●症 例
要旨:症例は 51 歳,男性.2009 年 10 月および 2010 年 3 月の検診で胸部異常影を指摘されたため前医受 診となった.胸部 CT にて右中葉に腫瘤影を認め,FDG-PET でも同部位に異常集積を認めたことから肺癌 が疑われたが,CT ガイド下肺生検で診断確定に至らず,当科紹介となった.胸部 CT では右中葉 S4に spicu- lation や pleural indentation を伴う腫瘤影を認め,肺癌が強く疑われたが,各種検査でも確定診断がつかな かったことから,手術を施行した.摘出肺には細気管支を中心に類上皮細胞を伴った壊死性肉芽腫性病変が みられ,真菌や抗酸菌は証明されず,組織学的には気管支中心性肉芽腫症(Bronchocentric granulomatosis:
BCG)の範疇に入るものと考えられた.
キーワード:気管支中心性肉芽腫症,肺癌,外科的切除
Bronchocentric granulomatosis,Lung cancer,Surgical resection
緒 言
気管支中心性肉芽腫症(Bronchocentric granulomato- sis:以下 BCG)は 1973 年に Liebow1)によって提唱され た病理組織学的な概念で,気管支あるいは細気管支を中 心に壊死性肉芽腫を形成する病変と定義されている.
BCG は稀な疾患で,画像所見から肺癌との鑑別が問題 となることもあり,外科的切除によって診断されること も多い.今回我々は,画像所見からは肺癌が疑われ,外 科的切除後に気管支中心性肉芽腫症と診断し得た 1 例を 経験したので,文献的考察を加えて報告する.
症 例
症例:51 歳,男性.
主訴:胸部異常陰影.
既往歴:42 歳時に職場事故で右第 III,IV 指切断.気 管支喘息の既往なし.
家族歴:父,胃癌.
職業歴:粉塵曝露歴なし.
喫煙歴:30 本!日×33 年間(18 歳〜50 歳).
現病歴:2009 年 10 月の検診で胸部異常影を指摘され
るも放置.2010 年 3 月の検診で再度胸部異常影を指摘 され前医を受診した.胸部 CT にて右中葉に腫瘤影を,
FDG-PET でも同部位に異常集積を認めたため,肺癌疑 いにて CT ガイド下肺生検を施行されるも類上皮細胞性 肉芽腫を認めるのみで悪性所見はなく,精査目的に 5 月 当科紹介となった.
初診時現 症:身 長 176 cm,体 重 64 kg,血 圧 130!66 mmHg,脈拍 70!分・整,体温 36.5℃,SpO2 96%(room air).貧血・黄疸なし.表在リンパ節の腫脹を認めず.
心音・呼吸音異常なし.腹部異常なし.右第 III,IV 指 欠損.バチ状指なし.皮疹なし.
検査所見:血液検査では血算,生化学検査にて異常を 認めず,各種腫瘍マーカーも正常範囲内であった.また,
血清
β-D-glucan 値,アスペルギルス抗原および沈降抗
体,MPO-ANCA,PR3-ANCA,ツベルクリン反応,ク オンティフェロンは全て陰性であり,血清 ACE 活性値 も正常基準範囲内(8.8 IU!l,正常 値 8.3〜21.4 IU! l),
喀痰検査でも病原菌は検出されず,細胞診も陰性であっ た.
画像所見:胸部単純 X 線写真では,右中肺野に辺縁 不整な腫瘤影を認めた(Fig. 1).胸部 CT では,右中葉 S4末梢に葉間を越えて上下葉に進展する 35 mm 大の腫 瘤影を認めた.腫瘤の辺縁は不整で,spiculation や pleu- ral indentation を伴い内部は不均一に造影された(Fig.
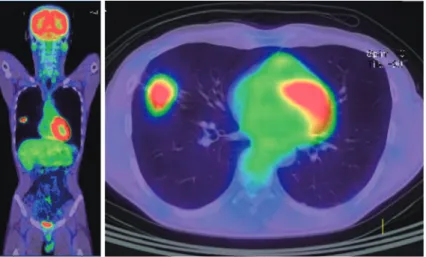
2).ま た 前 医 PET-CT で は 右 中 葉 腫 瘤 影 に 一 致 し て FDG 異常集積(SUV max:早期相 6.63,後期相 8.87)を 認め,その他には異常集積を認めなかった(Fig. 3).
臨床経過:前医での CT ガイド下肺生検の病理組織所
画像的に肺癌が疑われた気管支中心性肉芽腫症の 1 例
三村 一行
1)望月 吉郎
1)中原 保治
1)河村 哲治
1)三村 六郎
2)小橋陽一郎
3)〒670―8520 兵庫県姫路市本町 68
1)独立行政法人国立病院機構姫路医療センター呼吸器内
科
2)独立行政法人国立病院機構姫路医療センター病理
〒632―8552 奈良県天理市三島町 200
3)天理よろづ相談所病院病理
(受付日平成 23 年 5 月 18 日)
Fig. 1 Chest radiograph showing a nodular lesion with an irregular margin located in the right middle field.
Fig. 2 Chest CT scan showing a 35-mm nodular lesion at the periphery of the right S4 extending to the upper and lower lobes with an irregular margin, spiculation and pleural indentation. The inside of the nodular lesion was heterogeneously enhanced.
見では,肺内に壊死を伴わない小さな類上皮細胞肉芽腫 が散在しており,ラングハンス型巨細胞も認められた
(Fig. 4).よって,サルコイドーシス,抗酸菌や真菌感 染症,Wegener 肉芽腫症などの可能性を考え,各種検 査を施行するも有意な所見なく,頭部 MRI や骨シンチ,
眼科・耳鼻咽喉科的検査でも特記すべき異常所見を認め なかった.しかし,画像所見上は肺癌が強く疑われたた め,十分な説明を行い同意を得た上で外科的切除を行っ た.術中所見は,中葉は上葉とは末梢側で軽度癒着し,
下葉とは広範囲に癒着していた.術中迅速病理診断では 悪性所見なく,壊死を伴った類上皮細胞肉芽腫の所見の み認めたため,胸腔鏡下右中葉切除および上下葉部分切 除術で手術終了となった.
病理組織所見:切除腫瘤は 4.5×3.0×2.0 cm 大で,多 数の壊死性肉芽腫が葉間胸膜を越えて上中下葉に分布し ていた(Fig. 5).壊死物質は細気管支内腔に充満してお り,弾性線維染色でみると壊死性肉芽腫は肺動脈周囲に 形成されていた(Fig. 6A,B).また,壊死性肉芽腫の 周囲には巨細胞を伴った壊死のない肉芽腫形成もあり,
前医での CT ガイド下肺生検の組織像と一致していた
(Fig. 6C,D).よって,本症例は組織学的には細気管支
Fig. 3 A PET-CT scan shows an abnormal amount of FDG accumulation in the nodular lesion (SUV max; 6.63 in the early phase, 8.87 in the late phase).
Fig. 4 The CT-guided lung biopsy specimen obtained by the referring physician histopathologically showed that small non-necrotic epithelioid cell gran- ulomas were dispersed in the lung tissue and were associated with Langhan giant cells. (hematoxylin-eo- sin [HE] stain, ×10)
Fig. 5 Histology of the resected nodular lesion shows epithelioid cell granulomas with necrosis spreading beyond the interlobar pleura. (RUL: right upper lobe, RML: right middle lobe, PL: pleura, HE stain ×1)
を中心とした壊死性肉芽腫性病変,いわゆる broncho- centric granulomatosis(BCG)の範疇に入るものと考 え ら れ た.Ziehl-Neelsen 染 色,PAS 染 色,Grocott 染 色を行ったが抗酸菌や真菌は認めず,組織培養でも細菌 は検出されなかった.術後経過は良好であり,現在は外 来で経過観察中であるが,新たな陰影の出現は認めてお らず,気管支喘息の発症もない.
考 察
Liebow1)は 1973 年に肺における血管炎および肉芽腫 症を,classical Wegenerʼs granulomatosis(CWG),lim-
ited angitis and granulomatosis of the Wegener type
(LWG),lymphomatoid granulomatosis(LYG),necrotiz- ing sarcoid angitis(NSG),bronchocentric granulomato- sis(BCG)に分類したが,このうち BCG に関しては病 理組織学的概念が先行し,頻度も少なく,その病態がア レルギー反応なのか,感染症の一側面なのか,低悪性度 の腫瘍性病変なのか不明であり,臨床医にとって理解し 難い疾患概念となっている.Liebow によれば,BCG は 壁破壊を伴う気管支や細気管支周囲の非特異的な壊死性 肉芽腫性病変を特徴とするが,血管炎所見が軽いことが Wegener 肉芽腫などといった他の肉芽腫性血管炎と異 なるとされる.その後の検討で,BCG の約半数はアレ ルギー性気管支肺アスペルギルス症(allergic bron- chopulmonary aspergillosis:以下 ABPA)に伴うこと がわかってきた2).一方,ABPA を伴わない群では,
Fig. 6 (A) Epithelioid cell granuloma with necrosis centered on the bronchioles. (Br: bronchiole, PA: pul- monary artery, HE stain ×2) (B) This necrotizing granuloma was formed around the pulmonary artery (Elastica van Gieson stain ×2). (C) (D) These granulomas ( → ) were surrounded by other non-necrotic granulomas with giant cells. (HE stain ×10)
Wegener 肉芽腫症や関節リウマチ,抗酸菌感染症やク リプトコッカス症などアスペルギルス以外の真菌感染 症,インフルエンザ A,エキノコックス症,肺癌,糸 球体腎炎,中枢性尿崩症,ブドウ膜炎など様々な基礎疾 患に合併するという文献的報告がある3)〜12).従って,BCG という組織所見を認めた場合には,まず ABPA や真菌・
抗酸菌感染症などの基礎疾患の有無を検討すべきであ り,基礎疾患を指摘し得ない場合にのみ診断名として BCG とつけるのが好ましいと思われる.本症例では気 管支喘息や ABPA の所見は認めず,β-D-glucan,アス ペルギルス抗原・抗体,リウマチ因子,ANCA などは 全て陰性であり,眼科や耳鼻咽喉科診察でも Wegener 肉芽腫症などを示唆する所見も認めなかった.また,
Ziehl-Neelsen 染 色,PAS 染 色,Grocott 染 色 で も 病 巣 部に抗酸菌や真菌を認めず,組織培養でも原因菌は検出 できなかった.さらに,切除標本には Wegener 肉芽腫 症に典型的な好中球の壊死を特徴とする basophilic ne- crosis や ABPA によく認められるような好酸球浸潤な どもなく,本症例は基礎疾患を伴わないケースと考えら れた.
BCG の胸部単純 X 線写真や胸部 CT 所見は,spicula- tion を伴う単発性結節影や腫瘤影,mucoid impaction
や無気肺を伴う浸潤影などが片側性,上葉優位にみられ るとされている13)14).本症例では,胸部 CT にて spicula- tion や pleural indentation を伴い,葉間を越える陰影を 認め,また前医 PET-CT で FDG 異常集積を認めたこと より,肺野型肺癌を強く疑った.BCG 症例の中には肺 癌と類似の画像所見を呈するものや,増大傾向を示すも のもあり15),本症例においてもあたかも肺癌のように葉 間を越えて上葉および下葉にも病変が広がっていた.本 症例の手術所見では分葉不全は認めず,病理学的に肺癌 の併存などもなかったことから,BCG 自体が浸潤傾向 の強い一面を持っている可能性が考えられた.また BCG には本症例と同様に FDG-PET で集積を認める症例も報 告されている16).本症例の FDG 集積は後期相でさらに 亢進しており,これは一般的には悪性腫瘍を強く疑う所 見である.よって,BCG と肺癌の鑑別は FDG-PET で も困難であると考えられる.
本症例では画像的に肺癌が強く疑われ経皮生検で BCG に矛盾しない所見が得られていたが,陰影のすべ てが BCG でよいのか,腫瘍性病変が併存していないか,
といった疑問が生じ結局外科的切除が避けられなかっ た.治療に関しては,基礎疾患がある症例ではその治療 が基本であるが,限局性 BCG 病変では,外科的切除の
みで多くが治癒すると言われており,本症例も術後再発 は認めず経過良好である.
以上,画像的に肺癌との鑑別に苦慮した BCG の 1 例 を経験したので文献的考察を加えて報告した.
引用文献
1)Liebow AA. Pulmonary angiitis and granulomatosis.
Am Rev Respir Dis 1973 ; 108 : 1-18.
2)Katzenstein AL, Liebow AA, Friedman PJ. Bron- chocentric granulomatosis, mucoid impaction, and hypersensitivity reactions to fungi. Am Rev Respir Dis 1975 ; 111 : 497-537.
3)Yousem SA. Bronchocentric injury in Wegenerʼs granulomatosis : a report of five cases. Hum Pathol 1991 ; 22 : 535-540.
4)Bonafede RP, Benatar SR. Bronchocentric granulo- matosis and rheumatoid arthritis. Br J Dis Chest
1987 ; 81 : 197-201.
5)Myers JL, Katzenstein AL. Granulomatous infection mimicking bronchocentric granulomatosis. Am J Surg Pathol 1986 ; 10 : 317-322.
6)Myers JL. Bronchocentric granulomatosis. Disease or diagnosis? Chest 1989 ; 96 : 3-4.
7)Van der Klooster JM, Nurmohamed LA, van Kaam NA. Bronchocentric granulomatosis associated with influenza-A virus infection. Respiration 2004 ; 71 : 412-416.
8)Den Hertog RW, Wagenaar SS, Wastermann CJ.
Bronchocentric granulomatosis and pulmonary
echinococcosis. Am Rev Respir Dis 1982 ; 126 : 344- 347.
9)Houser SL, Mark EJ. Bronchocentric granulomato- sis with mucus impaction due to bronchogenic carci- noma. An association with clinical relevance. Arch Pathol Lab Med 2000 ; 124 : 1168-1171.
10)Warren J, Pitchenik AE, Saldana MJ. Bronchocen- tric granulomatosis with glomerulonephritis. Chest 1985 ; 87 : 832-834.
11)Rossi GP, Pavan E, Chiesura-Corona M, et al. Bron- chocentric granulomatosis and central diabetes in- sipidus successfully treated with corticosteroids.
Eur Respir J 1994 ; 7 : 1893-1898.
12)田中雅子,市川洋一郎,木下正治,他.ブドウ膜炎 を合併した Bronchocentric granulomatosis の 1 例.
日胸疾会誌 1992 ; 30 : 1537-1542.
13)Robinson RG, Wehunt WD, Tsou E, et al. Broncho- centric granulomatosis : roentgenographic manifes- tations. Am Rev Respir Dis 1982 ; 125 : 751-756.
14)Ward S, Heyneman LE, Flint JDA, et al. Broncho- centric granulomatosis : computed tomographic findings in five patients. Clin Radiol 2000 ; 55 : 296- 300.
15)桑原元尚,宗像光輝,光武孝倫,他.腫瘤影を呈し た気管支中心性肉芽腫症の 1 例.日胸 2008 ; 67 : 678-683.
16)Hurwitz LM, McAdams HP, Sporn TA, et al. A 73- year-old woman with a cough. Chest 2005 ; 128 : 1018.
Abstract
A case of bronchocentric granulomatosis resembling lung cancer on diagnostic imaging
Kazuyuki Mimura
1), Yoshirou Mochizuki
1), Yasuharu Nakahara
1), Tetsuji Kawamura
1), Rokurou Mimura
2)and Youichirou Kobashi
3)1)Department of Respiratory Medicine, National Hospital Organization Himeji Medical Center
2)Department of Pathology, National Hospital Organization Himeji Medical Center
3)Department of Pathology, Tenri Yorozu Hospital
A 51-year-old man visited a local physician because of a chest radiographic abnormality which had been pointed out in October 2009 and March 2010. His chest CT images revealed a nodular lesion in the right middle lobe. Since the nodular lesion showed abnormal FDG accumulation on FDG-PET, the physician suspected lung cancer, but was unable to make a definitive diagnosis by CT-guided lung biopsy. The patient was thus referred to our hospital for detailed investigations. A nodular lesion with spiculation and pleural indentation was recognized in the S4region on chest CT scans which was strongly suspected to be lung cancer. Since various examinations did not provide a definitive diagnosis, we performed surgery. The histological findings of the extirpated tumor were considered to be bronchocentric granulomatosis (BCG), because necrotic granulomatous lesions with epithe- lioid cells centered on the bronchioles and there was no evidence of fungus or acid-fast bacterium infection.