被保険者
被扶養者
㊞ 私は ㊞ を代理人と定め、療養費(家族療養費)の受領を ㊞¥
受 付 日 付 印 年 月 日 平・令 年 月 日まで 平・令 年 月 日 □は い ⇒ □仕事中(業務上・通勤途上) □第三者行為(交通事故等) □いいえ海外療養費支給申請書
健康保険被保険者 記号 被保険者の㊞
証の記号と番号 番号 氏名と印 被 保 険 者 の 住 所〒
丁目、番地、アパート名等詳細に記入してください。 電 話 番 号 - -事 業 所 の 名 称 発病又は負傷の原因 傷 病 の 経 過 年 月 日 受診した医療機関名 住所及び担当医師名 名称 住所 担当名 診療又は手当の内容 平成 令和 傷 病 名 発病又は負傷の 年 月 日 診療又は手当の期間 う ち 入 院し た 期 間 平・令 年 月 日から 日間 申請が被扶養者分であ るときはその者の氏名 生年 月日 昭和 平成 令和 年 月 日 平・令 仕事中又は第三者行為 による傷病ですか? 同意欄 療養を受けた海外の医療機関等に中部アイティ産業健康保険組合が文書等により当申請内容を 照会することに同意します。 (被保険者氏名) マイナンバーにより申請する場合は、備考欄に記載して下さい。当健保にマイナンバーの届出がない方は、マイナンバーカード(両面写)を 添付して下さい。なお、マイナンバーカードをお持ちでない方は、通知カード(写)またはマイナンバー付きの住民票と運転免許証等の顔写 真付きの身分証明(写)を添付して下さい。 被保険者 との続柄 □マイナンバー記載の本申請書提出を事業主へ委任します。(事業主経由にて申請の場合、レ点) 備 考 受取代理人の欄 委任します。 (被保険者氏名) 支 給 金 額 被保険者 銀行口座 銀行 金庫 農協 本店 支店 出張所 健 保 組 合 処 支 給 決 定 確 認年 月 日
取 得 喪 失 常 務 理 事 事 務 長 係 ( 支給額計算 款 項 目年 月 日
) 年 月 日 支 払 年 月 日 ( 名義 ) 普通 口座番号1 Please fill in this form so that the patient may claim the social insurance benefit.
この様式は患者の社会保険の給付の申請に必要ですので、証明をお願いします。2 This form should be completed and signed by the attending physician.
この様式は担当医が記入し、署名して下さい。3 One form for each month and one form for hospitalization/outpatient (home visit) should be filled out.
各月毎、入院・入院外毎につき、この様式1枚が必要です。Form A
様 式 A
1 Name of Patient (Last, First)
患 者 名
Age(Date of Birth)
Sex ( Male / Female )
年齢(生年月日) 性別 ( 男 ・ 女 )
2 Name of Illness or Injury preferablry with the number of International Classiffication of Diseases for
the use of Social Insurance (Please refer to the table attached to this form).
傷病名及び社会保険用国際疾病分類番号
3 Date of First Diagnosis :
初 診 日 ,
4 Days of Diagnosis and Treatment :
days
診 療 日 数 日間
5 Type of Treatment
治療の分類
□ Hospitalization : From
to
( ) days
入院 自 至 ( ) 日間
□ Outpatient or
Home Visit
入院外
6 Nature and Condition of Illness or Injury (in brief)
症 状 の 概 要
7 Prescription, Operation and any other Treatments (in brief)
処方、手術その他の処置の概要
8 Was the treatment as a result of an accidential injury?
Yes
□
No
□
治療は事故の傷害によるものですか? はい いいえ
9 Itemized amounts paid to Hospital and / or Attending Physician : Fill in Form B
項目別治療実費 / 様式Bによる
10 Name and Address of Attending Physician
担当医の名前及び住所
Name 名前 :
Last 姓
First 名
Title 称号
Address 住所:
Home
自宅Phone
電話Office
病院又は診療所Phone
電話Date
日付Signature
署名Attending Physician 担当医
Reference Number of your Medical Record (if applicable)
診療録の番号
(No. )
Attending Physician's Statement
診 療 内 容 明 細 書
Request to Attending Physician
邦 訳 (A)
2.傷病名及び社会保険用国際疾病分類番号
6.症状の概要
7.処方、手術その他の処置の概要
1 Please fill in this form so that the patient may claim the social insurance benefit.
この様式は患者の社会保険の給付の申請に必要ですので、証明をお願いします。
2 This form should be completed and signed by either the attending physician or the superintendent of hospital/
この様式は担当医又は病院事務長が記入し、署名して下さい。
3 One form for each month and one form for hospitalization/outpatient (home visit) should be filled out.
各月毎、入院・入院外毎につき、この様式1枚が必要です。
4 If not in dollars, please specify the unit used.
ドル以外の貨幣の場合はその旨を書いて下さい。
Form B
様 式 B
Fee for Initial Office Visit
初 診 料$
Fee for Follow-up Office Visit
再 診 料$
Fee for Home Visit
往 診 料$
Fee for Hospital Visit
入院管理料$
Hospitalization
入 院 費$
Consultation
診 察 費$
Operation
手 術 費$
Professional Nursing
職業看護婦費$
X-Ray Examinations
X線検査費$
Laboratory Tests
諸検査費$
Medicines
医 薬 費$
Surgical Dressing
包 帯 費$
Anaethetics
麻 酔 費$
Operating Room Charge
手術室費用$
$
Others (Specify)
その他(項目明記)$
$
Unit is
Total
合
計
$
貨幣単位Important : Exclude the amount irrelevant to the treatment, i.e. , payment for a luxurious room charge
注 意 : 高級治療室等治療に直接関係のないものは除いて下さい。
Name 名前 :
Last 姓
First 名
Title 称号
Address 住所:
Home
自宅Phone
電話Office
病院又は診療所Phone
電話Date
日付Signature
署名Attending Physician 担当医
Reference Number of your Medical Record (if applicable)
診療録の番号
(1)
(2)
Request to Attending Physician or Superintendent of Hospital / Clinic
担当医又は病院事務長へのお願い
Itemized Receipt
診 療 内 容 明 細 書
担当医又は病院事務長の名前及び住所
(16)
(6)
(7)
(8)
(9)
(10)
(11)
(13)
(14)
Name and Address of Attending Physician / Superintendent of Hospital or Clinic
(12)
(3)
(4)
(15)
(5)
邦 訳 (B)
(15) その他(項目明記)
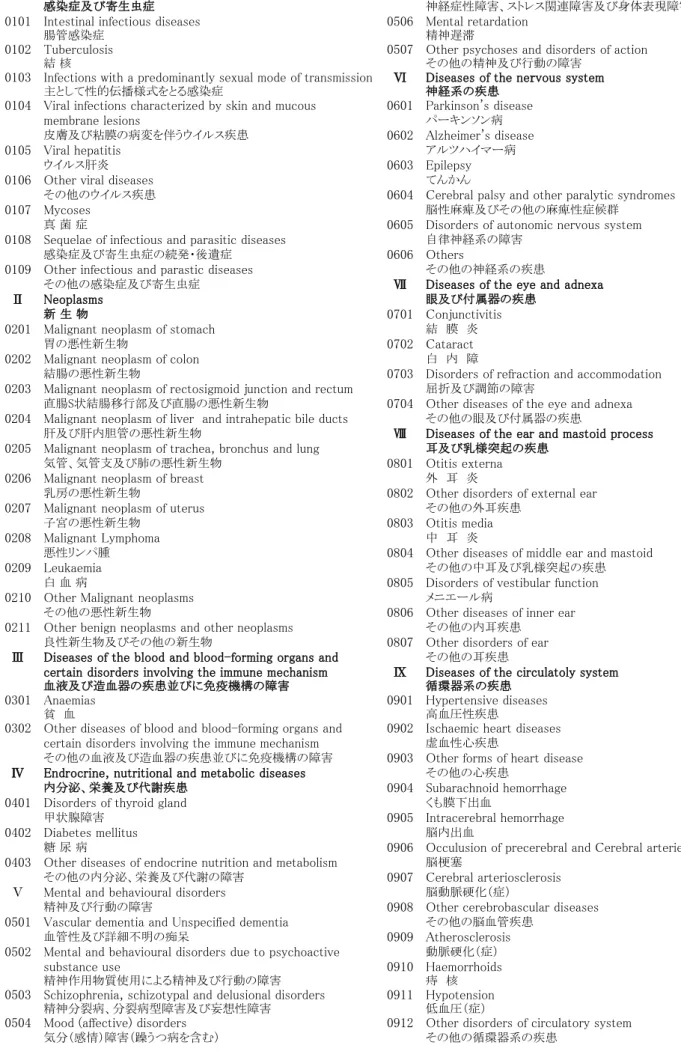
Ⅰ Certain infectious and parasitic diseases 0505 Neurotic, stress-related and somatoform disorders
感染症及び寄生虫症 神経症性障害、ストレス関連障害及び身体表現障害
0101 Intestinal infectious diseases 0506 Mental retardation
腸管感染症 精神遅滞
0102 Tuberculosis 0507 Other psychoses and disorders of action
結 核 その他の精神及び行動の障害
0103 Infections with a predominantly sexual mode of transmission Ⅵ Diseases of the nervous system
主として性的伝播様式をとる感染症 神経系の疾患
0104 Viral infections characterized by skin and mucous 0601 Parkinson's disease
membrane lesions パーキンソン病
皮膚及び粘膜の病変を伴うウイルス疾患 0602 Alzheimer's disease
0105 Viral hepatitis アルツハイマー病
ウイルス肝炎 0603 Epilepsy
0106 Other viral diseases てんかん
その他のウイルス疾患 0604 Cerebral palsy and other paralytic syndromes
0107 Mycoses 脳性麻痺及びその他の麻痺性症候群
真 菌 症 0605 Disorders of autonomic nervous system 0108 Sequelae of infectious and parasitic diseases 自律神経系の障害
感染症及び寄生虫症の続発・後遺症 0606 Others
0109 Other infectious and parastic diseases その他の神経系の疾患
その他の感染症及び寄生虫症 Ⅶ Diseases of the eye and adnexa
Ⅱ Neoplasms 眼及び付属器の疾患
新 生 物 0701 Conjunctivitis
0201 Malignant neoplasm of stomach 結 膜 炎
胃の悪性新生物 0702 Cataract
0202 Malignant neoplasm of colon 白 内 障
結腸の悪性新生物 0703 Disorders of refraction and accommodation 0203 Malignant neoplasm of rectosigmoid junction and rectum 屈折及び調節の障害
直腸S状結腸移行部及び直腸の悪性新生物 0704 Other diseases of the eye and adnexa 0204 Malignant neoplasm of liver and intrahepatic bile ducts その他の眼及び付属器の疾患
肝及び肝内胆管の悪性新生物 Ⅷ Diseases of the ear and mastoid process 0205 Malignant neoplasm of trachea, bronchus and lung 耳及び乳様突起の疾患
気管、気管支及び肺の悪性新生物 0801 Otitis externa 0206 Malignant neoplasm of breast 外 耳 炎
乳房の悪性新生物 0802 Other disorders of external ear 0207 Malignant neoplasm of uterus その他の外耳疾患
子宮の悪性新生物 0803 Otitis media
0208 Malignant Lymphoma 中 耳 炎
悪性リンパ腫 0804 Other diseases of middle ear and mastoid
0209 Leukaemia その他の中耳及び乳様突起の疾患
白 血 病 0805 Disorders of vestibular function 0210 Other Malignant neoplasms メニエール病
その他の悪性新生物 0806 Other diseases of inner ear 0211 Other benign neoplasms and other neoplasms その他の内耳疾患
良性新生物及びその他の新生物 0807 Other disorders of ear Ⅲ Diseases of the blood and blood-forming organs and その他の耳疾患
certain disorders involving the immune mechanism Ⅸ Diseases of the circulatoly system
血液及び造血器の疾患並びに免疫機構の障害 循環器系の疾患
0301 Anaemias 0901 Hypertensive diseases
貧 血 高血圧性疾患
0302 Other diseases of blood and blood-forming organs and 0902 Ischaemic heart diseases certain disorders involving the immune mechanism 虚血性心疾患
その他の血液及び造血器の疾患並びに免疫機構の障害 0903 Other forms of heart disease Ⅳ Endrocrine, nutritional and metabolic diseases その他の心疾患
内分泌、栄養及び代謝疾患 0904 Subarachnoid hemorrhage 0401 Disorders of thyroid gland くも膜下出血
甲状腺障害 0905 Intracerebral hemorrhage
0402 Diabetes mellitus 脳内出血
糖 尿 病 0906 Occulusion of precerebral and Cerebral arteries 0403 Other diseases of endocrine nutrition and metabolism 脳梗塞
その他の内分泌、栄養及び代謝の障害 0907 Cerebral arteriosclerosis Ⅴ Mental and behavioural disorders 脳動脈硬化(症)
精神及び行動の障害 0908 Other cerebrobascular diseases 0501 Vascular dementia and Unspecified dementia その他の脳血管疾患
血管性及び詳細不明の痴呆 0909 Atherosclerosis
0502 Mental and behavioural disorders due to psychoactive 動脈硬化(症)
substance use 0910 Haemorrhoids
精神作用物質使用による精神及び行動の障害 痔 核
0503 Schizophrenia, schizotypal and delusional disorders 0911 Hypotension
精神分裂病、分裂病型障害及び妄想性障害 低血圧(症)
0504 Mood (affective) disorders 0912 Other disorders of circulatory system
気分(感情)障害(躁うつ病を含む) その他の循環器系の疾患
社会保険用国際疾病分類表
Ⅹ Diseases of the respiratory system 1306 Low back pain and sciatica
呼吸器系の疾患 腰痛症及び坐骨神経痛
1001 Acute nasopharyngitis (common cold) 1307 Other dorsopathies
急性鼻咽頭炎(風邪) その他の脊椎障害
1002 Acute pharyngitis and tonsillitis 1308 Shoulder lesions
急性咽頭炎及び急性扁桃炎 肩の傷害
1003 Other acute upper respiratory infections 1309 Disorders of bone density and structure
その他の急性上気道感染症 骨の密度及び構造の障害
1004 Pneumonia 1310 Other diseases of skeletal muscles and connective tissues
肺 炎 その他の筋骨格系及び結合組織の疾患
1005 Acute bronchitis and bronchiolitis ⅩⅣ Diseases of the genitourinary system
急性気管支炎及び急性細気管支炎 尿路性器系の疾患
1006 Vasmotor and allergic rhinitis 1401 Glomerular diseases
アレルギー性鼻炎 糸球体疾患及び腎尿細管間質性疾患
1007 Chronic sinusitis 1402 Renal failure
慢性副鼻腔炎 腎 不 全
1008 Bronchitis, not specified as acute or chronic 1403 Urolithiasis
急性又は慢性と明示されない気管支炎 尿路結石症
1009 Chronic obstructive pulmonary disease 1404 Other diseases of urinary system
慢性閉塞性肺疾患 その他の尿路系の疾患
1010 Asthma 1405 Hyperplasia of prostate
喘 息 前立腺肥大(症)
1011 Other diseases of respiratory system 1406 Other diseases of male genital organs
その他の呼吸器系の疾患 その他の男性性器の疾患
ⅩⅠ Diseases of the digestive system 1407 Menopausal and postmenopausal disorders
消化器系の疾患 月経障害及び閉経周辺期障害
1101 Dental caries 1408 Other disorders of breast and female genital organs
う 蝕 乳房及びその他の女性性器の疾患
1102 Gingivitis and periodontal diseases ⅩⅤ Pregnancy, childbirth and the puerperium
歯肉炎及び歯周疾患 妊娠、分娩及び産じょく
1103 Other disorders of teeth and supporting structures 1501 Pregnancy with abortive outcome
その他の歯及び歯の支持組織の障害 流 産
1104 Gastric and duodenal ulcer 1502 Oedema, proteinuria and hypertensive disorders in pregnancy,
胃潰瘍及び十二指腸潰瘍 childbirth and the puerperium 1105 Gastritis and duodenitis 妊娠中毒症
胃炎及び十二指腸炎 1503 Single spontaneous delivery 1106 Alcoholic liver disease 単体自然分娩
アルコール性肝疾患 1504 Others
1107 Chronic hepatitis, not elsewhere classified その他の妊娠、分娩及び産じょく
慢性肝炎(アルコール性のものを除く) ⅩⅥ Certain conditions originating in the perinatal period
1108 Liver cirrhosis 周産期に発生した病態
肝硬変(アルコール性のものを除く) 1601 Disorders related to length of gestation and fetal growth 1109 Other disorders of liver 妊娠及び胎児発育に関連する障害
その他の肝疾患 1602 Others
1110 Cholelithiasis and cholecystitis その他の周産期に発生した病態
胆石症及び胆のう炎 ⅩⅦ Congeneital malformations, deformations and chromosomal 1111 Diseases of pancreas abnormalities
膵 疾 患 先天奇形、変形及び染色体異常
1112 Other diseases of digestive system 1701 Congenital anomalies of heart
その他の消化器系の疾患 心臓の先天奇形
ⅩⅡ Diseases of the skin and subcutaneous tissue 1702 Others
皮膚及び皮下組織の疾患 その他の先天奇形、変形及び染色体異常
1201 Infections of the skin and subcutaneous tissue ⅩⅧ Symptoms, signs and abnormal clinical and laboratory findings,
皮膚及び皮下組織の感染症 not slewhere classified
1202 Dermatitis and eczema 症状、徴候及び異常臨床所見・異常検査所見で他に分類されないもの 皮膚炎及び湿疹 1800 Symptoms, signs and abnormal clinical and labolatory findings, 1203 Others not slewhere classified
その他の皮膚及び皮下組織の疾患 症状、徴候及び異常臨床所見・異常検査所見で他に分類されないもの
ⅩⅢ Diseases of the musculoskeletal system and ⅩⅨ Injury, poisoning and certain other concequences of connective tissue external causes
筋骨格及び結合組織の疾患 損傷、中毒及びその他の外因の影響
1301 Inflammatory polyarthropathies 1901 Fracture
炎症性多発性関節障害 骨 折
1302 Arthrosis 1902 Intracranial damege and internal organ damege
関 節 症 頭蓋内損傷及び内臓の損傷
1303 Spondylopathies 1903 Burns and corrosions
脊椎障害(脊椎症を含む) 熱傷及び腐食
1304 Interverteblal disc disorders 1904 Poisoning *