNew
Zealand
was50%
andthe
response rate
frorn
the
USA
",as31%.
Analysis
ef thequestionnaire
resuttsrevealed
that
pulmonary
educationin
the
USt'X
was similaramong allof
the
5
regions ofthe
IISA
(Nc)rtheastern.
Atlantic.
Southeustern,
CentraL
andWestern
regions} andsignificantly
fewer
hours
of cardiopulmonaryPT
educationwere
provided
toUSA
students comparedto
tal
ancl neuromuscularPT
eduEation(4.9
cardiopulmonary
508
Table
2
Instruction
rp"ptil\
rg32tsag8e
Time
in
Pulmonary
Physicat
Therapy
in1974
and2003
Categories
Number
ofSchoolsReporting
Instruction
Time
in
1974
Y2
Hr.
IHr,
2Hr,3
Hr.
4
Hr.
No
orMore
Answer2oo3
Hrs"
L
2.
3,
4.
5.
6,
7.
8.
9.Ie,IL12.13.14.15.16.17.
A&P
Resp,
System
PFTsPsychosocial
Probs.
InterrelationsA
DrugslMech.
Vent.
Path,fProg.
Asthma
Asthma
Rx
Path/Prog.
Emphysema
Emphysema
Rx
Path,fProg.
Bronchitis
Bronchitis
Rx
PathJProg.
Bronchiectasis
Bronchiectasis
Rx
Path,
ofAcute
Condit.
Pre-IPost-Surgical
Condit,
Pre-IPost-Surgical
Rx
Special
Probs.AA
o4212117181213919122616o2218
4101019251516151414II881820195
6105oo459105532912911
54ooo5234111o2222
32l7ooo111613137672
911201614132015131624l72720131618
8,O'"2.41.42.55,O"LlLl1.31.41.11.3O.8O.8
**e,7
**3.e
**3.0O.8
Adapted
from
Watrous
ML.
Chest
Physical
Therapy
-
A
Survey
and aChallenge.
Phys
Ther
1977:
57(2):
143-14Z
Hr.
=,
hour:
A&P
Resp.
= anatomy and physiology ofthe
respiratory system:PFTs
=
pulmonary
function
tests:
Probs.
=problems:
Mech.
Vent
= mechanical ventilation:Path,fProg.
=pathologyfprognosis;
Rx
=treatment:
Condit.
=con-ditions.*..2003
Hrs
= mean number ofhours
ofinstruction
reportedby
the
USA
Physical
Therapy
Programs
in
2oo3,
Mean
number of2003
hours
for
these
questions
is
the
sum ofhours
from
two
or mere separate areas or conditions{i.e.
number ofhours
of respiratory anatomyinstruction
+
number ofhours
of respiratoryphysiology
instruction).
A
Interrelations
with otherhealth
careprofessionals
such asphysicians,
nurses, respiratorytherapists,
and aicles. AASpecial
problems
such as collapsedIobes.
it
hours
for
musculoskeletal and neuromuscularPT:
p<
O.05}8).
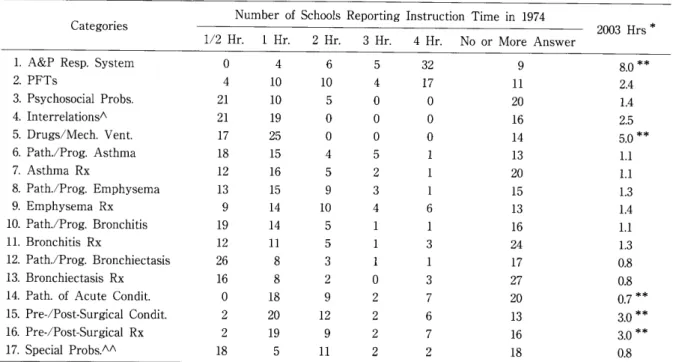
Table2
has
been
slightly adaptedfrom
atable
published
by
May
Watrous
in
1977
and showsthe
instruction
time
in
pulmonary
PT.
The
originaltable
that
Ms,
Watrous
pub-lished
is
in
the
middle andleft
side ofTable
2
andlists
the
number of
PT
schools reportinginstruction
time
in
17
areasin
1974
(with
the
number of schools efferinglf2
hour,
1
hour,
2
hours,
3
hours,
4
hours
orMore,
orNo
Answer),
The
last
column onthe
far
right ofTable
2
was addedto
the
originatWatrous
table
and showsthe
mean number ofhours
ofinstruction
time
in
each of the17
categoriesin
2oo3,
This
column showsthat
comparedto
1974,
the
num-ber
ofhours
spent educatingUS
students aboutPutmonary
PT
has
increased,
but
notin
ull of the17
areaslisted,
The
greatest
amount ofinstruction
timeis
in
Anatomy
andPhysiology
and theleast
amount ofinstruction
time
is
in
the
Pathotogy
ofAcute
Conditions.
This
is
concerning as aremany of the other categories showing
less
than
2
heurs
ofinstruction
time
(a
total
of11
out of17
categories or65%
of
the
Pulmonary
PT
categorieshad
less
than
2
hours
ofinstruction)S}.
Comparing
pulmonary
PT
educationin
the
USA
to
the
World
revealedthat
95%
less
time
is
spentin
cardiovascu-lar
andpulmonary
PT
education and only slightly morehours
areprovided
in otherdomains
ofPT
Education
(e,g.
musculoskeletal and neuromuscular)
in
the
USA
comparedto
otherEnglish
speaking countries,We
atsofound
that
<1}
fewer
USA
credithours
are providedin
anatomy andphys-iology
ofthe
respiratory system, mechanical ventilation and suctioning, and education and treatment of severalpul-monary
patholegies
and(2)
fewer
USA
students chosepul-monary affiliations.
Another
important
aspect about ourstudy and
the
poor
USA
response rateis
that
manyUSA
PT
education programslikely
have
part-time
faculty
teach-ing
cardiopulmonaryPT
which waslikely
to
<1)
yield
the
poor
USA
respense rate and(2)
give
students aless
than
favorable
impression
ofthis
domain
ofPT.
These
areissues
that
my colleagues andI
are very concerned aboutfor
car-diopulmenary
PT
andthe
PT
profession
in
theUSA,
However,
some ofthese
problems
do
not appear tobe
is}
lated
to
the
USA
aloneS
iO},In
2003
Roskell
andCross
published
their
findings
ofBritish
PT
student'sperceptions
of cardiopulmonaryPT9).
The
purpose
ofthe
study was to examine studentpercep-tions of cardiopulmonary
PT
in
orderto
possibly
recruit newgraduates
to
practice
in
cardiopulmonaryPT.
Fifteen
final
year
studentsfrom
22
undergraduatePT
schoolsin
the
UK
(total
N=330)
were selectedto
answer10
questions
about cardiopulrnonaryPT.
The
results ofthis
studyfound
that
Cardiovascular
andPulmonary
Physical
222
ofthe
330
questionnaires were returned(67%
response rate) revealingthat
80%
ofthe
studentsbetieved
cardiopul-monaryPT
was of significant value,but
that
only6%
stat-ed anintent
to
specialize9).Also,
30%
ofthe
students stat-ed that they wereless
competentin
cardiopulmonaryPT
than
other specialties9).These
results are clinically signifi-cant sincefew
studentsin
the
UK
intend
lo specializein
cardiopulmonaryPT.
The
sameis
likely
true
in
the
USA
andis
likely
due
to
agap
between
education andpractice,
Roskell
andCross
as well asHunt
et alstatethat
studentslack
knowledge
ofthe
`worldof work'
in
the
cardiopul-monary area which makesit
necessaryfor
universitiesto
provide
opportunitiesto
better
integrate
cardiopulmonaryeducation with cardiopulmonary
PT
practice
in
the
work-place9)iOi.
It
appearsthat
what occurredin
the
USA
cluring
the
1950's
to
l980's
is
now occurringin
the
UK
withBritish
physical
therapistspracticing
in
otherdomains
ofPT.
This
is
extremelyimportant
as we trainfuture
physical
thera-pists
aroundthe
globe.
Because
cardiovaseular andpul-monary
PT
is
practiced
by
sofew
North
American
physi-cal
therapists,
PT
studentsin
theUSA
are exposed tofewer
cardiovascular and
pulmonary
clinical affiliations andmen-tors.
Therefore,
the
USA
andPT
educationalprograms
around
the
globe
mustbecome
more "clinicatly sensitive''to
the
international
differences
in
academicpreparation
ofphys-ical
therapists
andto
cardiopulmonaryPT
education.International
clinical athliatiens arnongdifferent
countries are necessary and willlikely
facilitate
the
development
ofcar-diovascular
andpulmonary
PT
in
the
USA.
The
APTA
CIinical
Specialization
andClinical
Residency
Programsii)
arelikely
topromote
cardiovascular andpulmonary
PT,
but
greater
emphasisis
neededin
basic
cardiovascular andpul-monary
PT
educationto
develop
greater
cardiopulmonaryinterest
and numbers of cardiovascular andpulmonary
elin-icians
who can serve as mentersin
clinical affiliations.There
is
a needfor
greater
"clinicalsensitivity''within
the
PT
pro-fession
aroundthe
globe.
Clinical
Jmplications
for
Jdpanese
Physical
Therapists
The
previous
discussion
andquestionnalre
survey resu]tshave
important
clinicalimplications
for
Japunese
physical
therapists.
The
majorimplications
for
Japanese
physical
ther-apists
include
the needto
continue to(1)
maintain apres-ence
in
the
ICU,
(2)
make cardiovascular, pulmonary, andother
domains
ofPT
visiblein
Japan,
(3}
exploit exist{ngtechnologies
anddevelop
new onesin
cardiovascular,pul-monary, and other
domains
ofPT.
and(4)
develop
non-sub-servient
professional
PT
-
physician
relationships.
Although
cardievascular andpulmonary
PT
may notbe
particularly
high
profiLe
practice
areasin
Japan,
the
pres-ence of
Japanese
physical
therapists
in
the
ICU
is
tikely
to
Therapy
Education
in
the
United
States
509
maintain
this
particular
practice
area as aPT
practice
domain.
In
the
USA,
the
small number ofUSA
physical
apists
in
the
ICU
resultedin
the
deveiopment
of the
Respiratory
Therapy
profession
and the currentlimited
tice of
USA
physical
therupists
in
theICU,
Maintaining
apresence
in
the
ICU
is
therefore
]ikely
to
maintainthis
domain
ofpractice
in
Japan.
Japanese
technology
has
influencecl
every aspect oflife
around the globe and combining
PT
with existingnolegies will
likely
facilitate
PT
growth
in
Japan
and theworld.
Coordinated
effortsbetween
Japanese
physical
apists and
Japanese
technologists
to exploit existingnologies and
develop
new ones willlikely
enableJapanese
physical
therapists
to
be
worldleaders
in
rehabilitatien.A
PT
-
technology relationship maybe
best
promoted
by
the
Japanese
PT
Association
(JPTA}.
The
JPTA
may alsofacilitate
the
visibility ofPT
in
japan
by
standardizingPT
educ:ation and consideringthe
tions
of advanceddegrees
]ike
the
DPT.
The
DPT
may not
be
the
preferred
terminal
degree
in
Japan,
but
advancingthe
PT
profession
through
advanced academic standards and
degrees
appears tohave
occurredin
the
USA
and othercountries6).
Other
implications
for
Japanese
physical
therapistsinctude
the
needto
(1)
provide
optimaL clinical affiliationsfor
Japanese
PT
student's,(2}
narrowthe
gap
between
PT
ory and
practice,
and{3)
educatethe
world aboutPT
tice
in
Japan.
Providing
PT
students with optimal clinicalaffiliations and narrowing
the
gap
between
PT
theery
and
practice
areglobal
PT
problems
thut
mustbe
re$olved,The
wiclespread
PT
presence
in
the
ICU
in
Japan
has
the
tial
for
optimal clinical affiliations which arelikely
to
row the
gap
between
PT
theory andpractice
in
the
diovascular
andpulmonary
domains.
Establishing
tional
clinical affiliationsbetween
Japanese
clinical sites andother countries of
the
worLdis
Hkely
to
promote
the
opment of cardiovascular and
pulmonary
PT
aroundthe
globe,
Informing
the
wor!d aboutPT
practice
in
Japan
is
avery
irnportant
facter
that
willfurther
facilitate
Japanese
research, clinical
practice,
and eclucation.Informing
the
worldabout
Japanese
PT
canbe
accomp]ishedin
many ways ofwhich clinlcal research and
innovative
PT
-
technotogieal
relationships arethe
mostlikely
to
be
successful,Clinical
sensTtTvity
to
PT
is
important
in
Japan
andthe
world.Conclusion
The
theme of clinical sensitivityis
important
for
PT
around
the
globe,
Being
sensitive to the educational andical
needs ofphysical
therapists, otherheaLth
careproviclers.
and patients while emphasizingthe
trajectery
efthe
ical
therapist anclPT
profession
are criticallyimportant
51e
ge"fiza\
issues
in
Japan,
USA,
and all countries wherePT
is
ticed.
Cardiovascular
andpulmenary
diseases
arethe
majorcauses of
disablement
throughout the world andphysical
therapists
are capable of making a significantirnpact
onthese
disorders.
However,
cardiovascuLar andpulmonary
PT
has
poor
visibility worldwide whenit
shoutdbe
the mostvisible
domain
ofPT
practice.
A
variety of strategies exist
to
make cardiovascular andpulmonary
PT
more visible ofwhich skill
in
communicatingthe
favorable
effects ofPT
oncardiovascular and
pulmonary
diseases,
increasing
the
focus
of cardiovascular and
pulmonary
education, anddeveloping
PT
-
technologlcat
professional
relationships are most
tant.
Increasing
elinicalsensitivityin
PT
is
necessary tomote
the
PT
profession,
cardiovascular andpulmonary
PT,
and optimal patient care around
the
globe.
Not
increasing
ctinical sensitivity
in
PT
is
likety
to
allow othersless
ified
to
fulfill
roles that wouldbe
best
perfermed
by
ical
therapists,
thus
providing
suboptlmal careto
patients,
eg32tsag8e
o
2)
3)4)
5}
6)
7)8}9)]o)
11)References
Dean
E,
Frownfelter
D,
WongWP,
et al./Cardiovascular/cHr-diopulmonary
physicul therapy sinks or swimsin
the2]"t
cen-tury/
Addressing
thehealth
careissues
of ourtime.
Phys
Ther
80(12),1275-127g,
2000,
Weiiacher
RR.
AARC
-50
Years
ofService.
http/f,'www,aarc.org!member.services/history,htmL
Lee
AP.
Ice
R
BIessey
R,
et al./Long-term
effects nfphysicat
training
on eoronary patients withimpaired
ventricularfunction.
Circulation
60,
1519-1526,
1979.Cardioputmenary
Physicat
Therapy
(2"d
Edition).Irwin
S,
Tecklin
JS
(eds),
CM
Mosby
Company.
St.
Louis,
199e.Cahalin
LP,
Blessey
RL,
Kummer
D,
Simard
M, Thc safety ofexercise testingperfermed
independently
byphysical
therapists.
J
Cardiopul
Rehabil
7{6),
269-276,
1987.Moffat
M,
IIistory
of physicaL therapy practicein
theUnited
Stutes.
J
PhysicalTherupy
Education
2003,
Winter.
Watrous
ML/Chest
physical therapy-A
survey and achat-lenge,
Phys
Ther
57(2)/
143-147.
1977.
Cahalin
LP,Wiltoughby
S,
Brooks
G:
Pulmonary
Physical
Therapy
Education