千葉県こども病院における 2009 年から 2012 年の小児臨床検体由来 Haemophilus influenzae の抗菌薬感受性に関する検討
1)千葉県こども病院感染症科,2)同 検査科
星野 直
1)朽名 悟
1)澤田 恭子
2)佐藤 洋子
2)深沢 千絵
1)(平成 25 年 2 月 5 日受付)
(平成 25 年 5 月 20 日受理)
Key words : Haemophilus influenzae, child, drug-resistance
要 旨
2009〜2012 年に千葉県こども病院で小児臨床検体より分離されたHaemophilus influenzae 1,208 株の抗菌 薬感受性に関する検討を行った.その内訳は,β-lactamase 非産生 ampicillin(ABPC)感受性株(BLNAS)
が 461 株(38.2%),β-lactamase 非産生 ABPC 中等度耐性株(BLNAI)が 168 株(13.9%),β-lactamase 非 産生 ABPC 耐性株(BLNAR)が 462 株(38.2%),β-lactamase 産生 ABPC 耐性株(BLPAR)が 63 株(5.2%),
β-lactamase 産生 clavulanic acid!amoxicillin 耐性株(BLPACR)が 54 株(4.5%)であった.2000〜2003 年
(I 期)の 15.0% から 2004〜2008 年(II 期)の 32.7% に急増した BLNAR であったが,II 期から今回にか けて増加のペースは緩やかになっていた.しかし,I 期の 10.6% から II 期の 8.9% に減少していた BLNAI は,今回は増加に転じていた.全H. influenzaeに対する MIC90が低値であったのは,tosufloxacin(≦0.06μg! mL),tazobactam!piperacillin(≦0.13μg!mL)であり,BLNAR に対しても同様であった.BLNAR の増 加に伴い,I 期〜II 期に引き続きセフェム系薬の感受性低下を認めた.なお,b 型莢膜株(Hib)は 54 株(4.5%)
分離され,II 期の 6.3% から減少していた.特に,Hib ワクチンの主な接種対象である 0 歳および 1 歳児か らの検出率が 56.8% から 29.6% に低下しており,ワクチン接種率の向上に伴う変化と考えられた.非 b 型 莢膜株は 21 株(1,7%)であり,11 株が e 型,10 株が f 型であった.
〔感染症誌 87:581〜589,2013〕
序 文
Haemophilus influenzaeは小児細菌感染症の代表的 原 因 菌 で あ る.2000 年 以 降,β-lactamase-non-pro- ducing ampicillin(ABPC)-resistant strain(BLNAR)
の急増が認められており1),細菌性髄膜炎など各種感 染症の治療に難渋する例が増加している.2008 年か ら 2010 年にかけて,tazobactam!piperacillin(TAZ!
PIPC)1:8 製剤や tosufloxacin(TFLX),tebipenem- pivoxil の小児への使用が保険収載され,H. influenzae による感染症への投与が広く行われるようになった.
また,2008 年末には b 型莢膜株(Hib)に対する結合 型ワクチンの接種が開始された.このように,H. influ-
enzaeを取り巻く環境には変化が見受けられる.そこ
で,小児におけるH. influenzaeの薬剤耐性動向につい
て確認するため,過去 4 年間の抗菌薬感受性に関する 検討を行った.
対象と方法
千葉県こども病院において,2009〜2012 年の 4 年 間に臨床検体より分離され,抗菌薬感受性を測定した
H. influenzae 1,208 株を対象に,感受性結果ならびに
菌株の分離背景について後方視的に検討した.抗菌薬 感受性は,日本化学療法学会標準法に準拠した微量液 体希釈法2)により最少発育阻止濃度(minimum inhibi- tory concentration:MIC)を測定し,測定対象抗菌 薬 は ABPC,piperacillin(PIPC),clavulanic acid! amoxicillin(CVA!AMPC),TAZ!PIPC,cefditoren
(CDTR),cefotaxime(CTX),ceftriaxone(CTRX),
meropenem(MEPM),TFLX,chloramphenicol(CP)
の 10 薬剤とした.このうち TFLX については,院内 における MIC 測定メニューが変更された 2010 年 4 月 原 著
別刷請求先:(〒266―0007)千葉市緑区辺田町 579―1
千葉県こども病院感染症科 星野 直
Table 1 Characteristics and
description
Total No. (%) of isolates
No. of isolates
BLNAS BLNAI BLNAR BLPAR BLPACR
Total 1,208 (100) 461 168 462 63 54
Sex
Male 705 (58.4) 276 108 253 35 33
Female 503 (41.6) 185 60 209 28 21
Age (yr)
0 218 (18.0) 89 26 82 12 9
1 314 (26.0) 94 46 146 11 17
2-5 458 (37.9) 179 59 173 29 18
6<_ 218 (18.0) 99 37 61 11 10
Specimen type
Sputum 739 (61.2) 281 103 284 39 32
Nasal/rhinorrhea 135 (11.2) 56 19 46 5 9
Otorrhea 52 ( 4.3) 23 7 18 2 2
Pharynx/nasopharynx 222 (18.4) 72 31 96 13 10
Eye discharge 30 ( 2.5) 10 3 12 4 1
Blood 4 ( 0.3) 3 1 0 0 0
CSF 12 ( 1.0) 8 3 1 0 0
Other 14 ( 1.2) 8 1 5 0 0
Characteristics and description of 1,208 isolates of Haemophilus influenzae
BLNAS: β-lactamase-non-producing ampicillin-sensitive strain, BLNAI: β-lactamase-non-producing ampicillin- intermediately-resistant strain, BLNAR: β-lactamase-non-producing ampicillin-resistant strain, BLPAR: β-lac- tamase-producing ampicillin-resistant strain, and BLPACR: β-lactamase-producing clavulanic acid/ amoxicil- lin-resistant strain.
Fig. 1 Changes in distribution of Haemophilus influenzae classified according to am- picillin or clavulanic acid/amoxicillin resistance in 2000-2003, 2004-2008, and 2009- 2012
BLNAS: β-lactamase-non-producing ampicillin-sensitive strain, BLNAI: β-lactamase- non-producing ampicillin-intermediately-resistant strain, BLNAR: β-lactamase-non- producing ampicillin-resistant strain, BLPAR: β-lactamase-producing ampicillin-resis- tant strain, and BLPACR: β-lactamase-producing clavulanic acid/amoxicillin- resistant strain.
以降の 750 株を測定対象とした.βラクタマーゼ産生 能はニトロセフィン法により確認した.また,無菌部 位から分離された全株と,発育したコロニーがムコイ
ド様を呈した菌株については,スライド凝集法による 血清型の確認も併せて行った.
対 象 と な っ た 菌 株 は,Clinical and Laboratory
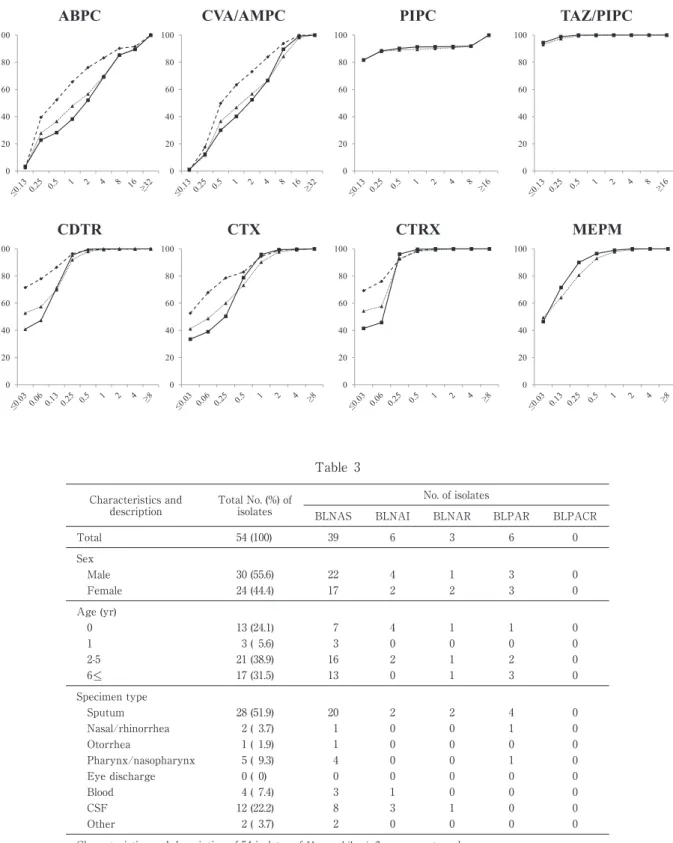
Fig. 2 Percentage distribution of antimicrobial susceptibility classified according to ampicillin or clavulanic acid/amoxicillin resistance, MIC50, and MIC90 of Haemophilus influenzae to penicillins
ABPC: ampicillin, PIPC: piperacillin, CVA/AMPC: clavulanic acid/amoxicillin, TAZ/PIPC: tazobactam/piperacil- lin, CDTR: cefditoren, CTX: cefotaxime, CTRX: ceftriaxone, MEPM: meropenem, TFLX: tosufloxacin, and CP:
chloramphenicol.
BLNAS: β-lactamase-non-producing ampicillin-sensitive strain, BLNAI: β-lactamase-non-producing ampicillin-inter- mediately-resistant strain, BLNAR: β-lactamase-non-producing ampicillin-resistant strain, BLPAR: β-lactamase- producing ampicillin-resistant strain, and BLPACR: β-lactamase-producing clavulanic acid/ amoxicillin-resistant strain.
Vertical axis: number of strains, horizontal axis: MIC (μg/mL).
Standard Institute(CLSI)の ABPC お よ び CVA!
AMPC の耐性基準3)により分類し,β-lactamase 非産 生株については,ABPC の MIC が 1μg!mL 以下の株 をβ-lactamase-non-producing ABPC-sensitive strain
(BLNAS),2μg!mL の株をβ-lactamase-non-producing ABPC-intermediately-resistant strain(BLNAI),4μg!
mL 以 上 の 株 を BLNAR と 定 義 し た.ま た,β- lactamase 産 生 株 に つ い て は,CVA!AMPC の MIC が 4μg!mL 以下の株をβ-lactamase-producing ABPC- resistant strain(BLPAR),8μg!mL 以 上 の 株 をβ- lactamase-producing CVA!AMPC-resistant strain
(BLPACR)と定義した.一部のデータについては,
当院における 2000〜2003 年4)(以下 I 期と記載)およ び 2004〜2008 年5)(以下 II 期と記載)のデータとの比 較を行った.有意差の検定は Fisher の直接検定法に より行い,p<0.05 を有意とした.
成 績
全 1,208 株の分離背景であるが,患者年齢別には 2〜
5 歳 458 株(37.9%),1 歳 314 株(26.0%),0 歳 お よ び 6 歳以上各 218 株(18.0%)の順に多く認めた.検 体別には,喀痰の 739 株(61.2%)が最多で,以下咽 頭・鼻咽頭 222 株(18.4%),鼻腔・鼻汁 135 株(11.2%)
と続き,無菌部位は髄液が 12 株(1.0%),血液が 4 株(0.3%)であっ た(Table 1).な お,細 菌 性 髄 膜 炎患者の髄液,血液の両部位から菌が検出された場合 は,髄液由来株のみを対象としたため,重複はしてい ない.
ABPC および CVA!AMPC 耐性度別の分離頻度を,
I 期,II 期 の 結 果 と 共 に 示 し た(Fig. 1).今 回 は,
BLNAS 38.2%,BLNAI 13.9%,BLNAR 38.2%,
BLPAR 5.2%,BLPACR 4.5% であり,BLNAS と BLNAR が同率であった.耐性度別分離頻度を経年的 に 見 る と,BLNAR は I 期 が 15.0%,II 期 が 32.7%,
今回が 38.2% であり,I〜II 期,II 期〜今回ともに有 意な増加を示したものの,増加のペースが緩やかと なっていた.I 期の 10.6% から II 期の 8.9% に減少し
Fig. 3 Percentage distribution of antimicrobial susceptibility classified according to ampicillin or clavulanic acid/amoxicillin resistance, MIC50, and MIC90 of Haemophilus influenzae to cephems and carbapenem
ABPC: ampicillin, PIPC: piperacillin, CVA/AMPC: clavulanic acid/amoxicillin, TAZ/PIPC: tazobactam/piperacil- lin, CDTR: cefditoren, CTX: cefotaxime, CTRX: ceftriaxone, MEPM: meropenem, TFLX: tosufloxacin, and CP:
chloramphenicol.
BLNAS: β-lactamase-non-producing ampicillin-sensitive strain, BLNAI: β-lactamase-non-producing ampicillin-inter- mediately-resistant strain, BLNAR: β-lactamase-non-producing ampicillin-resistant strain, BLPAR: β-lactamase- producing ampicillin-resistant strain, and BLPACR: β-lactamase-producing clavulanic acid/ amoxicillin-resistant strain.
Vertical axis: number of strains, horizontal axis: MIC (μg/mL).
て い た BLNAI は,13.9% と 増 加 に 転 じ て い た.
BLNAS は,I 期,II 期,今回の順に,65.5%,47.8%,
38.2% であり,I〜II 期,II 期〜今回ともに有意に減 少していた.βラクタマーゼ産生株の頻度は,8.8%,
10.6%,9.7% と 有 意 な 変 動 は な か っ た も の の,
BLPACR の頻度は 1.8%,3.7%,4.5% と微増傾向を 示し,I〜II 期にかけては有意差を認めた(Fig. 1).
H. influenzaeの各抗菌薬に対する感受性分布は Fig.
2〜4に 示 し た.MIC90(μg!mL)は,TFLX(≦0.06),
TAZ!PIPC(≦0.13),CDTR お よ び CTRX(0.25),
PIPC および MEPM(0.5)の順に優れていた.ABPC および CVA!AMPC 耐性度別の感受性分布に着目す ると,TAZ!PIPC と TFLX は耐性度に影響されず良 好な感受性を示した(Fig. 2,4).一方,CDTR,CTX,
CTRX,MEPM は,BLNAR と BLNAI を中心に低感 受性株が目立った.ま た,CDTR,CTX,CTRX の セフェム系 3 薬剤では,BLNAS が主体の感受性側の
ピークと,BLNAR と BLNAI が主体の耐性側のピー クを持つ,2 峰性の分布を呈した(Fig. 3).BLNAR に対する抗菌薬感受性については Table 2に示した.
MIC90(μg!mL)は,TFLX(≦0.06),TAZ!PIPC(≦
0.13),PIPC,CDTR,CTRX(0.25),MEPM(0.5)
の順に良好であった.
2000 年 以 降 のβラ ク タ ム 系 薬(ABPC,CVA! AMPC,PIPC,TAZ!PIPC,CDTR,CTX,CTRX,
MEPM)の MIC 累積百分率を,I 期を破線,II 期を 点線,今回を実線で示した(Fig. 5).なお,PIPC,TAZ!
PIPC,MEPM は,2004 年に MIC の測定メニューに 加わったため,II 期と今回のデータ比較のみ行った.
ABPC,CVA!AMPC,CDTR,CTX,CTRX の 5 薬 剤は,全期間を通じて感受性が低下していた.特に,
CDTR,CTX,CTRX の 3 薬 剤 で は,BLNAR の 増 加に伴う感受性株の減少を反映し,MIC が低値側の グラフが明らかに下方へシフトしていた.PIPC,TAZ!
Table 2 Antimicrobial
Agent
No. of isolates
MIC (μg/mL)
50% 90% Range
ABPC 462 8 16 4- >_ 32
PIPC 462 <_ 0.13 0.25 <_ 0.13-1
CVA/AMPC 462 8 16 2- >_ 32
TAZ/PIPC 462 <_ 0.13 <_ 0.13 <_ 0.13-0.5
CDTR 462 0.25 0.25 <_ 0.03-1
CTX 462 0.5 1 <_ 0.06- >_ 8
CTRX 462 0.25 0.25 <_ 0.03-1
MEPM 462 0.25 0.5 <_ 0.03-2
TFLX 334 <_ 0.06 <_ 0.06 <_ 0.06-1
CP 462 0.5 1 <_ 0.25-2
Susceptibilities of β-lactamase-non-producing ampicillin-resis- tant Haemophilus influenzae (BLNAR) to 10 antimicrobial agents ABPC: ampicillin, PIPC: piperacillin, CVA/AMPC: clavulanic acid/ amoxicillin, TAZ/PIPC: tazobactam/ piperacillin, CDTR:
cefditoren, CTX: cefotaxime, CTRX: ceftriaxone, MEPM: me- ropenem, TFLX: tosufloxacin, and CP: chloramphenicol.
Fig. 4 Percentage distribution of antimicrobial susceptibility classified according to ampicillin or clavulanic acid/amoxicillin resistance, MIC50, and MIC90 of Haemophilus influenzae to non-β-lactams
ABPC: ampicillin, PIPC: piperacillin, CVA/AMPC: clavulanic acid/amoxicillin, TAZ/PIPC: tazobactam/piperacil- lin, CDTR: cefditoren, CTX: cefotaxime, CTRX: ceftriaxone, MEPM: meropenem, TFLX: tosufloxacin, and CP:
chloramphenicol.
BLNAS: β-lactamase-non-producing ampicillin-sensitive strain, BLNAI: β-lactamase-non-producing ampicillin-inter- mediately-resistant strain, BLNAR: β-lactamase-non-producing ampicillin-resistant strain, BLPAR: β-lactamase- producing ampicillin-resistant strain, and BLPACR: β-lactamase-producing clavulanic acid/ amoxicillin-resistant strain.
Vertical axis: number of strains, horizontal axis: MIC (μg/mL).
PIPC,MEPM の 3 薬剤については,低感受性化は認 められなかった.
今回,無菌部位由来 16 株と,目視にてムコイド株 と判定された 59 株の計 75 株について,スライド凝集 法で血清型の判定を行った.75 株全てがいずれかの 血清型に分類され,16 株の全無菌部位由来株を含む 54 株(4.5%)が Hib で あ っ た(Table 3).患 者 年 齢 別 Hib 菌株数は,2〜5 歳が 21 株(38.9%)と最多で,次 いで 6 歳以上の 17 株(31.5%),0 歳 の 13 株(24.1%),
1 歳の 3 株(5.6%)の順であった.検体別には,喀痰 28 株(51.9%)が 最 多 で,髄 液 12 株(22.2%)が こ れに続き,以下咽頭・鼻咽頭 5 株(9.3%),血液 4 株
(7.4%)の順であった.耐性度別には BLNAS 39 株
(72.2%),BLNAI 6 株(11.1%),BLNAR 3 株(5.6%),
BLPAR 6 株(11.1%)であり,BLPACR の検出はな かった.なお,非 b 型莢膜株は 21 株(1,7%)であり,
無菌部位からの検出はなく,11 株が e 型,10 株が f 型に分類された.
考 察
当院では,1990 年代後半からH. influenzaeの抗菌 薬感受性サーベイランスを継続してきた4)〜6).1997〜
1999 年の検討では,H. influenzaeの ABPC 耐性は主 にβラクタマーゼ産生によるものであり,βラクタ マーゼ産生株が全H. influenzaeの 12.8% を占めたの に対し,BLNAR は 3% に過ぎなかった6).しかし,2000 年代に入ると,I 期には BLNAR がβラクタマーゼ産 生株を逆転し,II 期には完全に BLNAR が主体となっ た.抗菌薬耐性化の進行は,その消費量と相関するこ とが示されており7),penicillin-biding-protein(PBP)3 をコードするftsI遺伝子の変異により生じる BLNAR の増加は,セフェム系薬の多用に原因があると推測さ れている8).
今回,I 期,II 期から引き続き BLNAR が有意に増 加していたが,増加のペースは緩やかになっていた.1 年 毎 の 頻 度 は 2009〜2012 年 の 順 に 36.7%,41.7%,
Table 3 Characteristics and
description
Total No. (%) of isolates
No. of isolates
BLNAS BLNAI BLNAR BLPAR BLPACR
Total 54 (100) 39 6 3 6 0
Sex
Male 30 (55.6) 22 4 1 3 0
Female 24 (44.4) 17 2 2 3 0
Age (yr)
0 13 (24.1) 7 4 1 1 0
1 3 ( 5.6) 3 0 0 0 0
2-5 21 (38.9) 16 2 1 2 0
6<_ 17 (31.5) 13 0 1 3 0
Specimen type
Sputum 28 (51.9) 20 2 2 4 0
Nasal/rhinorrhea 2 ( 3.7) 1 0 0 1 0
Otorrhea 1 ( 1.9) 1 0 0 0 0
Pharynx/nasopharynx 5 ( 9.3) 4 0 0 1 0
Eye discharge 0 ( 0) 0 0 0 0 0
Blood 4 ( 7.4) 3 1 0 0 0
CSF 12 (22.2) 8 3 1 0 0
Other 2 ( 3.7) 2 0 0 0 0
Characteristics and description of 54 isolates of Haemophilus influenzae serotype b
BLNAS: β-lactamase-non-producing ampicillin-sensitive strain, BLNAI: β-lactamase-non-producing ampicillin- intermediately-resistant strain, BLNAR: β-lactamase-non-producing ampicillin-resistant strain, BLPAR: β-lac- tamase-producing ampicillin-resistant strain, and BLPACR: β-lactamase-producing clavulanic acid/ amoxicil- lin-resistant strain.
Fig. 5 Comparison of cumulative MICs of 8-β-lactams for Haemophilus influenzae between 2000-2003 (1,024 strains), 2004-2008 (1,317strains), and 2009-2012 (1,208strains)
ABPC: ampicillin, CVA/AMPC: clavulanic acid/amoxicillin, PIPC: piperacillin, TAZ/PIPC: tazobactam/piperacil- lin, CDTR: cefditoren, CTX: cefotaxime, CTRX: ceftriaxone, MEPM: meropenem.
Broken line: 2000-2003 (n=1,024), dotted line: 2004-2008 (n=1,317), and solid line: 2009-2012 (n=1,208).
Vertical axis: cumulative % of strains, horizontal axis: MIC (μg/mL).
38.8%,35.3% となっており,対象期間内に限定すれ ば BLNAR の増加は認められなかったことになる.
我々は,II 期の検討でも同様の傾向を確認しており,
2005 年以降は BLNAR の頻度が 30% 台前半から半ば で推移していた5).しかし,I 期から II 期にかけて減 少していた BLNAI が増加に転じた点にも注目しなく てはならない.Ubukata らは,ftsI遺伝子の 2 ヶ所に 変異を認める耐性度の強い株は,主に ABPC-MIC が 2μg!mL 以上に分布し,変異が 1 ヶ所の株に比べ,セ フェム系薬への感受性低下が強く認められることを報 告 し て い る9).今 回 の 感 受 性 分 布 よ り,BLNAI は BLNAR と同じようなセフェム系薬耐性を示してお り,ABPC-MIC の違いはあるが,両者は 同 一 のftsI 遺伝子変異を有する可能性が示唆される.BLNAR の βラクタム系薬耐性化の指標として,BLNAI の増減 にも注目すべきであろう.
I 期,II 期の検討結果4)5)と同様に,今回も CTX お よび CTRX の感受性低下が確認されたが,そのよう な中で PIPC,TAZ!PIPC,MEPM の 3 薬剤の経年的 な感受性低下は認められなかった.特に,PIPC と TAZ
!PIPC は BLNAR に 対 す る 感 受 性 が 非 常 に 良 好 で あったが,これは PIPC が高濃度存在下で PBP2 にも 結合するためと考えられている10).我々は,早くから この 2 剤を BLNAR 治療における key drug と考え,
気管支肺感染症に対する有用性を確認している11).今 回,βラクタマーゼの産生能とftsI遺伝子の変異を併 せ持つ BLPACR は微増傾向であったが,BLPACR 54 株の TAZ!PIPC に対する MIC は,52 株で≦0.13μg!
mL,2 株で 0.25 μg!mL と低値であり,今のところ経 年的な悪化も認めていない.TAZ!PIPC は,βラク タマーゼ産生株のカバーも必要な髄膜炎初期治療薬と しての有用性も高いものと考えられ,実際に Hib 髄 膜炎 5 例に対し 95.7〜113.6mg!kg!回を 1 時間で点滴 静注した場合,投与後 0〜40 分後の平均髄液中濃度は TAZ 1.08μg!mL,PIPC 6.42μg!mL と良好であった12).
今回最も感受性が優れていたのは TFLX であり,
BLNAR に対する MIC90も≦0.06μg!mL と低値であっ た.2009 年 10 月に小児肺炎,中耳炎への投与が保険 収載された TFLX は,難治化する小児耐性菌気道感 染症に対する経口治療薬の切り札的な位置づけにあ る.元々グラム陰性菌への抗菌活性が優れるフルオロ キノロンであるが,TFLX はグラム陽性菌,特にStrep- tococcus pneumoniaeへの感受性も良好であり,BLNAR やペニシリン耐性S. pneumoniae検出例を含む難治性 気 管 支 肺 感 染 症 治 療 に お け る 有 用 性 も 高 い13).H.
influenzaeのフルオロキノロン耐性株は,標的酵素で
ある DNA ジャイレースやトポイソメラーゼ遺伝子に 存 在 す る quinolone-resistance-determining region
(QRDR)の変異によって生じ,すでに本邦成人におけ る分離も認められている14).我々の検討では TFLX 耐性株は検出されず,MIC が 1μg!mL 以上を示した のも 3 株のみであった(1μg!mL が 2 株,2μg!mL が 1 株).しかし,ciprofloxacin に関する検 討 で,MIC 上は感受性を示す株の中に,QRDR の変異を有して いる株が少なからず存在することも報告されており,
フルオロキノロン耐性株の予備軍であると考えられて いる15).前述の通り TFLX の小児適用が追加承認さ れたことや,増加傾向が認められるマクロライド耐性
Mycoplasma pneumoniae感染症への投与が行われてい
る現状を考慮すると,小児におけるフルオロキノロン の投与量は確実に増えているものと予想される.した がって,フルオロキノロン耐性株の増加が懸念される が,小児呼吸器感染症診療ガイドラインでは,TFLX の肺炎初期治療薬としての使用を「耐性菌感染が疑わ れ,かつ amoxicillin あるいは広域セフェムの増量療 法が無効な場合」に限定している16).濫用は慎みたい.
2008 年 12 月 に 導 入 さ れ た Hib ワ ク チ ン は,2010 年末の公費助成開始により普及が進み,2011 年の Hib 侵襲性感染症罹患率は大幅に低下した17).当院におけ る Hib 分離率も,Hib ワクチン導入前に該当する II 期の 6.3% から,導入後を網羅した今回の 4.5% へ有 意な低下を認めた.検出数を 1 年毎に見てみると,2009 年は 24 株(8.2%),2010 年は 14 株(4.1%),2011 年 は 11 株(4.0%),2012 年は 5 株(1.7%)と減少傾向 であった.また,2 歳未満の Hib 分離頻度は,II 期の 56.8% から今回の 29.6% に有意に減少していた(p=
0.004).すなわち,主なワクチン接種対象である 0〜1 歳児を中心に Hib が減少していることは明らかであ り,ワクチン普及による保菌の減少を示唆するデータ と考えられる.なお,21 株(1.7%)の分離に留まっ た非 b 型莢膜株であるが,Hib の減少に伴いH. influ-
enzae侵襲性感染症における血清型の replacement が
生じることも懸念される.今後の検出頻度にも注目し たい.
利益相反自己申告:申告すべきものなし.
文 献
1)Sakata H, Toyonaga Y, Sato Y, Hanaki H, Nonoyama M, Oishi T,et al.:Nationwide sur- vey of the development of drug-resistance in the pediatric field : drug sensitivity ofHaemophi- lus influenzae in Japan. J Infect Chemother 2009;15:402―9.
2)日本化学療法学会,抗菌薬測定法検討委員会:
微量液体希釈法による MIC 測定法.Chemother- apy 1990;38:102―5.
3)Clinical and Laboratory Standards Institute.
Performance standards for antimicrobial suscep- tibility testing ; 17th informational supplement.
M100-S17. Clinical and Laboratory Standards In- stitute, Wayne, PA, 2007.
4)星野 直,須藤扶佐代,澤田恭子,末吉沙織,中
村 明:小児臨床検体由来Haemophilus influen- zaeの抗菌薬感受性に関する検討.感 染 症 誌 2004;78:943―51.
5)澤田恭子,佐藤洋子,有馬聖永,星野 直:2004 年から 2008 年の小児由来Haemophilus influenzae の抗菌薬感受性に関する検討.感染症誌 2010;
84:441―8.
6)Ohkusu K, Nakamura A, Sawada K:Antibiotic resistance among recent clinical isolates ofHae- mophilus influenzae in Japanese children. Diagn Microbiol Infect Dis 2000;36:249―54.
7)Austin DJ, Kristinsson KG, Anderson RM:The relationship between volume of antimicrobial consumption in human communities and the fre- quency of resistance. Proc Natl Acad Sci USA 1999;96:1152―6.
8)Hasegawa K, Kobayashi R, Takada E, Ono A, Chiba N, Morozumi M,et al.:High prevalence of type b β-lactamase-non-producing ampicillin- resistant Haemophilus influenzae in meningitis : the situation in Japan where Hib vaccine has not been introduced. Antimicrob Agents Che- mother 2006;57:1077―82.
9)Ubukata K, Chiba N, Hasegawa K, Shibasaki Y, Sunakawa K, Nonoyama M,et al.:Differentia- tion of β-lactamase-negative ampicillin-resistant Haemophilus influenzae from other H. influenzae by a disc method. J Infect Chemother 2002;8:
50―8.
10)Morikawa Y, Kitazato M, Mitsuyama J, Mizu- naga S, Minami S, Watanabe Y:In vitro activi- ties of piperacillin against β-lactamase-negative ampicillin-resistant Haemophilus influenzae. An- timicrob Agents Chemother 2004;48:1229―
34.
11)須藤扶佐代,石和田稔彦,星野 直,深沢千絵,
稲見由紀子,菱木はるか,他:小児Haemophilus influenzae気管支肺感染症に対する piperacillin,
tazobactam!piperacillin の 臨 床 効 果 に 関 す る 検 討.感染症誌 2005;79:637―43.
12)深沢千絵,朽名 悟,澤田恭子,佐藤洋子,星
野 直,石和田稔彦:Haemophilus influenzae細 菌性髄膜 炎 に お け る tazobactam!piperacillin の 髄液中濃度に関する検討.第 61 回日本感染症学 会東日本地方会学術集会口演.東京,2012.
13)星 野 直:小 児 に お け る 抗 菌 薬 の 争 点 2)
ニューキノロン系抗菌薬.感染と抗菌薬 2009;
12:136―41.
14)Yokota S, Ohkoshi Y, Sato K, Fujii N:Emer- gence of fluoroquinolone-resistant Haemophilus influenzaestrains among elderly patients but not among children. J Clin Microbiol 2008;46:
361―5.
15)Hirakata Y, Ohmori K, Mikuriya M, Saika T, Matsuzaki K, Hasegawa M,et al.:Antimicrobial activities of piperacillin-tazobactam againstHae- mophilus influenzae isolates, including β-lactama- se-negative ampicillin-resistant and β-lactamase- positive amoxicillin-clavulanate-resistant isolates, and mutation in their quinolone resistance- determining resions. Antimicrob Agents Che- mother 2009;53:4225―30.
16)日本小児呼吸器疾患学会,日本小児感染症学会
編:小児呼吸器感染症診療ガイドライン 2011.協 和企画,東京,2011.
17)庵原俊昭,菅 秀,浅田和 豊,富 樫 武 弘,細 矢光晃,陶山和秀,他:インフルエンザ菌 b 型
(Hib)ワクチンおよび 7 価肺炎球菌結合型ワク チン(PCV7)導入が侵襲性細菌感染症に及ぼす 効果について.病原微生物検出情報 2012;33:
71―2.
Antimicrobial Susceptibility ofHaemophilus influenzaeIsolated from Pediatric Patients at a Pediatric Facility between 2009 and 2012
Tadashi HOSHINO1), Satoru KUTSUNA1), Kyoko SAWADA2), Hiroko SATO2)& Chie FUKASAWA1)
1)Division of Infectious Diseases and2)Division of Clinical Laboratory, Chiba Childrenʼs Hospital
We examined the antimicrobial susceptibility of 1,208 Haemophilus influenzaeisolates obtained at a pedi- atric facility between 2009 and 2012. The percentage distribution of β-lactamase-non-producing ampicillin (ABPC)-sensitive (BLNAS) strains was 38.2%, that ofβ-lactamase-non-producing ABPC-intermediately resis- tant (BLNAI) strains was 13.9%, that of β-lactamase-non-producing ABPC-resistant (BLNAR) strains was 38.2%, that of β-lactamase-producing ABPC-resistant (BLPAR) strains was 5.2%, and that of β-lactamase- producing clavulanic acid!amoxicillin-resistant (BLPACR) strains was 4.5%. Although the percentage of BLNAR strains increased dramatically from 13.9% (2000-2003 ; period I) to 32.7% (2004-2008 ; period II), it in- creased more slowly from period II to the present period (2009-2012). However, the percentage of BLNAI strains, which had decreased from 10.6% (period I) to 8.9% (period II), began to increase during the present period. Tosufloxacin ("0.06μg!mL) and tazobactam!piperacillin ("0.13μg!mL) exhibited a low 90% mini- mum inhibitory concentration forH. influenzae, as well as for BLNAR strains. A decreased susceptibility to cephems was also observed throughout all 3 periods.
Serotype b strains (Hib) were observed in 54 of the 1,208 isolates (4.5%) ; their distribution decreased since period II (6.3%). In Hib, the percentage distribution of strains from patients less than 2 years of age, who are recommended to be vaccinated against Hib, decreased from 56.8% to 29.6%, and this reduction seems to have been achieved by increasing the percentage of Hib vaccine inoculations in Japan. Non- serotype b-capsulated strains were identified in 21 isolates (1.7%), and 11 of them were serotyped as type e, whereas the other 10 were serotyped as type f.