徳島大学大学院救急集中治療医学(〒770-8503 徳島県徳島市蔵本町3-18-15) 受付日2017年 1 月 6 日 採択日2017年 5 月 1 日 要約:患者-人工呼吸器非同調(以下,非同調)は,人工呼吸中に見られる頻度の高い事象で ある。人工呼吸器のガス供給パターンと,患者の呼吸パターンにずれがある場合,非同調が 生じる。非同調は,ガス交換障害,肺過膨張,呼吸仕事量の増大,人工呼吸期間やICU滞在 期間の延長をきたし,患者予後への影響も指摘されているが,その認識は高いとは言えない。 非同調は,①患者の吸気努力に一致して人工呼吸器の送気が開始しない不適切なトリガー (オートトリガー,ミストリガー,二重トリガー,逆行性トリガー),②吸気から呼気へ転じ るタイミングのずれ(送気の早期終了,送気の終了遅延),③人工呼吸器の送気流量と患者の 吸気流量の過不足,の3つに大別される。ベッドサイドの医療者には,これら非同調の原因, グラフィックモニタ波形上の特徴,対処方法について深い理解が求められる。
Key words: ①mechanical ventilation, ②patient-ventilator asynchrony, ③respiratory mechanics
Patient-ventilator asynchrony
(患者-人工呼吸器非同調)
板垣 大雅 西村 匡司
Ⅰ.はじめに
人工呼吸は,適切な換気量の維持と酸素化の改善,
呼吸仕事量の軽減を目的とし,人工呼吸に至った病態
が改善するまで肺保護的に継続されなければならな
い
1)。最短で人工呼吸器からの離脱を図るのが理想で
あるが,様々な要因が人工呼吸器からの離脱を妨げる。
患 者 と 人 工 呼 吸 器 の 非 同 調(patient-ventilator
asynchrony; 以下,非同調)は人工呼吸器のガス供給
パターンと,患者の呼吸パターンにずれがある状態を
指し
2),呼吸仕事量の増大,患者快適性の低下,過剰鎮
静,ウィーニング過程での混乱,そして人工呼吸期間
の延長
3),4)などの原因となる(Table 1)
5),6)。非同調は
人工呼吸管理中を通して少なくとも25%の患者に生
じ る 頻 度 の 高 い 事 象 で あ る
3),4),7)。Blanchら は
asynchrony index(非同調イベント数/全呼吸数)が
10%以上の患者でICUおよび院内死亡率が有意に上
昇したと報告している
8)。
しかし,患者の吸気努力をモニタリングすることな
く,グラフィックモニタ波形から非同調を診断するこ
とは集中治療に習熟した医師でも容易ではない
9)。一
般的な人工呼吸モードにおける非同調の原因,グラ
フィックモニタ波形上の特徴,対処方法について紹介
する。
Ⅱ.患者-人工呼吸器非同調の種類と発生機序
非 同 調 は,① 不 適 切 な ト リ ガ ー(trigger
asynchrony),②吸気から呼気へ転じるタイミングの
ずれ(cycling asynchrony),③吸気流量の過不足(flow
asynchrony)の3つに大別される
7)。Thilleらは,62
名の患者で人工呼吸開始後早期に30分間グラフィッ
ク波形を解析し,非同調が毎分2.1回(中央値)発生し,
うち85%がミストリガー,13%が二重トリガーであっ
たと報告している
3)。個々の非同調の発生率は,観察
の時期や期間,患者の吸気努力の程度や鎮静状態など
によって大きく左右されるが
6),ミストリガーが圧倒
的に頻度の高い非同調であることは,多くの研究で共
通している
3),10)〜13)。
1
)
不適切なトリガー(
trigger asynchrony
)
人工呼吸器の送気が患者の吸気努力と同時に開始し
ない非同調を指す。
①オートトリガー(auto-triggering)
(Fig. 1)
患者の吸気努力がないにもかかわらず行われる補助
換気である。気道内圧の変化を招くリーク
3),心拍変
動
14),人工呼吸器回路内の結露や気道内分泌物貯留
15)などが原因になる。不適切に鋭敏なトリガー感度も
オートトリガーを招く。患者不快の他,呼吸性アルカ
ローシスや内因性PEEPの悪化
16),脳死判定の遅れ
17)に繋がる。リークの生じやすい非侵襲的人工換気にお
いて最も頻度の高い非同調である
18)。
② ミストリガー(ineffective inspiratory efforts)
(Fig. 2)
患者の吸気努力が人工呼吸器をトリガーできず,補
助換気が伴わない非同調で,侵襲的人工換気で最も頻
度の高い非同調である
3),13)。不適切なトリガー感度や
減弱した吸気努力,過剰鎮静などによって起こり
19),
呼吸仕事量の増大,呼吸筋疲労を招く
4)。内因性
PEEPが原因となることが多い
13)。内因性PEEPは呼
気終末の肺胞内圧と近位気道内圧との圧較差であり,
動的肺過膨張によって生じる。気管支喘息や慢性閉塞
性 呼 吸 器 疾 患(chronic obstructive pulmonary
diseases, COPD)の気道閉塞,不適切な人工呼吸器設
定(過剰な呼吸回数や1回換気量,長い吸気時間)では,
呼気時間が短すぎて肺胞気をすべて呼出することがで
・Hypoxemia ・Lung over-distension and dynamic hyperinflation ・Increased work of breathing ・Patient discomfort and dyspnea ・Increased use of sedation and neuromuscular blocking agents ・Respiratory muscle dysfunction ・Prolongation of mechanical ventilation ・Clinician’s confusion(error in decision making) Adapted from reference 5 and 6. Fig. 1 Auto-triggering during pressure control ventilation White arrow indicates machine cycle falsely triggered by a signal caused by excessive water in ventilator circuit. After removal of the water(dotted line), saw-tooth pattern of the waveforms disappeared. Paw, airway pressure; V 4 , flow; VT, tidal volume. 0 2 4 6 8 10 12 14 16 18 20 22 0 2 4 6 8 10 12 14 16 18 20 22 0 2 4 6 8 10 12 14 16 18 20 22 30 20 10 0 -10 -20 120 90 60 30 0 -30 -60 -90 -120 1,000 800 600 400 200 0 -100P
aw cmH2OV
T mlV
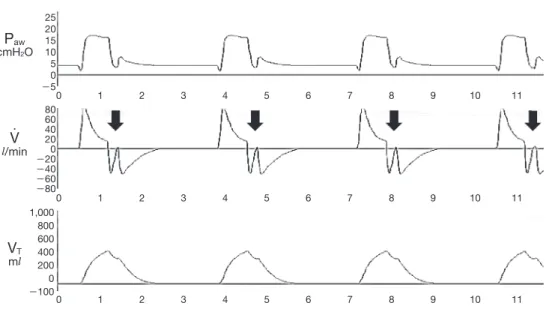
l/min ・Fig. 2 Ineffective inspiratory efforts during pressure control ventilation Black arrows indicate ineffective inspiratory efforts failed to trigger the ventilator. Paw, airway pressure; V 4 , flow; VT, tidal volume. 0 2 4 6 8 10 12 14 16 18 20 22 0 2 4 6 8 10 12 14 16 18 20 22 0 2 4 6 8 10 12 14 16 18 20 22 25 20 15 10 5 0 -5 80 60 40 20 0 -20 -40 -60 -80 200 160 120 80 40 0 -20
P
aw cmH2OV
T mlV
l/min ・きず,肺容量が少しずつ増加していく。内因性PEEP
は吸気開始時に呼気流を生じ,患者はこれを打ち消す
大きな吸気努力を要するが(Fig. 3),不十分である場
合,ミストリガーが生じる。
③二重トリガー(double triggering)
(Fig. 4)
1回の吸気努力の間に連続して2回補助換気が行わ
れることをいう。患者の吸気時間が設定吸気時間より
も長い場合,最初の補助換気終了後も持続した吸気努
力が別の補助換気をトリガーする。2つの補助換気を
隔てる呼気時間が極めて短いため,1回換気量が増加
して肺過膨張のリスクが高まる
20)。
④逆行性トリガー(reverse triggering)
強制換気にトリガーされた規則的な横隔膜収縮であ
る。 古 く か ら 報 告 の あ る 現 象 で あ る が
21),22),
Akoumianakiら が 過 剰 鎮 静 下 のARDS(acute
respiratory distress syndrome)患者において認めら
れることを報告してから
23),非同調の一形態として注
目されている。臨床的な影響は不明であるが,二段呼
吸の誘発,プラトー圧の測定変動,酸素消費量の増大
などが問題視されている
24)〜26)。脳死患者における
報告もある
27)。
2
)
吸 気 か ら 呼 気 へ 転 じ る タ イ ミ ン グ の ず れ
(
cycling asynchrony
)
サイクリングとは,人工呼吸器が吸気相から呼気相
に転じることを指す。Cycling asynchronyは患者が
吸気を終えるタイミングでサイクリングしない非同調
である。
Fig. 3 The effects of intrinsic PEEP to trigger the ventilator
(a)At the beginning of inspiration, increased pressure in the alveolar(Palv)generates high
intrinsic PEEP(Palv-PEEP)and outward-directed
air flow(black arrow). Initial inspiratory effort of patient(white arrow)is consumed to overcome this flow.
(b)Increased PEEP(counter PEEP)decreases outward-directed flow and makes it easier for patient to trigger the ventilator. 15 5 PEEP Intrinsic PEEP=10 +counter PEEP Palv 15 12 PEEP↑ Intrinsic PEEP=3 Palv (a) (b)
Fig. 4 Double triggering during pressure control ventilation
Two ventilator-delivered cycles separated by a very short expiratory time occur within a single inspiratory effort of a patient. This results in increased tidal volume(area under the flow waveform). Paw, airway pressure; V 4 , flow. Fig. 5 Premature cycling Black arrows show where inspiratory effort continued after the end of the ventilator cycle. Paw, airway pressure; V 4 , flow; VT, tidal volume.
①送気の早期終了(premature cycling)
(Fig. 5)
送気終了時に患者の吸気努力が持続している場合を
いう。設定吸気時間が患者の吸気時間に比べて短い状
態であり,二重トリガーの原因となる
28)〜30)。
②送気の終了遅延(delayed cycling)
(Fig. 6)
患者が呼気に転じた後も送気が持続する場合に生じ
る
31)。呼気時間が短くなるにつれて動的肺過膨脹が
進行すると,ミストリガーが起こる
30),32)。
トリガーの遅れも送気の終了遅延をきたす。鈍いト
リガー感度設定,気道抵抗の上昇,圧トリガーで認め
られるが,内因性PEEPに打ち勝って人工呼吸器をト
リガーしなければならないCOPD患者などで顕著で
ある
13),33)。
0 4 8 12 16 20 0 -5 80 60 40 20 0 -20 -40 -60 -80V
l/min ・ 0 1 2 3 4 5 6 7 8 9 10 11 0 1 2 3 4 5 6 7 8 9 10 11 0 1 2 3 4 5 6 7 8 9 10 11 25 20 15 10 5 0 -5 80 60 40 20 0 -20 -40 -60 -80 1,000 800 600 400 200 0 -100P
aw cmH2OV
T mlV
l/min ・3
)
吸気流量の過不足(
flow asynchrony
)
Flow asynchronyは人工呼吸器の送気流量(供給)
と患者の吸気流量(需要)との間にミスマッチがある
非同調である。
①量規定換気におけるflow asynchrony(Fig. 7)
人工呼吸器の吸気流量が患者の吸気流量に満たない
場合,呼吸仕事量は増大する
34),35)。最大吸気流量と
流量パターン(矩形波,漸減波)が固定されている量規
定換気で頻度の高い非同調である。代謝の亢進(熱傷,
発熱,敗血症)や疼痛・不安などで吸気努力が著しく
増強している場合に生じやすい。
②圧制御換気におけるflow asynchrony
プレッシャーサポート換気(pressure support
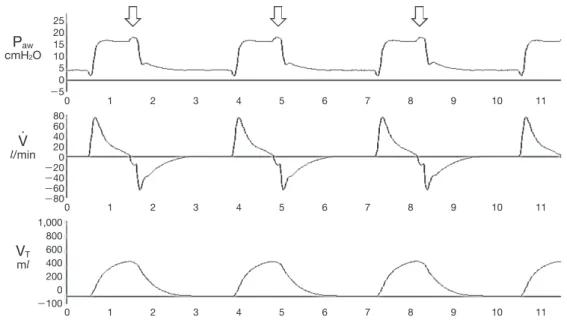
Fig. 6 Delayed cycling White arrows show “pressure spikes” where expiratory efforts began just before the end of the machine cycle. Paw, airway pressure; V 4 , flow; VT, tidal volume.
ventilation, PSV)やプレッシャーコントロール換気
(pressure controlled ventilation, PCV)のような圧制
御換気における流量に関するパラメータに立ち上がり
時間(ライズタイム)がある。患者吸気努力に比べて
立ち上がり時間が遅い場合,呼吸筋のunloadingが不
十分となり,呼吸仕事量が増大する
36)。一方,早すぎ
る立ち上がり時間は患者不快を増し,PSVにおいて
0 1 2 3 4 5 6 7 8 9 10 11 0 1 2 3 4 5 6 7 8 9 10 11 0 1 2 3 4 5 6 7 8 9 10 11 25 20 15 10 5 0 -5 80 60 40 20 0 -20 -40 -60 -80 1,000 800 600 400 200 0 -100P
aw cmH2OV
T mlV
l/min ・ Fig. 7 Flow asynchrony during volume control ventilation Black arrows indicate scooped-out deflection of airway pressure waveform caused by low peak flow(30 l/min). Increased peak flow(60 l/min, after the dotted line)met the patient’s flow demand and eliminated the scooped appearance of airway pressure waveform. Paw, airway pressure; V 4 , flow; VT, tidal volume. 0 2 4 6 8 10 12 14 16 18 20 22 0 2 4 6 8 10 12 14 16 18 20 22 0 2 4 6 8 10 12 14 16 18 20 22 22 25 20 15 10 5 0 -5 120 90 60 30 0 -30 -60 -90 -120 1,000 800 600 400 200 0 -100P
aw cmH2OV
T mlV
l/min ・は,早期のサポート終了を招く
37)。
Ⅲ.非同調へのアプローチ
非同調は患者と人工呼吸器の吸気時間のミスマッチ
に由来するものが多いため,人工呼吸器の吸気時間を
見直すことが重要なアプローチとなる。
然のもしくは持続する呼吸回数の増加を認めた場合に
オートトリガーを疑う。気道内圧・流量波形の揺れは
人工呼吸器回路内の結露や分泌物貯留を示唆し,これ
ら原因の除去で患者は瞬時に快適性を取り戻す(Fig.
1)。診断的にトリガー感度を鈍くすることも行われる
が,上記原因が除去されていなければ,ミストリガー
のリスクが増大する。
②ミストリガー
呼気相において補助換気を伴わない流量や気道内圧
の変化が観察できる(Fig. 2)。呼気流量波形が基線に
戻らない場合,内因性PEEPの存在を疑う。初めに病
態を見極め,気管支拡張薬や分泌物除去によって呼気
流量を確保する。トリガー感度の調整と呼気時間が延
長する設定変更を行い,内因性PEEPの軽減を図る。
ただし,吸気時間の短縮に伴い,呼吸回数が増加する
場合があることに注意する
38)。また,内因性PEEPに
相当する分のPEEPを上乗せする(counter PEEP)こ
とでトリガーに要する呼吸仕事量を軽減できる(Fig.
3)。
③二重トリガー
極めて短い呼気で隔てられた連続する2つの吸気が
特徴である(Fig. 4)。初めに吸気時間を延長する設定
変更を行う。PSVへの変更も効果的とされる
19)。なお,
鎮静を深めることは二重トリガーの頻度を減少せ
ず
19),ミストリガーの頻度を増加する
39)。
④逆行性トリガー
強制換気の吸気相,吸気相から呼気相への移行部,
そして呼気相において,気道内圧の低下および流量の
増加が規則的に観察される。深鎮静を避け,補助換気
主体の人工呼吸とする。
2
)
吸気から呼気へ転じるタイミングのずれ
①送気の早期終了
流量波形において呼気時の凸状パターンが特徴的で
ある(Fig. 5)。この場合,吸気時間を延長させる設定
変更を行う。
②送気の終了遅延
長すぎる送気は呼気筋の収縮を誘発し,吸気終末に
気道内圧の上昇を認める(Fig. 6)。この場合,吸気時
間を短縮させる設定変更を行う。トリガー感度はオー
トトリガーを予防し,かつ最も鋭敏なレベルに設定す
る。
7)
。最大吸気流量を吸気努力に見合った分だけ増
量する。ただし,この設定変更は吸気時間の短縮を伴
うため,吸気時間を個別に設定でき,吸気流量が変動
するPCVへの変更も考慮する。
②圧制御換気におけるflow asynchrony
早すぎる立ち上がり時間は吸気開始時の気道内圧を
オーバーシュートさせる。一方,遅い立ち上がり時間
で は,設 定 圧 に 到 達 す る ま で の 時 間 が 延 長 す る。
PCV,PSVともに,気道内圧がオーバーシュートしな
い範囲で,最も早い立ち上がり時間を選択する。
Ⅳ.まとめ
患者-人工呼吸器非同調は日常頻繁に発生している
が,気づかれていないことも多い。しかし,非同調は
患者予後に影響を与える重要な問題である。人工呼吸
器のグラフィックモニタ波形や患者の呼吸様式を綿密
に観察すれば,多くの場合に発見可能である。医療者
には,グラフィックモニタ波形から非同調を適切に診
断し,対処できる知識が求められる。
本稿のすべての著者には規定されたCOIはない。 文 献1) Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med 2013;369:2126-36.
2) Kacmarek RM, Pirrone M, Berra L. Assisted mechanical ventilation: the future is now!. BMC Anesthesiol 2015;15: 110.
3) Thille AW, Rodriguez P, Cabello B, et al. Patient-ventilator asynchrony during assisted mechanical venti-lation. Intensive Care Med 2006;32:1515-22.
4) de Wit M, Miller KB, Green DA, et al. Ineffective triggering predicts increased duration of mechanical ventilation. Crit Care Med 2009;37:2740-5.
5) Pierson DJ. Patient-ventilator interaction. Respir Care 2011;56:214-28.
6) Epstein SK. How often does patient-ventilator asynchrony occur and what are the consequences?. Respir Care 2011;56:25-38.
7) Mauri T, Yoshida T, Bellani G, et al; PLeUral pressure working Group (PLUG—Acute Respiratory Failure section of the European Society of Intensive Care Medicine). Esophageal and transpulmonary pressure in the clinical setting: meaning, usefulness and perspectives. Intensive Care Med 2016;42:1360-73.
8) Blanch L, Villagra A, Sales B, et al. Asynchronies during mechanical ventilation are associated with mortality. Intensive Care Med 2015;41:633-41.
ventilator waveforms observation in detecting patient-ventilator asynchrony. Crit Care Med 2011;39:2452-7. 10) Mellott KG, Grap MJ, Munro CL, et al. Patient ventilator
asynchrony in critically ill adults: frequency and types. Heart Lung 2014;43:231-43.
11) Vitacca M, Bianchi L, Zanotti E, et al. Assessment of physiologic variables and subjective comfort under different levels of pressure support ventilation. Chest 2004;126:851-9.
12) de Wit M, Pedram S, Best AM, et al. Observational study of patient-ventilator asynchrony and relationship to sedation level. J Crit Care 2009;24:74-80.
13) Kondili E, Prinianakis G, Georgopoulos D. Patient-ventilator interaction. Br J Anaesth 2003;91:106-19. 14) I m a n a k a H , N i s h i m u r a M , T a k e u c h i M , e t a l .
Autotriggering caused by cardiogenic oscillation during flow-triggered mechanical ventilation. Crit Care Med 2000;28:402-7.
15) Georgopoulos D, Prinianakis G, Kondili E. Bedside waveforms interpretation as a tool to identify patient-ventilator asynchronies. Intensive Care Med 2006;32: 34-47.
16) Harboe S, Hjalmarsson S, Søreide E. Autocycling and increase in intrinsic positive end-expiratory pressure during mechanical ventilation. Acta Anaesthesiol Scand 2001;45:1295-7.
17) McGee WT, Mailloux P. Ventilator autocycling and delayed recognition of brain death. Neurocrit Care 2011;14:267-71.
18) Carteaux G, Lyazidi A, Cordoba-Izquierdo A, et al. Patient-ventilator asynchrony during noninvasive v e n t i l a t i o n : a b e n c h a n d c l i n i c a l s t u d y . C h e s t 2012;142:367-76.
19) Chanques G, Kress JP, Pohlman A, et al. Impact of venti-lator adjustment and sedation-analgesia practices on severe asynchrony in patients ventilated in assist-control mode. Crit Care Med 2013;41:2177-87.
20) Pohlman MC, McCallister KE, Schweickert WD, et al. Excessive tidal volume from breath stacking during lung-protective ventilation for acute lung injury. Crit Care Med 2008;36:3019-23.
21) Petrillo GA, Glass L. A theory for phase locking of respi-ration in cats to a mechanical ventilator. Am J Physiol 1984;246(3 Pt 2):R311-20.
22) Graves C, Glass L, Laporta D, et al. Respiratory phase locking during mechanical ventilation in anesthetized human subjects. Am J Physiol 1986;250(5 Pt 2):R902-9. 23) Akoumianaki E, Lyazidi A, Rey N, et al. Mechanical
ventilation-induced reverse-triggered breaths: a frequently unrecognized form of neuromechanical coupling. Chest 2013;143:927-38.
24) Branson RD, Blakeman TC, Robinson BR. Asynchrony and dyspnea. Respir Care 2013;58:973-89.
25) Murias G, de Haro C, Blanch L. Does this ventilated
patient have asynchronies? Recognizing reverse triggering and entrainment at the bedside. Intensive Care Med 2016;42:1058-61.
26) Sorichter S, Puschendorf B, Mair J. Skeletal muscle injury induced by eccentric muscle action: muscle proteins as markers of muscle fiber injury. Exerc Immunol Rev 1999;5:5-21.
27) Delisle S, Charbonney E, Albert M, et al. Patient-ventilator asynchrony due to reverse triggering occurring in brain-dead patients: clinical implications and physiological meaning. Am J Respir Crit Care Med 2016;194:1166-8. 28) Tokioka H, Tanaka T, Ishizu T, et al. The effect of breath termination criterion on breathing patterns and the work of breathing during pressure support ventilation. Anesth Analg 2001;92:161-5. 29) Chiumello D, Polli F, Tallarini F, et al. Effect of different cycling-off criteria and positive end-expiratory pressure during pressure support ventilation in patients with chronic obstructive pulmonary disease. Crit Care Med 2007;35:2547-52.
30) Gentile MA. Cycling of the mechanical ventilator breath. Respir Care 2011;56:52-60.
31) Parthasarathy S, Jubran A, Tobin MJ. Cycling of inspi-ratory and expiratory muscle groups with the ventilator in airflow limitation. Am J Respir Crit Care Med 1998;158(5 Pt 1):1471-8.
32) Younes M, Kun J, Webster K, et al. Response of ventilator-dependent patients to delayed opening of e x h a l a t i o n v a l v e . A m J R e s p i r C r i t C a r e M e d 2002;166:21-30.
33) Stell IM, Paul G, Lee KC, et al. Noninvasive ventilator triggering in chronic obstructive pulmonary disease. A test lung comparison. Am J Respir Crit Care Med 2001;164:2092-7.
34) Tobin MJ, Jubran A, Laghi F. Patient-ventilator inter-action. Am J Respir Crit Care Med 2001;163:1059-63. 35) de Wit M. Monitoring of patient-ventilator interaction at
the bedside. Respir Care 2011;56:61-72.
36) Murata S, Yokoyama K, Sakamoto Y, et al. Effects of inspiratory rise time on triggering work load during pressure-support ventilation a lung model study. Respir Care 2010;55:878-84.
37) Nilsestuen JO, Hargett KD. Using ventilator graphics to identify patient-ventilator asynchrony. Respir Care 2005;50:202-34.
38) Laghi F, Karamchandani K, Tobin MJ. Influence of venti-lator settings in determining respiratory frequency during mechanical ventilation. Am J Respir Crit Care Med 1999;160(5 Pt 1):1766-70.
39) Vaschetto R, Cammarota G, Colombo D, et al. Effects of propofol on patient-ventilator synchrony and interaction during pressure support ventilation and neurally adjusted ventilatory assist. Crit Care Med 2014;42:74-82.