緒 言 近年、小児科・小児外科、消化器外科および救命救急 医学の領域において、プロバイオティクスの代表的な菌 株であるL . caseiシロタ株(LcS 株)およびB . breveヤ クルト株(BBG-01 株)を用いたプロ(シン)バイオティ クス療法による感染症予防に関する報告が増加している 1-5)。臨床機関における、シンバイオティクス療法によ る感染症予防のアプローチは増々、発展していくものと 考えられる。 一方で、臨床で用いられている抗菌薬に対する LcS 株および BBG-01 株の感受性について、医療機関から の問い合わせが増加している。そこで LcS 株および BBG-01 株の種々の抗菌薬に対する最小発育阻止濃度 (MIC)を Clinical and Laboratory Standards Institute (CLSI:米国臨床検査標準化委員会)の定める broth microdilution method6)にて測定し、それぞれの感受性 を判定した。 材料および方法 1.抗菌薬の調製 各種抗菌薬 47 種 { アミノグリコシド系[Amikacin sulfate salt(Sigma),Gentamycin salfate(Sigma), Kanamycin monosalfate(Sigma),Streptomycin sulfate salt(Sigma)]、ϐ−ラクタム系[Ampicillin(Sigma), Carbenicillin disodium salt(Sigma),Oxacillin sodium salt monohydrate(Sigma),Penicillin(Sigma)]、セフェ ム系[Cefaclor(Sigma),Cefazolin sodium salt(Sigma), Cefbuperazone sodium(Toyama Chemical),Cefdinir (Sigma),Cefmetazole sodium(Daiichi Sankyo),
Cefotaxime(Sigma),Cefotiam dihydrochloride (Takeda Pharmaceutical),Cefoxitin sodium salt (Sigma),Cefpirome sulfate(Aventis Pharma),
Cefsulodin sodium salt(Sigma),Ceftazidime hydrate (Sigma),Ceftizoxime sodium(Fujisawa Healthcare),
Ceftriaxone disadium salt hemi(hepatohydrate) (Sigma),Cephalothin sodium salt(Sigma),Flomoxef
Lactobacillus casei
シロタ株および
Bifidobacterium breve
ヤクルト株の薬剤感受性
朝原 崇・結城 功勝・高橋 明・高橋 琢也・野本 康二
Takashi Asahara, Norikatsu Yuki, Akira Takahashi, Takuya Takahashi, Koji Nomoto Yakult Central Institute for Microbiological Research,
1796 Yaho, Kunitachi, Tokyo 186-8650 Japan
Abstract
The minimum inhibitory concentrations (MIC) of probiotic strains, Lactobacillus casei strain Shirota (LcS) and Bifidobacteriumbreve strain Yakult (BBG-01) to clinically used antibiotics were determined by the broth microdilution method proposed by the Clinical and Laboratory Standards Institute (CLSI) . Since the CLSI susceptibility evaluation table does not include Lactobacillus or Bifidobacterium, their susceptibility was evaluated using the evaluation tables for other bacteria . LcS and BBG-01 were slightly susceptible to many aminoglycoside, cephem, quinolone, peptide antibiotics, fosfomycin, sulfamethoxazole, trimethoprime, but were susceptible to tetracycline and macrolide antibiotics .
Susceptibility of
Lactobacillus casei
strain Shirota and
sodium(Shionogi),Latamoxef sodium(Shionogi)]、 マクロライド系[Clarithromycin(Sigma),Clindamycin (Sigma),Erythromycin(Sigma),Oleandomycin phosphate salt(Sigma)]、カルバペネム系[Imipenem/ Cilastatin(Banyu Pharmaceutical),Panipenem/ betamipron(Daiichi Sankyo)]、キノロン系[Ciprofloxacin (Sigma),Enoxacin(Sigma),Levofloxacin HCl(LKT
Laboratories),Lomefloxacin hydrochroride(Santa Cruz Biotechnology),Ofloxacin(Sigma)]、テトラサイクリン系 [Minocyclin hydrochloride(Sigma),Tetracyclin
hydrochloride(Sigma)]、ペプチド系[Colistin methanesulfate (Sigma),Polymyxin B sulfate salt(Sigma),Vancomycin
hydrochloride(Sigma)]、および、その他[Chloramphenicol (Sigma),Fosfomycin disodium salt(Sigma),
Lincomycin(Sigma),Neomycin sulfate(Sigma), Sulfamethoxazole(Sigma),Trimethoprim lactate salt (Sigma)]}をそれぞれ 25 .6 mg/0 .5 ml になるよう滅菌蒸 留水に溶解し、これを 0 .45 µm のメンブランフィルター (DISMIC-25cs,Toyo Roshi)を用いてろ過滅菌した。ろ 過滅菌済みの各種抗菌薬水溶液を基礎培地(LSM- シス テイン添加液体培地7))に添加して、512 µg/ml の各抗 菌薬添加液体培地を作製した。さらに 512 µg/ml の各 抗菌薬添加液体培地を基礎培地にて 2 倍段階希釈して、 256 ~ 0 .5 µg/ml の希釈系列を作製した。512 ~ 0 .5 µg/ml の濃度の各抗菌薬添加液体培地を 96 穴プレート (丸底、滅菌済)のウェルに 50 µl ずつ分注した。陰性 対照として抗菌薬非添加液体培地を用いた。 2.菌液の調製 LcS 株を 104 CFU/ml になるよう 10 ml の MRS 液体
培地(Becton Dickinson and Company[3])に添加し
て、37℃、24 時間嫌気(100%CO2
)培養した。BBG-01 株 に つ い て は、104 CFU/ml に な る よ う 10 ml の
GAM 液 体 培 地(Nissui Pharmaceutical8))に 菌 を 添
加して同様に培養した。培養終了後の各培養液の 0 .1 ml を、 そ れ ぞ れ MRS 寒 天 培 地(Becton Dickinson and Company、LcS 株用)、あるいは GAM 寒天培地 (Nissui Pharmaceutical、BBG-01 株用)に塗抹して、
37℃、48 時間嫌気(Anaero Pack-Anaero, Mitsubishi Gas Chemical)培養した。培地上に発育したコロニー 10 ~ 20 個を釣菌して、これをそれぞれの液体培地に 懸濁(マクファーランド 0 .5-1 .0)させて、106 CFU/ml になるよう調整した。調整済み菌液を 96 穴プレートに 50 µl ずつ分注した(抗菌薬最終濃度:0 .25 ~ 256 µg/ ml)。 3.培養および MIC 判定 菌液入りの 96 穴プレートの蓋をして良く撹拌した後、 37℃、48 時間嫌気(Anaero Pack-Anaero 薬剤感受性 用 , Mitsubishi Gas Chemical)培養した。培養後、Well 中の培養液の発育を観察して、陰性対照に比べて目視に て明確に増殖抑制の認められた各種抗菌薬の最低濃度を 最小発育阻止濃度(MIC)とした。なお本測定を 3 連に て実施した。感染リスクのある細菌についての薬剤感受 性評価基準である CLSI M100-S189)を参考にして感受 性(S)、中間(I)、低感受性(R)を判定した。なお、CLSI M100-S18 に は、Bifidobacteriumお よ びLactobacillus の感受性判定表がないことから、単純比較はできないが、 本 論 文 で は 便 宜 上、Staphylococcus、Enterococcus、
Enterobacteriaceae、あるいは Non-Enterobacteriaceae
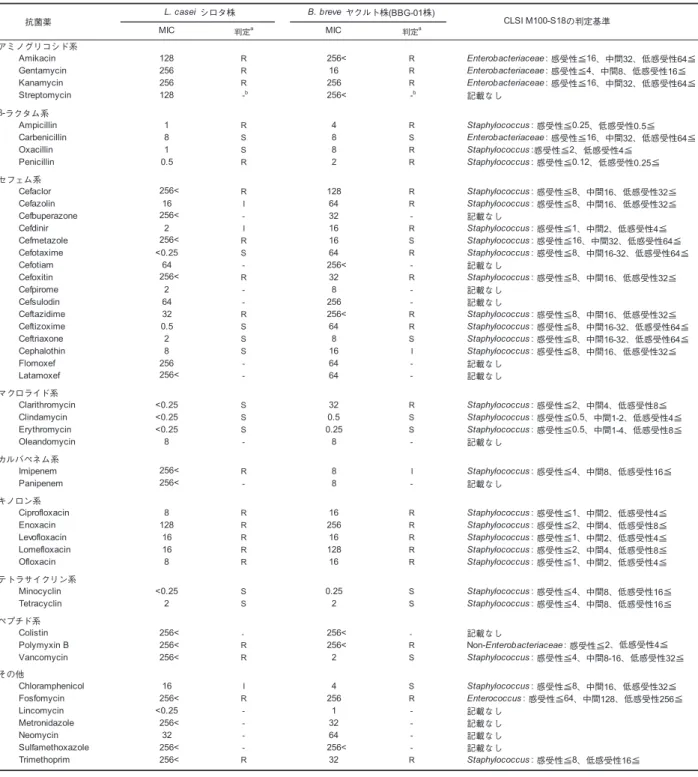
の判定基準を用いて、それぞれの感受性を判定した。 結 果 47 種の抗菌薬に対する LcS 株および BBG-01 株の MIC を Table 1 に示した。 1)LcS 株は、アミノグリコシド系、キノロン系およびペプ チド系の多くの抗菌薬、ならびにβ - ラクタム系の Ampicillin および Penicillin、セフェム系の Cefaclor、 Cefmetazole、Cefoxitin および Ceftazidime、カルバペ ネム系のImipenem、Fosfomycin および Trimethoprim に低感受性であった。CLSI M100-S18 の感受性判定表 に掲載されていない Metronidazole、Neomycin およ び Sulfamethoxazole に対する MIC が高値であり(32 ~ 256< µg/ml)、これらの抗菌薬に対しても低感受性 であると考えられた。一方、セフェム系の Cefotaxime、 Ceftizoxime、Ceftriaxone および Cefalothin、マクロ ライド系の多くの抗菌薬およびテトラサイクリン系の Minocyclin および Tetracyclin に は 感 受 性 で あり、 Chloramphenicol には中間であった。 2)BBG-01 株は、アミノグリコシド系、ϐ ラクタム系、セ フェム系、およびキノロン系の多くの抗菌薬、ならび
にマクロライド系の Clarithromycin、ペプチド系の Polymyxin B や Fosfomycin および Trimethoprim に 低感受性であった。また、CLSI M100-S18 の感受性判 定表に記載されていない Metronidazole、Neomycin および Sulfamethoxazole に対する MIC が高値であ り(32 ~ 256< µg/ml)、これらの抗菌薬に対しても 低感受性であると考えられた。一方、カルバペネム系 の Imipenem には中間値を示し、マクロライド系の Clindamycin および Erythromycin、ならびにテトラ サイクリン系の Minocyclin および Tetracyclin、ペプ チド系の Vancomycin、および Chloramphenicol に は感受性であった。 考 察 周術期の患者では、感染症の予防、治療を目的として 抗菌薬が使用されることが多い。したがって抗菌薬投与 下の患者に用いられるプロバイオティクスの生菌として の有効性を考慮すると、その抗菌薬に対して低感受性で あることが必要である。 一方、臨床で用いられる抗菌薬に対するLactobacillus やBifidobacteriumの 感 受 性 に つ い て、 種 々 の 乳 酸 菌やビフィズス菌で報告8,10)が認められるが、残念な がらこれまで LcS 株については臨床で使用される頻 度の低い抗菌薬についての報告のみであり11)、また BBG-01 株については薬剤感受性の報告は認められな い。周術期の感染症予防のため、術前に Kanamycin や Metronidazole が、術後に Cefazorin や Cefotiam 等の セフェム系の抗菌薬、Vancomycin、等が使用されるこ とが多い12,13)。今回の MIC 測定結果より、LcS 株およ び BBG-01 株は、臨床で用いられるアミノグリコシド 系、セフェム系、キノロン系、ペプチド系の多くの抗菌 薬、ならびに Fosfomycin や Metronidazole に低感受 性であることが明らかになった。また LcS 株について はカルバペネム系抗菌薬や Vancomycin にも低感受性 であった。以上のことから患者における当該抗菌薬と LcS 株および BBG-01 株の併用による予防・治療効果 の可能性が強く示唆された。 病原菌による抗菌薬耐性獲得についての問題が提起 され、伝達性の抗菌薬耐性遺伝子の有無はプロバイオ ティクにおいても安全性評価の主要な基準の一つと なっている11,14)。院内感染菌である Vancomycin 耐
性腸球菌(VRE)の Vancomycin 耐性遺伝子(vanA と vanB 遺伝子)は薬剤耐性プラスミドなどにより接合伝 達で菌体間を伝播する。LcS 株も Vancomycin に対し て低感受性であったが、木脇ら11)は、LcS 株が既知の Vancomycin 耐性遺伝子を持たないことを PCR 法に より明らかにしている。近年、メチシリン耐性黄色ブ ドウ球菌(MRSA)、多剤耐性アシネトバクタバウマニ (MDRAb)、VRE、等の耐性菌の出現が社会問題となっ ていることから、臨床で用いられるプロバイオティクス は、耐性遺伝子伝播についての安全性が調べられた菌株 でなければならないと考えられた。 木脇らは、17 種の抗菌薬に対する LcS 株を含むL . casei 43 菌株およびB . breve 26 菌株の薬剤感受性を 測定したところ、供した菌株は概ね菌種固有の MIC 値 を示したと報告している11,15)。本研究で用いた臨床で 利用される抗菌薬に対しても、供試菌株を増やして、菌 種固有の自然耐性か獲得耐性かの判断16)、既知の抗生 物質耐性遺伝子の有無の確認等により、伝達性抗生物質 耐性遺伝子を持つか否かを明らかにしていくことが今後 の課題であると考えられた。 要 約 臨床で用いられている抗菌薬に対する プロバイオティ クスの代表的な菌株であるLactobacillus caseiシロタ株 (LcS株)およびBifidobacterium breve ヤクルト株(BBG-01 株)の最小発育阻止濃度(MIC)について、Clinical and Laboratory Standards Institute(CLSI)の 定 め る broth microdilution method にて測定した。CLSI の感 受性判定表には、BifidobacteriumおよびLactobacillus の判定表がないことから、他の細菌の判定表を参照して、 それぞれの感受性を判定した。 LcS 株および BBG-01 株は、臨床で用いられるアミノグ リコシド系、セフェム系、キノロン系およびペプチド系の多 くの抗菌薬、ならびに Fosfomycin、Sulfamethoxazole お よび Trimethoprime に低感受性であり、テトラサイクリン 系やマクロライド系の抗菌薬には感受性であった。
【参考文献】 Genes in the probiotic L . casei strain Shirota . Annual Report of Yakult Central Institute for Microbiological Research ., 29, 27-36(2010) .
12) Kusachi S, Sumiyama Y, Nagao J, Arima Y, Yoshida Y, Tanaka H, Nakamura Y, Saida Y, Watanabe M, Watanabe R, Sato J: Prophylactic antibiotics given within 24 hours of surgery, compared with antibiotics given for 72 hours perioperatively, increased the rate of methicillin-resistant Staphylococcus aureus isolated from surgical site infections . J . Infect . Chemother .,
14, 44-50(2008) .
13) 炭山嘉伸 編著 , 消化器外科周術期感染症 , 南山堂(1998) . 14) Hummel AS, Hertel C, Holzapfel WH, Franz CM:
Antibiotic resistances of starter and probiotic strains of lactic acid bacteria . Appl . Environ . Microbiol ., 73, 730-739(2007) .
15) Kiwaki M, Sato T: Antimicrobial susceptibility of
Bifidobacterium breve strains and genetic analysis of streptomycin resistance of probiotic B . breve strain Yakult . Int . J . Food Microbiol ., 134, 211-215(2009) . 16) EFSA: Technical guidance . Update of the criteria
used in the assessment of bacterial resistance to antibiotics of human or veterinary importance . Prepared by the Panel on Additives and Products or Substances used in Animal Feed: EFSA J ., 732, 1-15 (2008) .
1) Kanamori Y, Sugiyama M, Hashizume K, Yuki N, Morotomi M, Tanaka R: Experience of long-term synbiotic therapy in seven short bowel patients with refractory enterocolitis . J . Pediatr . Surg ., 39, 1686-1692(2004) .
2) Wada M, Nagata S, Saito M, Shimizu T, Yamashiro Y, Matsuki T, Asahara T, Nomoto K: Effects of the enteral administration of Bifidobacterium breve on patients undergoing chemotherapy for pediatric malignancies . Support . Care Cancer, 18, 751-759 (2010) .
3) Sugawara G, Nagino M, Nishio H, Ebata T, Takagi K, Asahara T, Nomoto K, Nimura Y: Perioperative synbiotic treatment to prevent postoperative infectious complications in biliary cancer surgery: A randomized controlled trial . Ann . Surg ., 244, 706-714 (2006) .
4) Shimizu K, Ogura H, Goto M, Asahara T, Nomoto K, Morotomi M, Matsushima A, Tasaki O, Fujita K, Hosotsubo H, Kuwagata Y, Tanaka H, Shimazu T, Sugimoto H: Synbiotics decrease the incidence of septic complications in patients with severe SIRS: a preliminary report . Dig . Dis . Sci ., 54, 1071-1078 (2009) .
5) Usami M, Miyoshi M, Kanbara Y, Aoyama M, Sakaki H, Shuno K, Hirata K, Takahashi M, Ueno K, Tabata S, Asahara T, Nomoto K: Effects of perioperative synbiotic treatment on infectious complications, intestinal integrity, and fecal flora and organic acids in hepatic surgery with or without cirrhosis . JPEN J . Parenter . Enteral . Nutr ., 35, 317-328(2011) .
6) Methods for Antimicrobial Susceptibility Testing of Anaerobic Bacteria; Approved Standard-Seven Edition: CLSI M11-A7 vol . 27, No . 2 .
7) Klare I, Konstabel C, Müller-Bertling S, Reissbrodt R, Huys G, Vancanneyt M, Swings J, Goossens H, Witte W: Evaluation of new broth media for microdilution antibiotic susceptibility testing of Lactobacilli,
Pediococci, Lactococci, and Bifidobacteria . Appl . Environ . Microbiol ., 71, 8982-8986(2005) .
8) Moubareck C, Gavini F, Vaugien L, Butel MJ, Doucet-Populaire F: Antimicrobial susceptibility of bifidobacteria . J . Antimicrob . Chemother ., 55, 38-44 (2005) .
9) Peformance Standards for Antimicrobial Susceptibility Testing; Eighteenth Infomational Supplement: CLSI M100-S18 vol . 28, No .1 .
10) Mayrhofer S, van Hoek AH, Mair C, Huys G, Aarts HJ, Kneifel W, Domig KJ: Antibiotic susceptibility of members of the Lactobacillus acidophilus group using broth microdilution and molecular identification of their resistance determinants . Int . J . Food Microbiol .,
144, 81-87(2010) .
11) Kiwaki M, Kushiro A: Antibiotic Susceptibility Testing of Lactobacillus casei by the Broth Microdilution Method and a Survey of Vancomycin-Resistance
謝 辞
本研究の遂行に当たり、ご助言を頂きました株式会社 ヤクルト本社中央研究所 木脇真祐美 副主席研究員に謹 んで感謝の意を表します。
Table 1 Lactobacillus casei シロタ株およびBifidobacterium breveヤクルト株 (BBG-01株)の薬剤感受性 判定a 判定a アミノグリコシド系 Amikacin R R Enterobacteriaceae : 感受性≦16、中間32、低感受性64≦ Gentamycin R R Enterobacteriaceae : 感受性≦4、中間8、低感受性16≦ Kanamycin R R Enterobacteriaceae : 感受性≦16、中間32、低感受性64≦ Streptomycin -b -b 記載なし β-ラクタム系 Ampicillin R R Staphylococcus : 感受性≦0.25、低感受性0.5≦ Carbenicillin S S Enterobacteriaceae : 感受性≦16、中間32、低感受性64≦ Oxacillin S R Staphylococcus :感受性≦2、低感受性4≦ Penicillin R R Staphylococcus : 感受性≦0.12、低感受性0.25≦ セフェム系 Cefaclor R R Staphylococcus : 感受性≦8、中間16、低感受性32≦ Cefazolin I R Staphylococcus : 感受性≦8、中間16、低感受性32≦ Cefbuperazone - - 記載なし Cefdinir I R Staphylococcus : 感受性≦1、中間2、低感受性4≦ Cefmetazole R S Staphylococcus : 感受性≦16、中間32、低感受性64≦ Cefotaxime S R Staphylococcus : 感受性≦8、中間16-32、低感受性64≦ Cefotiam - - 記載なし Cefoxitin R R Staphylococcus : 感受性≦8、中間16、低感受性32≦ Cefpirome - - 記載なし Cefsulodin - - 記載なし Ceftazidime R R Staphylococcus : 感受性≦8、中間16、低感受性32≦ Ceftizoxime S R Staphylococcus : 感受性≦8、中間16-32、低感受性64≦ Ceftriaxone S S Staphylococcus : 感受性≦8、中間16-32、低感受性64≦ Cephalothin S I Staphylococcus : 感受性≦8、中間16、低感受性32≦ Flomoxef - - 記載なし Latamoxef - - 記載なし マクロライド系 Clarithromycin S R Staphylococcus : 感受性≦2、中間4、低感受性8≦ Clindamycin S S Staphylococcus : 感受性≦0.5、中間1-2、低感受性4≦ Erythromycin S S Staphylococcus : 感受性≦0.5、中間1-4、低感受性8≦ Oleandomycin - - 記載なし カルバペネム系 Imipenem R I Staphylococcus : 感受性≦4、中間8、低感受性16≦ Panipenem - - 記載なし キノロン系 Ciprofloxacin R R Staphylococcus : 感受性≦1、中間2、低感受性4≦ Enoxacin R R Staphylococcus : 感受性≦2、中間4、低感受性8≦ Levofloxacin R R Staphylococcus : 感受性≦1、中間2、低感受性4≦ Lomefloxacin R R Staphylococcus : 感受性≦2、中間4、低感受性8≦ Ofloxacin R R Staphylococcus : 感受性≦1、中間2、低感受性4≦ テトラサイクリン系 Minocyclin S S Staphylococcus : 感受性≦4、中間8、低感受性16≦ Tetracyclin S S Staphylococcus : 感受性≦4、中間8、低感受性16≦ ペプチド系 Colistin - - 記載なし Polymyxin B R R Non-Enterobacteriaceae : 感受性≦2、低感受性4≦ Vancomycin R S Staphylococcus : 感受性≦4、中間8-16、低感受性32≦ その他 Chloramphenicol I S Staphylococcus : 感受性≦8、中間16、低感受性32≦ Fosfomycin R R Enterococcus : 感受性≦64、中間128、低感受性256≦ Lincomycin - - 記載なし Metronidazole - - 記載なし Neomycin - - 記載なし Sulfamethoxazole - - 記載なし Trimethoprim R R Staphylococcus : 感受性≦8、低感受性16≦
測定法: broth microdilution method (CLSI M11-A76))
MIC: µg/ml a CLSI M100-S18 あるいはNon-Enterobacteriaceaeの判定基準を用いて感受性を判定した(S: 感受性、I: 中間、R: 低感受性)。 9)には、BifidobacteriumおよびLactobacillusの感受性判定表がないことから、Staphylococcus、Enterococcus、Enterobacteriaceae b CLSI M100-S189)の判定表に記載されていないため、「-」とした。 抗菌薬 256< 128 16 256 MIC MIC B. breve ヤクルト株(BBG-01株) L. casei シロタ株 256 256 256< 128 2 0.5 8 8 8 1 32 8 2 256< 32 256<64 4 1 256 128 64 0.25 <0.25 2 2 128 256< 16 8 64 16 32 256< 16 2 64 <0.25 16 256< 256 64 256< 8 64 0.5 8 2 32 <0.25 0.5 <0.25 64 256 0.25 <0.25 8 8 64 32 2 256< 1 <0.25 256< 256 16 256< 4 CLSI M100-S18の判定基準 16 8 256< 256< 32 256< 32 256< 256< 256< 256< 8 256< 8 256< 16 16 16 128 16 256<