は じ め に
巨大脳動脈瘤は破裂や mass effect による圧排などに よってその自然歴は不良であり,外科的治療介入が必要で
札幌禎心会病院 脳神経外科(受稿日 2018. 10. 1)(脱稿日 2019. 5. 9)〔連絡先:〒 065-0033 北海道札幌市東区北 33 条東 1 丁目 3-1 札幌 禎心会病院 脳神経外科 太田仲郎〕[Address correspondence: Nakao OTA, M.D., Ph.D., Department of Neurosurgery, Sapporo Teishinkai Hospital, 3-1, Higashi 1, Kita 33, Higashi-ku, Sapporo, Hokkaido 065-0033, Japan]
脳卒中の外科 49: 103 〜 110,2021
原 著
ある18).しかしながら,巨大脳動脈瘤は周囲重要構造を巻 き込んでいることが多く,治療介入に関しても非常に難易 度が高い2)10)17).そのため,治療戦略は動脈瘤の部位や周 辺構造との関係から柔軟に対応する必要がある.われわれ巨大動脈瘤に対する治療成績とその戦略
太田 仲郎,岡田 泰明,鈴木 陽祐,棚田 秀一,波多野勇人
橋本 集,近藤 智正,宮崎 貴則,木下 由宇,野田公寿茂
上山 博康,徳田 禎久,谷川 緑野
Surgical Strategy and Outcome of Giant Intracranial Aneurysms
Nakao OTA, M.D., Ph.D., Yasuaki OKADA, M.D., Yousuke SUZUKI, M.D., Syuichi TANADA, M.D.,Yuto HATANO, M.D., Atsumu HASHIMOTO, M.D., Tomomasa KONDO, M.D.,
Takanori MIYAZAKI, M.D., Yu KINOSHITA, M.D., Kosumo NODA, M.D., Hiroyasu KAMIYAMA, M.D.,
Sadahisa TOKUDA, M.D., and Rokuya TANIKAWA, M.D.
Stroke Center, Department of Neurosurgery, Sapporo Teishinkai Hospital, Sapporo, Hokkaido, Japan
Summary: Introduction: To evaluate the clinical outcomes and factors affecting the prognosis of giant aneurysms and to better establish the role of microsurgery with bypass in its management.
Materials and Methods: Forty-eight patients with surgically treated giant aneurysms were included in this study. A giant aneurysm is defined as an aneurysm with a maximum diameter of ≥25 mm. Poor outcomes were defined as modified Rankin scale scores of 3-6.
Results: The mean size of the aneurysms was 30.9 mm (range, 25.0-54.9 mm). In 38 (79.2%) patients, the aneurysms were completely occluded without residual aneurysms, eight (16.7%) patients had mi-nor aneurysm remnants, and two (4.2%) had incomplete occlusion. Two (1.3%) patients with giant basilar artery trunk aneurysms died due to rupture of the treated aneurysm. Bypass surgery was com-bined with microsurgery in 45 (93.8%) patients. Perforating artery infarction was observed postopera-tively in 18 (37.5%) patients, and poor outcomes were observed in 12 (25.0%) patients. Male sex (p=0.002; odds ratio [OR]: 10.000, [2.262-44.203]), perforating artery infarction (p=0.036; OR: 5.200, [1.277-21.181]), branches arising from the aneurysms (p=0.031; OR: 4.900, [1.219-19.689]), and loca-tion of the aneurysm (p=0.002) were significantly associated with poor outcomes.
Conclusion: Microsurgery with bypass is an acceptable treatment modality for several giant aneu-rysms. Infarction of the perforating artery remains an unsolved problem, for which additional surgical strategies are required.
Key words: ・ giant intracranial aneurysm ・ bypass surgery ・ complex aneurysm ・ protective bypass
Surg Cereb Stroke (Jpn) 49: 103-110, 2021
の治療成績を示し,治療戦略について考察する. 対象と方法 2012 年 4 月から 2018 年 4 月までの 7 年間で札幌禎心会 病院にて外科的に治療した巨大脳動脈瘤 48 例を対象とし た. 巨大脳動脈瘤は最大径 25 mm 以上と定義した.さらに, 一般に複雑動脈瘤の定義とされる4)①同部位への過去の治 療介入(手術または血管内手術)の有無,②血栓化,③高度 の石灰化,④動脈瘤の dome から皮質枝の流出の有無,⑤ 動脈瘤部位を評価した. 1.アウトカムの評価
アウトカムは modified Rankin Scale(mRS) 3 以上を予 後不良とし,術前 mRS 3 以上であった症例では 1 点以上 悪化したものを予後不良と定義した.予後は手術半年後時 点での評価とした. 動脈瘤アウトカムは,①完全;動脈瘤の完全消失,②残 存;3 mm 未満の微小な残存,③不完全;3 mm 以上の残 存と定義した. 2.外科的治療介入 外科的治療介入は,ネッククリッピング,トラッピン グ,近位または遠位母血管遮断に分類した.バイパス併用 の必要性は基本的に術前に判断し,瘤処置の前に protec-tive bypass として行った.その後さらに追加のバイパス を必要としたかどうか検討した. 3.統計解析
統計解析は IBM SPSS Statistics for Mac(version 24.0 ; IBM, Armonk, NY, USA)を使用した.p<0.05 を統計学的 に有意とした.
予後不良(mRS 3 以上)および穿通枝梗塞の有無を従属 変数として解析した.各連続変数は Shapiro-Wilk test を 用いて正規分布に従うかどうか検定し,正規分布に従う場 合は t test,そうでない場合は Mann-Whitney U test を用 いて解析を行った.順序変数は Mann-Whitney U test を 用い,各名義変数は Fisher’s exact test を用いて解析し た.単変量解析にて有意であった因子について,ロジス ティック回帰分析を用いて多変量解析を行った. 結 果 1.Baseline characteristics 巨大脳動脈瘤 48 例のうち破裂例は 2 例(4.2%),症候性 動脈瘤は 29 例(60.4%)に認めた.女性 34 例(70.8%),男性 14 例(29.2%),平均年齢は 61.1±15.5 歳(18-89 歳)であっ た.動脈瘤サイズは平均 30.9±6.9 mm(25.0-54.9 mm).動 脈瘤部位は内頚動脈 C1 部 5 例(10.4%),C2 部 6 例(12.5%), C3-C7 部 17 例(35.4%),中大脳動脈 5 例(10.4%),前大脳 動脈 1 例(2.1%),脳底動脈 8 例(16.7%),椎骨動脈 3 例 (6.3%),後大脳動脈 3 例(6.3%)であった.平均観察期間は 82.7 週.術後 6 カ月時点での poor outcome は 12 例(25.0%) に認めた.mortality 4.3%,morbidity 29.8%であった. 2.Complexity of the aneurysm
以前の治療介入は 2 例(4.2%),血栓化動脈瘤は 22 例 (45.8%),高度の石灰化は 6 例(12.5%),動脈瘤から皮質 枝の分岐は 15 例(31.3%)に認められた. 単 変 量 解 析 で は 男 性〔p=0.002;OR:10.000(2.262-44.203)〕,動脈瘤部位(p=0.002),動脈瘤 dome から皮質 枝の分岐〔p=0.031;OR:4.900(1.219-19.689)〕が 6 カ月後 poor mRS score と関連していた.一方で,動脈瘤サイズ は(25 mm 以上の巨大動脈瘤では)予後に差はなかった(p =0.329)(Table 1). 3.バイパス手術 バイパス術は 45 例(94.3%)に施行され,うち high-flow bypass 28 例(59.6 %),low-flow bypass 30 例(63.8 %)で あった.protective bypass は 46 例(95.8%)に行われてい た.
4.動脈瘤治療とアウトカム
動脈瘤治療はネッククリッピング 10 例(20.8%),proxi-mal clipping 11 例(22.9%),cervical IC ligation 18 例 (37.5 %),trapping 10 例(20.8 %)で あ っ た.suction and
decompression 法は 6 例(12.5%)に施行しており,動脈瘤 切除は 5 例(10.4%)に施行していた.動脈瘤部位と治療, アウトカムを Table 2 に示す. 術後穿通枝梗塞を 18 例(37.5%),皮質枝領域梗塞を 5 例 (10.4%),アプローチによる脳挫傷を 2 例(4.2%)に認めた. 動脈瘤は完全閉塞 38 例(79.2%),残存 8 例(16.7%),不 完全 2 例(4.2%)であった. 術 後 に 当 該 動 脈 瘤 破 裂 に よ る く も 膜 下 出 血 を 2 例 (4.2%)に認めた.いずれも脳底動脈瘤に対する近位部閉 塞術後 1 カ月以内に破裂し mRS 6 となった.観察期間 中,動脈瘤の画像上での明らかな再発増大例は認めなかっ た.一方で,2 例(4.2%)の内頚動脈海綿静脈洞部動脈瘤症 例に対して external carotid artery(EC)-radial artery graft (RAG)-M2 バイパス術,頚部内頚動脈遮断術後に 1 例は 三叉神経痛の悪化,1 例は複視の悪化にて再手術,trap-ping を行った.
(1.420-27.074)〕,cervical IC ligation〔p=0.002;OR: 0.500(0.361-0.693)〕,穿通枝梗塞〔p=0.036;OR:5.200 (1.277-21.181)〕が有意に予後と関連していた.一方で, 動脈瘤治療の完全性(p=0.231)は予後とは関連がなかった (Table 1).多変量解析では男性〔p=0.01,adjusted OR: 21.06(2.07-213.89)〕,脳底動脈瘤〔p=0.02,adjusted OR: 100.06(5.53-1810.68)〕が予後と関連していた(Table 3). 5.穿通枝梗塞と関連する因子
単変量解析では,皮質枝が動脈瘤から分岐(p=0.009, crude odds ratio 6.250,1.642-23.786)が有意に穿通枝梗 塞と相関し,治療法では頚部内頚動脈遮断〔p<0.001; OR:0.045(0.005-0.383)〕が穿通枝梗塞と有意に相関して いた.多変量解析では,動脈瘤からの皮質枝の分岐〔p= 0.045,adjusted OR:5.132(1.039-25.364)〕, 脳 底 動 脈 瘤 〔p=0.006,adjusted OR:26.218(2.519-272.899)〕および 内 頚 動 脈 C1 部 動 脈 瘤〔p=0.048,adjusted OR:12.126 (1.026-143.346)〕が穿通枝梗塞と関連していた(Table 4). 症 例
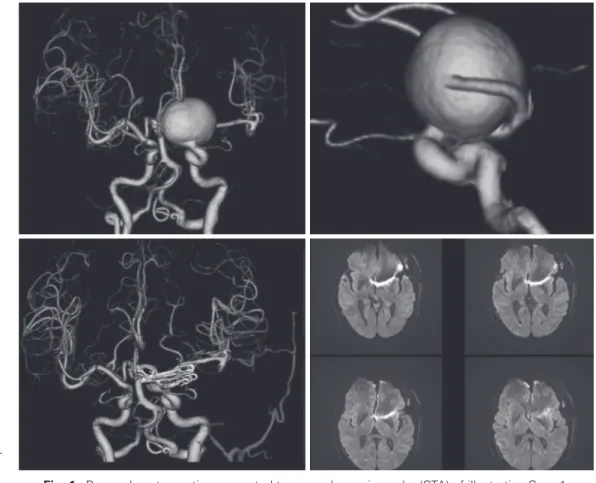
〈症例 1〉 内頚動脈瘤に対する superficial temporal artery (STA)-middle cerebral artery(MCA)bypass と suction
and decompression. 62 歳,女性.
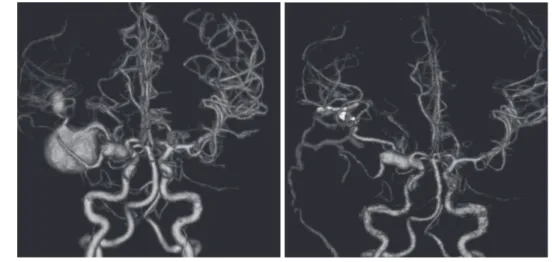
右同名半盲にて発見された左内頚動脈 C2 部巨大脳動脈 瘤(Fig. 1).STA-MCA bypass に よ る protective bypass を先行させた後に,上甲状腺動脈からの suction and de-compression 法にてクリッピングを施行した.遮断は 2 回 に分けて行い,それぞれ 7 分 5 秒と 8 分 47 秒であった. motor evoked potential(MEP)は,1 回目遮断時は 3 分 10 秒で消失(収縮期血圧 90 mmHg 台),2 回目は収縮期血圧 を 160 mmHg 程度に上げて遮断したことで遮断後 7 分で MEP 50%低下であった.遮断解除後 2 分で MEP 100%へ 復した.術後明らかな脳梗塞を認めなかった.一過性に右 不全麻痺を認めたが,リハビリテーションにて改善, mRS 1 で退院した.6 カ月後評価では視野も改善傾向を認 めていた.若干視野障害が残存のため mRS 1 で経過観察 中である. 〈症例 2〉 中大脳動脈瘤に対する protective bypass. 12 歳,女性. 頭痛で発見された未破裂右中大脳動脈紡錘状多発脳動脈 瘤(Fig. 2, 3).内頚動脈 C1 前脈絡叢動脈分岐直後から中 大脳動脈 M1,M2 superior trunk,M3 にかけての多発動 脈瘤を認めた.STA-MCA bypass 3 本によるすべての末 梢血管への血流補償を行ったのちに巨大血栓化動脈瘤をト ラッピングし,レンズ核線条体動脈が盲端化にならないよ う橈骨動脈グラフトを用いて M2 を再建した.動脈瘤ト ラッピングから M1-RAG-M2 バイパス開放まで 31 分 54 秒を要した.紡錘状で壁が厚い M1 動脈瘤は血栓化もなく 現時点では処理するリスクが高いと判断し温存し,M3 の 頭頂枝動脈瘤も末梢にバイパスをつないだのみで,今後の M1 動脈瘤が必要になった場合の逆行性血流の温存の目的 で処置しなかった.手術中一貫して MEP の低下は認めな Table 1 Baseline characteristics (n=48) and univariate
analy-sis of poor outcomes 6 months after surgery Variables Good (n=36) Poor (n=12) p value Age* 60.0 (±15.2) 64.3 (±16.5) 0.093 Sex† F 30, M 6 F4, M 8 0.002 Complexity of Aneurysm Symptomatic AN† 23 (63.9%) 6 (50.0%) 0.501 Size* 30.7 (±7.2) 31.7 (±6.5) 0.329 Previously treated† 0 2 (16.7%) 0.059 Thrombosed† 15 (41.7%) 7 (58.3%) 0.341 Calcification† 4 (11.1%) 2 (16.7%) 0.631
Branch arising from
AN† 8 (22.2%) 7 (58.3%) 0.031 Location of AN* C1 4 (11.1%) C1 1 (8.3%) 0.002 C2 6 (16.7%) C2 0 C3-7 17 (47.2%) C3-7 0 MCA 3 (8.3%) MCA 2 (16.7%) ACA 1 (2.8%) ACA 0 BA 1 (2.8%) BA 7 (58.3%) VA 1 (2.8%) VA 2 (16.7%) PCA 3 (8.3%) PCA 0 Treatment Bypass surgery† 34 (94.4%) 11 (91.7%) 1.000 Neck clipping† 7 (19.4%) 3 (25.0%) 0.695 Proximal clipping† 5 (13.9%) 6 (50.0%) 0.018 Cervical IC ligation† 18 (51.4%) 0 0.002 Trapping† 7 (19.4%) 3 (25.0%) 0.695 Radiographic findings Perforating artery infarction† 10 (27.8%) 8 (66.7%) 0.036 Cortical infarction† 2 (5.6%) 3 (25.0%) 0.092 Brain Contusion† 2 (5.7%) 0 1.000 Outcome of AN* Complete 30 (83.3%) Residual 5 (13.9%) Incomplete 1 (2.8%) Complete 8 (62.5%) Residual 3 (25.0%) Incomplete 1 (8.3%) 0.231
*Mann-Whitney U test, †Fisher’s exact test
MCA: middle cerebral artery, ACA: anterior cerebral artery, BA: basilar artery, VA: vertebral artery, PCA: posterior cerebral artery
Table 2 Treatment and outcomes of giant aneurysms based on location
Aneurysm
location (n=48) Treatment Bypass Perforating artery infarction (n=18) Poor outcome (n=12) ICA C3-C7 (n=17) Cervical IC ligation (n=17) STA-MCA and EC-M2 (n=17) 1 (5.9%) 0
ICA C2 (n=6) 2 (33.3%) 0 Case 1 Trapping STA-MCA and EC-M2 0 0 Case 2 Cervical IC ligation STA-MCA and EC-M2 0 0 Case 3 Trapping STA-MCA and EC-M2 1 0 Case 4 Neck clipping STA-MCA and EC-M2 0 0 Case 5 Neck clipping and
proximal clipping STA-MCA and EC-M2 0 0 Case 6 Neck clipping STA-MCA 1 0 ICA C1 (n=5) 4 (80%) 1 (20%)
Case 1 Trapping STA-MCA and EC-M2 1 0 Case 2 Neck clipping STA-MCA 1 0 Case 3 Cervical IC ligation STA-MCA and EC-M2 0 0 Case 4 Neck clipping STA-MCA and EC-M2 1 1 Case 5 Neck clipping STA-MCA and EC-M2 1 0 MCA (n=5) 2 (40%) 2 (40%)
Case 1 Proximal clipping (n=1) STA-MCA 0 0 Case 2 Trapping (n=1) STA-MCA and M1-M2 in situ* 0 0
Cases 3-5 Trapping (n=3) STA-MCA 2 2 ACA (n=1) Clipping STA-ACA and A3-A3 0 0 PCA (n=3) 2 (66.6%) 0 Case 1 Proximal clipping STA-PCA 1 0 Case 2 Trapping OA-calcarine, P2P-inferior
temporal artery in situ* 1 0
Case 3 Proximal clipping OA-calcarine 0 0
BA (n=8) 7 (87.5%) 7 (87.5%) postoperative rupture (n=2)
Case 1 Neck clipping STA-SCA 1 1 Case 2 Neck clipping None 0 1 Case 3 Proximal clipping V3-SVG-P2, STA-SCA and
STA-PCA 1 1 Case 4 Proximal clipping STA-SCA, STA-PCA 1 1 Case 5 Proximal clipping STA-PCA and STA-SCA 1 1 Case 6 Trapping OA-AICA, V3-RAG-P2 1 1 Case 7 Proximal clipping STA-SCA, STA-PCA 1 1 Case 8 Neck clipping STA-SCA 1 0 VA (n=3) 0 2 (66.6%)
Case 1 Proximal clipping V3-RAG-V3 and OA-PICA 0 1 Case 2 Proximal clipping OA-PICA 0 1 Case 3 Proximal clipping None 0 0
*bypass after repairing the aneurysm
To simplify the table, the items of MCA and ICA C3-7 are put in one in case of the treatment was the same.
ICA: internal carotid artery, STA-MCA: superficial temporal artery to middle cerebral artery bypass, EC: intra-operative patency of the extracranial, ACA: anterior cerebral artery, PCA: posterior cerebral artery, OA: occipital artery, BA: basilar artery, SCA: superior cerebellar artery, SVG: saphenous vein graft, AICA: anterior inferior cerebellar artery, RAG: radial artery graft
Table 3 Multivariate logistic regression analysis of the poor outcomes
Variable Significant probability (p) Crude odds ratio Adjusted odds ratio (95%CI) Male sex 0.010 10.000 21.057 (2.073-213.892) BA aneurysm 0.002 49.000 100.063 (5.530-1810.679) Model chi-square test p<0.001, percentage of correct classification 87.5%.
BA: basilar artery
Table 4 Multivariate logistic regression analysis of perforating artery infarction
Variable Significant probability (p) Crude odds ratio Adjusted odds ratio (95%CI) Branches arising from AN dome 0.045 6.250 5.132 (1.039-25.364) BA aneurysm 0.006 18.455 26.218 (2.519-272.899) C1 aneurysm 0.048 8.286 12.126 (1.026-143.346) Model chi-square test p<0.001, percentage of correct classification 81.3%.
BA: basilar artery
Fig. 1 Pre- and postoperative computed tomography angiography (CTA) of illustrative Case 1. A: Preoperative CTA showing a giant aneurysm on the C2 segment of the left internal
carotid artery.
B: Posterior communicating artery identified just distal to the aneurysm. C: Postoperative CTA shows complete neck clipping.
D: Postoperative diffusion weighted image does not show any high signal intensity. A B
Fig. 2 Pre- and postoperative computed tomography angiography (CTA) of illustrative Case 2. A: Preoperative CTA showing multiple aneurysms on the right side of the internal
ca-rotid artery to the distal middle cerebral artery.
B: Postoperative CTA showing good filling of the superficial temporal artery bypasses
and reconstructed M2 superior trunk.
A B
Fig. 3 Intraoperative findings and operative schema.
A: Intraoperative findings of the middle cerebral artery aneurysms.
B: Intraoperative findings showing the reconstructed M2 superior trunk and superficial
temporal artery to middle cerebral artery (STA-MCA) bypasses.
C: Schematic image of the preoperative condition. D: Schematic image of the final surgical results.
STA AN 4 M2 RAG M2 M2 inferior trunk STA STA LSAs A1 ICA M2 M2 M2 inferior trunk M1 M1 LSAs A1 ICA AN 3 AN 2 AN 1 STA STA RAG AN 4 AN 3 AN 3 AN 2 AN 1 A B C D
かった. 術後経過は良好で,mRS 0 で退院した. 考 察 Spetzlar らは 2008 年に複雑動脈瘤を① 25 mm 以上,② 動脈瘤部位,③以前の治療介入の有無,④側副血行の有 無,⑤血栓化,⑥石灰化病変と定義し報告した4).当院の 複雑動脈瘤治療成績では,動脈瘤部位,特に脳底動脈瘤お よび穿通枝梗塞が予後不良の危険因子であった16).穿通枝 梗塞の危険は動脈瘤部位によって規定される.今回われわ れの巨大脳動脈瘤結果をまとめると,予後不良は,男性, 動脈瘤部位,動脈瘤から皮質枝の分岐と関連しており,そ の予後不良の原因は穿通枝梗塞であるといえる.治療内容 では,proximal clipping 群で予後が悪く,cervical IC liga-tion 群では予後が良好であった.これは,内頚動脈海綿静 脈洞部瘤は EC-RAG-M2 バイパスを併用した cervical IC ligation で安全に治療が可能であり,穿通枝障害も生じな い.一方で,皮質枝が動脈瘤から分岐する,つまり椎骨・ 脳底動脈および内頚動脈 C1 部,中大脳動脈および前交通 動脈,後交通動脈などはその穿通枝梗塞リスクも高くな り,同じ穿通枝梗塞でも特に内頚動脈 C1 部,脳底動脈瘤 では 1 本の穿通枝の閉塞で重篤な症状になるリスクが高い ためと考えられる.バイパス手技の浸透と向上により皮質 枝領域の大梗塞をきたすことはほぼなくなり,そのため側 副血行路の有無や血栓化,石灰化はその治療難易度が上が るにせよ,それ自体予後不良因子といえなくなってきてい ると考えられる. 1.Protective bypass の有効性 上に述べたような複雑動脈瘤の予後因子の変化は pro-tective bypass の有効性を示していると考えられる.pro-tective bypass の概念は,最終的な動脈瘤修復のできあが りによるのではなく,遮断時間の予測がつかない場合にい かに末梢の虚血負荷なく,かつ安全確実に動脈瘤を修復す るかというものである14).すなわち,最終形をみればネッ ククリッピングや母血管温存が可能で,順行性血流を残す ことができる場合もあり得る.この場合にも,結果として バイパスがいらなかった場合や,最終形としては必要な かったが動脈瘤修復の遮断時間は長く有用であった場合に 分けられる.これらは術者の経験や技術,術前の予測によ りバイパス適応が変化するともいえるが,いずれにせよ結 果的に患者に障害がないのであればバイパスの過剰適応で はなく,安全な手術戦略を採用したと考えられる.これら protective bypass に基づいた動脈瘤治療は,前大脳動脈 瘤に対する STA-anterior cerebral artery(ACA)bypass や A3-A3 bypass14),後大脳動脈瘤に対する STA-posterior
cerebral artery(PCA)bypass や occipital
artery(OA)-PCA bypass15),本報告における内頚動脈,中大脳動脈瘤 に対する EC-MCA bypass など,動脈瘤を処理する前に 大部分の末梢血流の補償を終えているという意味で完成さ れた安全性の高い治療といえる.後に残る課題は,いかに 穿通枝を温存するかという点である. 2.穿通枝温存の課題 protective bypass によって末梢血流が補償され,遮断 時間の制限がほぼなく動脈瘤処置が可能となる.その分, 丁寧に穿通枝の剝離温存が可能となるが,それだけでは不 十分である.盲端化による遅発性血栓化や5)7)8)15),動脈瘤 自体から穿通枝が流出する場合の問題が未解決である.盲 端化による遅発性血栓化を避けるためには流出血管をつく ることが有用と考えられるが,一般化できるものではな い.さらに,穿通枝はわれわれの経験では虚血負荷に弱 く16),順行性血流をバイパスで再建しても遮断範囲に穿通 枝があった場合にはその穿通枝の温存ができるかどうかは 不明確であり,計画して行うべきものではない.これら穿 通枝温存にはおそらく症例 2 に示したように“根治”にこ だわらず手術の引き際と長期的な視点に立った治療介入が 必要になるのではないかと考えられる. 3.血管内治療について 近年,血管内治療による脳動脈瘤治療は術者の経験の蓄 積,デバイスの進歩によって,巨大動脈瘤に対しても部位 によっては比較的良好であるという報告がなされてい る3)6).末梢の巨大脳動脈瘤などは,単純な血管内治療に よる母血管遮断で完治し梗塞もなかったという報告もあ る1).また,穿通枝のない海綿静脈洞以下の内頚動脈瘤な どは,形状が許せば flow diverter のよい適応となるであ ろう13).一方で,動脈瘤から穿通枝,重要な細動脈が出て いるような症例では,急激な血栓化で穿通枝梗塞をきたし 予後不良である.後方循環動脈瘤に対する flow diverter の成績が悪いのも,それが原因である12).結果がよい脳底 動脈瘤症例などは,たまたま血栓化部分から重要な穿通枝 が出ていなかったにすぎない,と考えるのが妥当と考えら れる.これは外科治療にもいえることであり,直視下に確 認し温存可能の症例以外でバイパス併用の母血管遮断など は,たまたま結果がよい,結果が悪い,ということにすぎ ない9)11)16).現在それを超える決定的な治療法はないが, 知見の蓄積,CFD 解析を併用し,根治を目指すのではな く動脈瘤の壁を安定化させ破裂させず長期的な視点で治癒 を目指す治療が,今後の目指すところと考えられる.
結 論 protective bypass を併用した巨大脳動脈瘤治療は安全 かつ有効な治療法である.穿通枝梗塞の問題はいまだ克服 できていない問題であり,これにはすぐに根治を求めるの ではなく,長期的な視野に立った治療とその戦略が重要と なり今後の課題である. 著者全員は日本脳神経外科学会への COI 自己申告を完 了しています.本論文の発表に関して開示すべき COI は ありません. 文 献
1) Demartini Z Jr, Matos LA, Dos Santos ML, et al: Endovascular therapeutic occlusion of the posterior cerebral artery: an op-tion for ruptured giant aneurysm in a child. Pediatr Neuro-surg 51: 199-203, 2016
2) Gewirtz RJ, Awad IA: Giant aneurysms of the anterior circle of Willis: management outcome of open microsurgical treat-ment. Surg Neurol 45: 409-420, 1996
3) Ha SW, Jang SJ: Clinical analysis of giant intracranial aneu-rysms with endovascular embolization. J Cerebrovasc Endo-vasc Neurosurg 14: 22-28, 2012
4) Hanel RA, Spetzler RF: Surgical treatment of complex intra-cranial aneurysms. Neurosurgery 62(6 Suppl 3): 1289-1297, 2008
5) Iwai T, Naito I, Shimaguchi H, et al: Angiographic findings and clinical significance of the anterior and posterior spinal arteries in therapeutic parent artery occlusion for vertebral artery aneurysms. Interv Neuroradiol 6: 299-309, 2000 6) Jahromi BS, Mocco J, Bang JA, et al: Clinical and
angiograph-ic outcome after endovascular management of giant intracra-nial aneurysms. Neurosurgery 63: 662-674, 2008
7) Kado K, Hirai S, Kobayashi S, et al: Potential role of the ante-rior spinal artery in preventing propagation of thrombus in a therapeutically occluded vertebral artery: angiographic stud-ies before and after endovascular treatment. Neuroradiology
44: 347-354, 2002
8) Kazumata K, Nakayama N, Nakamura T, et al: Changing treatment strategy from clipping to radial artery graft by-pass and parent artery sacrifice in patients with ruptured blister-like internal carotid artery aneurysms. Neurosurgery 10(Suppl 1): 66-72, 2014
9) Krisht AF, Kadri PA: Surgical clipping of complex basilar apex aneurysms: a strategy for successful outcome using the pretemporal transzygomatic transcavernous approach. Neu-rosurgery 56(2 Suppl): 261-273, 2005
10) Lawton MT, Spetzler RF: Surgical management of giant in-tracranial aneurysms: experience with 171 patients. Clin Neurosurg 42: 245-266, 1995
11) Lawton MT, Abla AA, Rutledge WC, et al: Bypass surgery for the treatment of dolichoectatic basilar trunk aneurysms: a work in progress. Neurosurgery 79: 83-99, 2016
12) Lv X, Yang H, Liu P, et al: Flow-diverter devices in the treat-ment of intracranial aneurysms: A meta-analysis and system-atic review. Neuroradiol J 29: 66-71, 2016
13) Miyachi S, Ohnishi H, Hiramatsu R, et al: Innovations in endo-vascular treatment strategies for large carotid cavernous aneurysms─The safety and efficacy of a flow diverter. J Stroke Cerebrovasc Dis 26: 1071-1080, 2017
14) Ota N, Tanikawa R, Miyama M, et al: Surgical strategy for complex anterior cerebral artery aneurysms: retrospective case series and literature review. World Neurosurg 87: 328-345, 2016
15) Ota N, Goehre F, Miyazaki T, et al: Bypass revascularization applied to the posterior cerebral artery. World Neurosurg 96: 460-472, 2016
16) Ota N, Matsukawa H, Noda K, et al: Evaluation of microsur-gery for managing giant or complex cerebral aneurysms: a retrospective study. World Neurosurg 115: e190-199, 2018 17) Piepgras DG, Khurana VG, Whisnant JP: Ruptured giant
in-tracranial aneurysms. Part II. A retrospective analysis of timing and outcome of surgical treatment. J Neurosurg 88: 430-435, 1998
18) Wiebers DO, Whisnant JP, Huston J 3rd, et al: Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 362: 103-110, 2003