持続陽圧呼吸療法中の閉塞性睡眠時無呼吸症候群における一次性頭痛の合併頻 度とその治療効果
渡邉悠児
1),鈴木圭輔
1),宮本雅之
2),宮本智之
3),平田幸一
1)5
1) 獨協医科大学内科学(神経)
2)獨協医科大学看護学部看護医科学(病態治療)
3) 獨協医科大学越谷病院 神経内科
*Corresponding author:
10
鈴木 圭輔
獨協医科大学内科学(神経)
〒321-0293 栃木県下都賀郡壬生町北小林 880 TEL:0282-86-1111 (内 2721)
FAX:0282-86-5884
15
e-mail: [email protected]
文字数 要約 495 字,英文要旨字 239, 本文字 5,799 ,参考文献 27 ,図 3 ,表 2 Key words: obstructive sleep apnea syndrome, primary headache, continuous positive airway pressure, migraine, tension-type headache
20
欄外見出し: OSAS に伴う頭痛に対する CPAP の効果
要約
閉塞性睡眠時無呼吸症候群( obstructive sleep apnea syndrome, OSAS )に慢性頭痛 は高率に合併する.我々は OSAS における一次性頭痛の合併頻度と持続陽圧呼
25
吸 (continuous positive airway pressure, CPAP) 療法の効果について検討した.
CPAP 療法中の OSAS 患者 235 例(男性 190 例, 女性 45 例; 平均 54.8±11.6 歳)
を対象とした.一次性頭痛の診断は質問紙を参考に,面接法により国際頭痛分 類第 2 版 (International Classification of Headache Disorders, 2nd edition, ICHD-II) に基づいて行い,睡眠時無呼吸性頭痛の診断は ICHD-3beta を用いた. OSAS 235
30
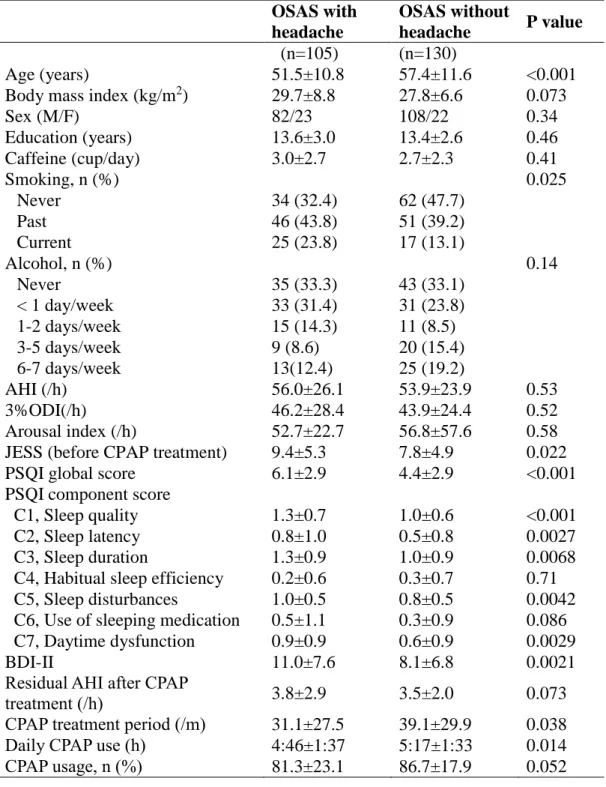
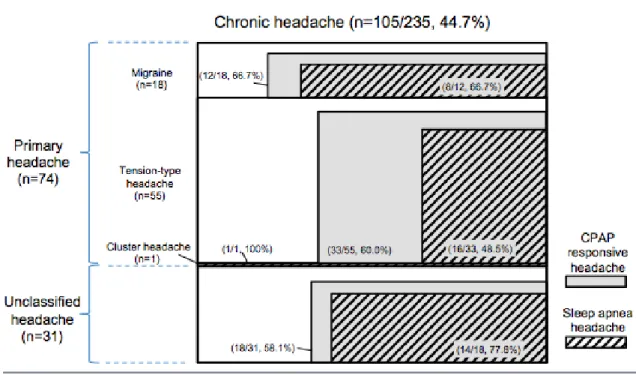
例中 105 例 (44.7%) に慢性頭痛があり,片頭痛 18 例 (7.7%) ,緊張型頭痛 55 例 (23.4%),群発頭痛 1 例 (0.4%), その他の頭痛 31 例 (13.0%)であった.頭痛のあ る群では,睡眠障害,日中の眠気,抑うつ症状が有意に認められた.慢性頭痛
105 例中 39 例 (37.1%) に睡眠時無呼吸性頭痛を認めた. CPAP 治療の効果があ
った片頭痛 12 例および緊張型頭痛 33 例のうち睡眠時無呼吸性頭痛の共存例は
35
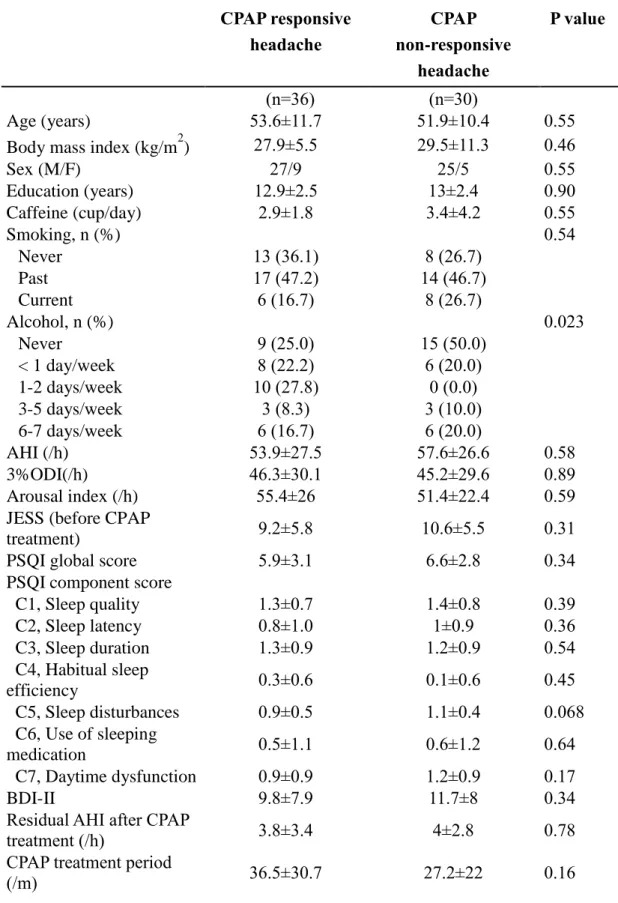
それぞれ 8 例 (66.7%),16 例 (48.5%) であった.頭痛のある OSAS 患者のうち 睡眠時無呼吸性頭痛を除外した 66 例の中で,頭痛に対して CPAP の効果があっ
た群 (n=36) では,頭痛に対して CPAP の効果がなかった群 (n=30) よりも一日の
CPAP 使用時間が有意に長かった.今回の検討では OSAS に慢性頭痛を高頻度に 合併したが,睡眠時無呼吸性頭痛の診断基準を満たさない一次性頭痛において
40
も CPAP 療法が有効な症例があることが明らかとなった.
Primary headaches in patients with obstructive sleep apnea syndrome receiving continuous positive airway pressure therapy
45
Yuji Watanabe
1), Keisuke Suzuki
1), Masayuki Miyamoto
2), Tomoyuki Miyamoto
3), Koichi Hirata
1)1)
Department of Neurology, Dokkyo Medical University
50
2)
Department of Clinical Medicine for Nursing, Dokkyo Medical University School of Nursing
3)
Department of Neurology, Dokkyo Medical University Koshigaya hospital
Abstract
55
Chronic headache is often comorbid with obstructive sleep apnea syndrome (OSAS).
We investigated the prevalence of primary headaches and also evaluated the effect of continuous positive airway pressure (CPAP) on the primary headaches. A total of 235 patients with OSAS (190 M, 45F; mean age 54.8±11.6 years) receiving CPAP therapy were participated in this study. Primary headaches were diagnosed according to the
60
International Classification of Headache Disorders, 2nd edition (ICHD-2). Sleep apnea headache was diagnosed based on ICHD-3 beta. Of 235 OSAS patients, chronic headaches were observed in 105 (44.7%): 18 migraines (7.6%); 55 tension-type headaches (23.5%); 1 cluster headache (0.4%) and 31 unclassified headaches (13.0%).
Patients with chronic headache showed higher scores for sleep disturbances, daytime
65
sleepiness and depressive symptoms compared with patients without chronic headache.
Of 105 patients with chronic headaches, 39 (37.1%) had sleep apnea headache. CPAP treatment was effective in reducing headaches in 12 patients with migraine (8 with comorbid sleep apnea headache, 66.7%) and in 33 patients with tension-type headache (16 with comorbid sleep apnea headache, 48.5%). Among OSAS patients with chronic
70
headaches after exclusion of patients with sleep apnea headache (n=66), CPAP-responsive headache group (n=36) had a significant longer daily CPAP use compared to CPAP-non responsive headache group (n=30). In patients with OSAS, chronic headache was frequently observed. Our study results showed that in patients with OSAS CPAP therapy can ameliorate concomitant primary headaches not fulfilling
75
the diagnostic criteria of sleep apnea headache.
はじめに
睡眠障害と頭痛はしばしば合併し,睡眠の分断や不眠が頭痛の原因となる一方
80
で,睡眠により頭痛が改善する場合もあることから,睡眠と頭痛の相互の密接 な関連性は以前より知られている
1).慢性頭痛は閉塞性睡眠時無呼吸症候群 (obstructive sleep apnea syndrome, OSAS) 患者の 15-50%に合併すると報告されて いる
2). また起床時頭痛は OSAS の随伴症状として, 18-60% の OSAS 患者でみ られる
3-6).そのうち,両側・圧迫性に生じ,持続時間が 30 分以内で OSAS の
85
適切な治療により消退する起床時頭痛は睡眠時無呼吸性頭痛として定義されて いる ( 国際頭痛分類第 2 版 , International Classification of Headache Disorders
(ICHD), second edition)
7).しかし,睡眠時無呼吸性頭痛では緊張型頭痛様の性質
の他,片頭痛様の性質を呈する場合もある
3). その後発刊された ICHD-3 beta 版の睡眠時無呼吸性頭痛の診断基準では持続時間が 30 分から 4 時間まで延長さ
90
れた
8).我々は持続陽圧呼吸療法中の OSAS 患者 235 例を対象に起床時頭痛を調 査し,睡眠時無呼吸性頭痛の ICHD-2 と ICHD 3-beta 版を用いて睡眠時無呼吸性 頭痛の頻度を調査した.その結果,起床時頭痛は全体の 20.4% にみられた.起床 時頭痛の 60.4% が ICHD-2 で, 81.3% が ICHD-3 beta で睡眠時無呼吸性頭痛と診断 され,ICHD-3beta の有用性が示された
7).しかし本邦において OSAS 患者におけ
95
る一次性頭痛の合併頻度や持続陽圧呼吸 (continuous positive airway pressure,
CPAP) の頭痛に対する効果は明らかにされていない.
本研究では CPAP 療法中の OSAS 患者における一次性頭痛の合併頻度を 調査し,CPAP 療法の頭痛に対する効果について検討した.
100
対象と方法
1. 対象
当院神経内科外来に通院している CPAP 療法中の OSAS 患者で,他の原発性睡
105
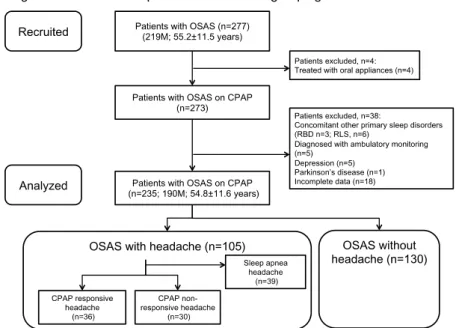
眠障害や神経・精神疾患などを除外した 235 例 (男性 190 例, 女性 45 例; 平均 54.8±11.6 歳 ) を対象に調査した (Fig.1) .
2. 方法
110
CPAP 療法中の OSAS 235 例 (男性 190 例, 女性 45 例; 平均 54.8±11.6 歳) を対象 に,頭痛と睡眠に関する質問紙を用いた横断調査を施行した. OSAS の診断は臨 床的に面接と診察の後に,睡眠ポリグラフ検査を施行して睡眠障害国際分類第 2 版に基づいて診断した
9). 呼 吸 イ ベ ン ト の 判 定 は American Academy
of Sleep Medicine の シ カ ゴ 基 準を用いて
10),睡眠時無呼吸低呼吸指数
115
(apnea hypopnea index, AHI), 3% 動脈血酸素飽和度低 下 指 数 (3% oxygen
desaturation index, 3%ODI) を含めた睡眠関連呼吸障害指標を解析した.覚醒反応
指数(arousal index)の判定は American Sleep Disorders Association の基準を用い
11)