■ 原 著
膵島分離用酵素の変更とドナー背景の変化が臨床膵島分離成績に
与える影響の検討
山根 佳
1,穴澤貴行
1,多田誠一郎
1,井ノ口健太
1,江本憲央
1,藤本七恵
1,秦浩一郎
1,
増井俊彦
1,田浦康二朗
1,上本伸二
2The effects of enzymes for islet isolation and donor background on the results of clinical
islet isolation
1 Department of Surgery, Graduate School of Medicine, Kyoto University, 2 Shiga University of Medical Science
Kei YAMANE 1, Takayuki ANAZAWA 1, Seiichiro TADA 1, Kenta INOGUCHI 1, Norio EMOTO 1, Nanae FUJIMOTO 1,
Koichiro HATA 1, Toshihiko MASUI 1, Kojiro TAURA 1, Shinji UEMOTO 2 【Summary】
【Objective】The donor factors and enzymes for islet isolation can exert a significant influence on the islet isola-tion results. Until 2007, Liberase HI was used as the enzyme for clinical islet isolaisola-tion; however, since the islet transplant clinical trial started in 2012, Liberase MTF has been used. Moreover, since 2013, islet transplantation from donors after brain death (DBD) has been started. Here, we examined the effects of donor factors and en-zymes on results of clinical islet isolation.
【Design】Retrospective case series.
【Methods】We compared the donor factors and islet isolation results of the two groups at our institution; the ear-ly group had 25 cases from January 2004 to Juear-ly 2007, and the late group had 13 cases from Juear-ly 2013 to No-vember 2018.
【Results】In the early group, the donations were only obtained from donors following cardiac death. However, in the late group, the donations were mainly from DBD. Owing to changes in donor background, the cold ischemic time was significantly longer in the late group (284.6±86.1 min vs. 386.9±89.1 min, p<0.005). Upon compari-son of the islet isolation results, no significant difference was observed in the digestion time (21.2±6.9 min vs. 18.7±6.4 min, p=0.25) or IEQ/g pancreas after purification (4.76±2.51 vs. 3.83±1.08<×10 3>), p=0.22);
20 of the 25 patients in HI group and 11 of the 13 patients in the MTF group met the transplantation criteria ( p= 0.72).
【Conclusion】We found that the clinical islet isolation results were maintained well after the change in enzymes and change in donor background.
Keywords: islet transplantation, islet isolation, type 1 diabetes, collagenase
I.はじめに
重症低血糖発作を伴うインスリン依存性糖尿病患者 に対する移植治療として,膵島移植が注目されてい る。膵島移植は低侵襲で安全性が高い移植治療であり ながら,血糖値の安定化と重症低血糖発作からの解放 をもたらし QOL を改善しうる 1, 2)。一方,インスリン 離脱を得るためには複数回の移植を要し,長期生着率 1京都大学医学部医学研究科外科学講座肝胆膵・移植外科,2滋賀 医科大学学長 (2020・8・8 受領;2020・12・21 受理)にはいまだ改善の余地があると考えられている 3)。 膵島移植において良好な成績を得るためには,ド ナーから提供された膵臓から Viability の高い膵島を数 多く分離することが前提となる。膵島分離の工程の中 で,膵島分離用酵素(コラゲナーゼ)は,膵島の収量 や質に大きな影響を及ぼす因子である 4)。本邦におい ては,2007 年までは Liberase HI(ロシュ社)を膵島 分離用酵素として使用していた 5)。しかし Liberase HI の製造工程で使用される微生物の培養液中にウシ脳神 経抽出物が添加されていることが判明し,プリオン病 感染のリスクが完全に否定できないことから,その販 売が中止され,同時にわが国の臨床膵島移植も一時的 に停止した 6)。その後,2012 年から哺乳類由来の材料 を用いずに製造された Liberase MTF が使用できるよ うになり,北米の CIT(Clinical Islet Transplantation) プロトコールをもとにした新たな免疫抑制プロトコー ルを導入した臨床膵島移植が多施設共同臨床試験とし て再開された 7)。また,2013 年からは脳死ドナーから の膵島提供が本邦でも可能となり近年は膵島提供のド ナー背景も大きく変化している 7)。 当院では,2004 年の本邦第 1 例目の臨床膵島移植 以降,2018 年までに 38 回の臨床膵島分離を行ってき た。2020 年 4 月には,「同種死体膵島移植」として膵 島移植が保険導入されており,今後症例数の増加が期 待される。一方,本邦において臨床膵島分離用酵素の 変更やドナー背景の変化が膵島分離・移植成績に与え た影響は明らかでない。今回われわれは,当院で施行 された臨床膵島分離におけるこれらの因子の影響を明 らかにし,今後の臨床膵島移植の展開に寄与する知見 を得ることを目的とした検討を行った。
II.対象と方法
対象は,2004 年 1 月から 2018 年 11 月までに当院 で実施した 38 例の臨床膵島分離とし,膵島分離用酵 素として Liberase HI を使用した 2004 年 1 月から 2007 年 7 月までの前期群 25 例,Liberase MTF を使用した 2013年 7 月から 2018 年 11 月までの後期群 13 例の 2 群に分け,ドナー因子や膵島分離成績を後方視的に比 較検討した。 膵臓は心停止あるいは脳死ドナーから提供を受け, 前期は全例で二層法(ETK 溶液と PFC 溶液) 8),後期 は近隣での提供であった 2 例のみ UW 液単純浸漬保 存で,その他は二層法であった。膵島分離は京都大学 医学部附属病院の分子細胞治療センター(Center forCell and Molecular Therapy:CCMT)で行った。膵島 分離は Edmonton group の方法を改良した方法にて 行った 9, 10)。Digestion time は,膨化後の膵臓を Ricordi s
chamberに 入 れ 回 路 内 が 溶 液 に 満 た さ れ chamber の shaking を始めた時間から消化組織回収開始まで,
Dilution timeは回収開始から回収終了までの時間と定
義した。膵島純化は比重遠心分離装置(COBE 2991 cell processor, Gambro Laboratories, Denver, CO)を用い て行った。密度勾配溶液の作成には前期群の 4 例で Ficoll(GE Healthcare, Little Chalfont, UK)が用いられ たが,以降は全例で Iodixanol(Optiprep, Sigma-Aldrich St. Louis, MO)を使用した。 移植成績は最終膵島移植後 3 か月のものを用いた。 SUIT-Index は以下の式で計算した 11)。 SUIT-Index=空腹時血中 C-peptide(ng/dL)/(空腹 時血糖値−63(mg/dL))×1,500 統 計 学 的 解 析 は Student s t-test,Mann-Whitney U test,χ 2検定にて行い,p<0.05 を有意差ありとした。
III.結 果
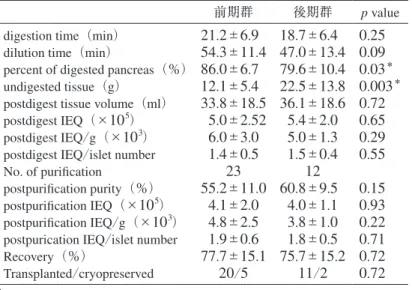
両群のドナー背景,グラフト背景を表 1,2 に示 す。ドナーの年齢,性別には差を認めなかったが, BMIは後期群で有意に高かった( p=0.03)。グラフト 背景としては前期群で全例心停止ドナーであった一 方,後期群では 1 例を除き脳死ドナーからの臓器提供 であった。グラフトの重量は前期群 89.9±26.1 g,後 期群 111.9±34.7 g( p=0.02)と後期群で有意に重く, 冷阻血時間は 284.6±86.1 min vs. 386.9±89.1 min と後 期群で有意に長かった(p=0.002)。 膵島分離成績の比較を表 3 に示す。digestion time, dilution timeにおいて両群間に有意差は認めなかった ( p=0.25,0.09)。消化された膵重量の割合は 86.0± 6.7% vs. 79.6±10.4%( p=0.03)と有意に前期群で有 意に高かったが,postdigest tissue volume は両群間で 差を認めなかった。postdigest IEQ や純化を行った数 は両群間で同等であった。post purification IEQ も両群 間で有意差を認めなかった。ロット毎の膵消化後成績 表 1 ドナー背景 前期群 後期群 p value No. of patients 25 13 Age(years) 43.6±15.9 45.5±13.0 0.91 Sex(male/female) 16/9 7/6 0.73 BMI 21.9±3.0 25.5±6.5 0.03* *p<0.05を図 1 にあげる。ロットごとの n 数が少なかったた め,それぞれの消化酵素におけるロット間の成績格差 を比較することは困難であったが,極端な違いは認め られなかった。 表 4 は両群における純化後の膵島サイズ分布の比 較である。純化後の膵島サイズは 200-250 μm におい て後期群で有意に多かったが,その他のサイズでは有 意差を認めなかった。 前期群,後期群の移植後の成績を図 2,表 5 に挙げ る。Hba1c は両群すべての患者において移植後 3 か月 の時点で改善を認めた。また移植後 3 か月の SUIT indexは両群間に有意差は認めなかった( p=0.69)。
IV.考 察
今回の検証で,臨床膵島移植における膵島分離用酵 素として Liberase MTF の使用開始以降も膵島分離成 績,移植成績は維持されており,膵島分離用酵素の変 更が本邦での臨床展開に悪影響を与えることなく,円 滑な臨床再開に寄与していたことが示唆された。Lib-erase HIは同種(他家)膵島移植に加え 12),慢性膵炎 に対する膵全摘後自家膵島移植においても広く臨床使 用されてきた 13)。しかし 2007 年,プリオン病感染の リスクが発覚し販売が中止され,本邦の臨床膵島移植 は中止された。2012 年からは Liberse MTF を用いて 臨床膵島移植が実施されている。これまで欧米におけ る両酵素を比較した報告はいくつか見られるが,本邦 の臨床膵島分離における両酵素の膵島分離に与える影 響を比較した報告はなく,本報告は,本邦初の臨床膵 島分離における膵島分離用酵素間の成績を比較したも のである。 2012 年より本邦の臨床膵島移植において使用が開 始された Liberase MTF はその製造工程に哺乳類・鳥 類由来成分が用いられておらず,さらに膵島分離に特 化した成分に高度に精製されたコラゲナーゼであり, Liberase HIに代わる膵消化酵素として開発された。欧 米では販売後早期よりヒト膵島分離に使用されてお り,Caballero-Corbalan らは 2010 年に Liberase MTF を 用いた臨床膵島分離で 12 例中 9 例において移植条件 (≧250,000IEQ,stimulation index≧1,viability≧78%) を満たしたと世界で初めて報告した 14)。その中で著者 らは Liberase MTF は他の消化酵素に比べ消化時間を 短縮したことを報告している 14)。また Meirigeng Qi らは Liberase HI,collagenaseNB1/neutral
protease,Liber-ase MTFそれぞれの臨床膵島分離成績を後方視的に比
表 2 グラフト背景
前期群 後期群 p value Cardiac/Brain 25/0 1/12 <0.001*
Graft weight(g) 89.8±26.1 111.9±34.7 0.02*
Warm ischemia time(min) 6.76±9.23 0.23±0.80 0.018*
Cold ischemia time(min) 284.6±86.1 386.9±89.1 0.002* *p<0.05
表 3 膵島分離結果
前期群 後期群 p value digestion time(min) 21.2±6.9 18.7±6.4 0.25 dilution time(min) 54.3±11.4 47.0±13.4 0.09 percent of digested pancreas(%) 86.0±6.7 79.6±10.4 0.03*
undigested tissue(g) 12.1±5.4 22.5±13.8 0.003*
postdigest tissue volume(ml) 33.8±18.5 36.1±18.6 0.72 postdigest IEQ(×105) 5.0±2.52 5.4±2.0 0.65
postdigest IEQ/g(×103) 6.0±3.0 5.0±1.3 0.29
postdigest IEQ/islet number 1.4±0.5 1.5±0.4 0.55 No. of purification 23 12
postpurification purity(%) 55.2±11.0 60.8±9.5 0.15 postpurification IEQ(×105) 4.1±2.0 4.0±1.1 0.93
postpurification IEQ/g(×103) 4.8±2.5 3.8±1.0 0.22
postpurication IEQ/islet number 1.9±0.6 1.8±0.5 0.71 Recovery(%) 77.7±15.1 75.7±15.2 0.72 Transplanted/cryopreserved 20/5 11/2 0.72
較検討し,Liberase MTF を用いた膵島分離は他酵素に 比べ膵消化効率と分離後膵島のインスリン分泌機能が 有意に優れていると報告した 15)。これらの報告は Lib-erase MTFが従来の消化酵素と比べても分離成績が維 持されると示唆されるものであり,本報告の分離結果 もそれと矛盾しない。 図 1 ロットごとの postdigest IEQ/g の比較 表 4 純化後の膵島サイズの比較 μm 50-100(%)100-150(%)150-200(%)200-250(%)250-300(%)300-350(%)350-400(%)>400(%) 前期群 33.4±10.5 36.3±7.1 16.9±6.3 6.9±3.0 3.7±2.9 1.4±1.2 0.7±0.9 0.5±0.7 後期群 29.1±9.6 32.2±5.5 21.8±9.4 11.3±4.4 3.5±0.9 1.3±0.7 0.4±0.7 0.5±0.7 p value 0.24 0.08 0.07 0.001* 0.75 0.64 0.26 0.80 *p<0.05 図 2 移植前,最終移植 3 か月後の Hba1c
臨床膵島移植の成績は近年向上しており,2016 年 に 北 米 の CITC(Clinical Islet Transplantation
Consor-tium)より報告された第 3 相多施設共同研究の結果で は,主要エンドポイント(Hba1c<7.0%)の達成率が 1年で 87.5%,2 年で 71%であった上に重症低血糖発 作回数を著明に改善している 16)。しかし,複数回の移 植を前提としている上,インスリン離脱率は移植後 1 年で 52.1%とエドモントンプロトコールが報告された 時期に比べ大きな向上は見られていない 9, 16)。現状で もインスリン離脱に必要な膵島量を確保するには複数 のドナーが必要とされており 17),分離効率向上のため さまざまな研究が進められている。 その一つとして,ドナー背景に合わせた分離酵素使 用法の改良が挙げられる。Miyazaki らはラットモデ ルを用い,系統間での膵臓組織におけるコラーゲン Ⅲ,コラーゲンⅤの発現の違いを示し,膵島分離酵素 における CollagenaseG,CollagenaseH 比の最適化が分 離成績の向上に寄与する可能性があると報告してい る 18)。また Loganathan らは若年ドナーからの膵島分離 は通常の消化酵素を使った場合,消化後も腺房細胞に 覆われた膵島の割合が多く収拾率が悪いことに注目 し,若年ドナーの膵島分離にプロテアーゼを多く使用 することより収量が増えることを報告した 19)。すなわ ち膵臓の細胞外マトリックスには個体差があり,ド ナー背景に応じて消化酵素の使用法を変えるにより膵 島分離成績が向上する可能性があると考えられる。 Liberase HIは,コラゲナーゼとプロテアーゼがすでに 配合された製剤で,コラゲナーゼとプロテアーゼの使 用割合を変えることはできなかったが,Liberase MTF はコラゲナーゼとプロテアーゼ(Thermolysin)が別 包されており,コラゲナーゼに対するプロテアーゼの 使用量を変更することが可能である。今後,本邦での ドナー背景因子が及ぼす膵島分離成績の影響がより明 らかになれば,欧米の知見を参考にドナー背景に応じ てプロテアーゼの量を変更するなどして膵島分離用酵 素の使用法を最適化することにより膵島分離成績の向 上に資する可能性がある。 また,今回の比較では,後期群で非消化組織量が増 加しているが,その要因としてグラフト膵臓の重量が 後期群で有意に重かったことが考えられる。膵臓の重 さに応じて酵素の量を変えることはしていなかったた め,膵重量あたりの酵素の力価が減少し,重い膵臓の 場合では未消化組織量が増加した可能性があると思わ れる。重い膵臓を消化する際には,酵素量を変更す る,あるいは消化時間をできるだけ延長する,といっ た膵消化法の工夫の必要性を示唆する結果であると思 われる。 2013 年より脳死ドナーからの膵島移植が可能と なったことを受けて,当院の膵島分離は脳死ドナーか らの提供が中心となった。心停止ドナーは比較的近距 離の施設からの提供に限られるが,脳死ドナーは全国 どの施設からの提供も可能であるという膵島提供体制 の背景から,脳死提供が中心となった後期群では冷阻 血時間(cold ischemia time)が延長した。一方,脳死 下提供では温阻血時間(warm ischemia time)が最小 限にとどめられる。温阻血時間は膵島移植の成績に影 響を及ぼすことが報告されており 20, 21),特に 30 分以 上温阻血時間が延長した場合は膵島の収量や viability を低下させると報告されている 22)。本研究では後期群 において温阻血時間が有意に短縮しているが,膵島収 量は前期群と同等の結果であった。これは前期群の温 阻血時間が 25 例中 23 例において 10 分以下と非常に 短いものであったため,膵島収量にほとんど影響を与 えなかった,もしくは与えたとしても後期群で有意に 延長した冷阻血時間によって相殺されたと考えられ る。温阻血時間のない脳死ドナーからの膵臓提供が安 定した膵島分離成績に寄与する可能性があると思われ るが,今後の症例の蓄積に基づいた解析が必要である。 表 5 両群における最終移植 3 か月後の SUIT index 前期群 後期群
patient No. transplanted islets(IEQ/kg) SUIT index patient No. transplanted islets(IEQ/kg) SUIT index
1 1.31×104 27.29 1 1.71×104 0.14 2 1.68×104 9.90 2 1.76×104 73.70 3 2.33×104 0.25 3 1.34×104 11.47 4 3.09×104 14.55 4 1.62×104 15.73 5 1.91×104 6.52 5 3.20×104 5.69 6 1.69×104 49.76 7 2.28×104 12.61 8 0.5×104 8.63
V.結 語
今回われわれは当院における臨床膵島分離成績を検 討し,膵島分離用酵素の変更やドナーの背景因子の変 化後も膵島分離成績が良好に維持されていることを示 した。2020 年 4 月より膵島移植が保険収載され,今 後膵島移植の実施数が増えることが期待される。しか し本邦でのドナー不足問題は依然解決の難しい問題で あり,膵島移植のための膵臓提供は大変貴重な機会で ある。貴重な膵臓からより良質で数の多い膵島を分離 することは,今後の膵島移植の発展において重要であ り,今後も膵島分離成績の改善に資する検討や工夫が 望まれる。 利益相反なし。 文 献1) Foster ED, Bridges ND, Feurer ID, et al. Improved health-related quality of life in a phase 3 islet trans-plantation trial in type 1 diabetes complicated by severe hypoglycemia. Diabetes Care 2018; 41: 1001︲ 1008.
2) Shapiro AM, Pokrywczynska M, Ricordi C. Clinical pancreatic islet transplantation. Nat Rev Endocrinol 2017; 13: 268︲277.
3) Shapiro AM, Ricordi C, Hering BJ, et al. International trial of the Edmonton protocol for islet transplantation. N Engl J Med 2006; 355: 1318︲1330.
4) Misawa R, Ricordi C, Miki A, et al. Evaluation of viable beta-cell mass is useful for selecting collage-nase for human islet isolation: comparison of collage -nase NB1 and liberase HI. Cell Transplant 2012; 21: 39︲47.
5) Saito T, Gotoh M, Satomi S, et al. Islet transplantation using donors after cardiac death: report of the Japan Islet Transplantation Registry. Transplantation 2010; 90: 740︲747.
6) Saito T, Anazawa T, Gotoh M, et al. Actions of the Japanese Pancreas and Islet Transplantation Associa -tion regarding transplanted human islets isolated using Liberase HI. Transplant Proc 2010; 42: 4213︲4216. 7) 伊藤泰平,明石優見,剣持 敬.膵島移植症例報
告(2017).移植 2017; 52: 169︲177.
8) Matsumoto S, Rigley TH, Qualley SA, et al. Efficacy of the oxygen-charged static two-layer method for short-term pancreas preservation and islet isolation from nonhuman primate and human pancreata. Cell Transplant 2002; 11: 769︲777.
9) Shapiro AM, Lakey JR, Ryan EA, et al. Islet trans-plantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppres-sive regimen. N Engl J Med 2000; 343: 230︲238. 10) Matsumoto S, Okitsu T, Iwanaga Y, et al. Successful
islet transplantation from nonheartbeating donor pancreata using modified Ricordi islet isolation method. Transplantation 2006; 82: 460︲465.
11) Noguchi H, Yamada Y, Okitsu T, et al. Secretory unit of islet in transplantation (SUIT) and engrafted islet rate (EIR) indexes are useful for evaluating single islet transplantation. Cell Transplant 2008; 17: 121︲128.
12) Brandhorst H, Friberg A, Nilsson B, et al. Large-scale comparison of Liberase HI and collagenase NB1 utilized for human islet isolation. Cell Transplant 2010; 19: 3︲8.
13) Anazawa T, Balamurugan AN, Bellin M, et al. Human islet isolation for autologous transplantation: compar -ison of yield and function using SERVA/Nordmark versus Roche enzymes. Am J Transplant 2009; 9: 2383︲2391.
14) Caballero-Corbalan J, Brandhorst H, Asif S, et al. Mammalian tissue-free liberase: a new GMP-graded enzyme blend for human islet isolation. Transplanta-tion 2010; 90: 332︲333.
15) Qi M, Valiente L, McFadden B, et al. The choice of enzyme for human pancreas digestion is a critical factor for increasing the success of islet isolation. Transplant Direct 2015; 1.
16) Hering BJ, Clarke WR, Bridges ND, et al. Phase 3 trial of transplantation of human islets in type 1 diabetes complicated by severe hypoglycemia. Diabetes Care 2016; 39: 1230︲1240.
17) de Kort H, de Koning EJ, Rabelink TJ, et al. Islet transplantation in type 1 diabetes. BMJ 2011; 342: d217.
18) Miyazaki Y, Murayama K, Fathi I, et al. Strategy towards tailored donor tissue-specific pancreatic islet
isolation. PLoS One 2019; 14: e0216136.
19) Loganathan G, Subhashree V, Narayanan S, et al. Improved recovery of human islets from young donor pancreases utilizing increased protease dose to colla -genase for digesting peri-islet extracellular matrix. Am J Transplant 2019; 19: 831︲843.
20) Boker A, Rothenberg L, Hernandez C, et al. Human islet transplantation: update. World J Surg 2001; 25:
481︲486.
21) Corlett MP, Scharp DW. The effect of pancreatic warm ischemia on islet isolation in rats and dogs. J Surg Res 1988; 45: 531︲536.
22) Tanioka Y, Hering BJ, Sutherland DE, et al. Effect of pancreatic warm ischemia on islet yield and viability in dogs. Transplantation 1997; 64: 1637︲1641.