m・}・tzaza*eg
20gag
1℃-
24-- 32fi
(1993
tf{)$&thm
Defecation
Treatment
for
Constipation
in
Children
Severe
Brain
Damage*
with
Masamichi
FURUSAWAi),
Matsuo
SHINB02),
Mineshige
MISAWA3>,
Koji
MATSUMOTO`),
Michiko
OMUROi),
Tatsuyuki
KANEK05)
and
Tomio
OUCHI6)
Abstract
The purpose of thisarticle istoreport on the result of a new treatment forconstipation in
children with severe
brain
damage.
Conventionat
rnethods forthetreatment of constipationin-clude the use of
taxative,
enema, abdominal massage, anddietary
control. However, thesetreatments
have
notbeen
markedly effective.With
thisnew treatment, the postural tuneis
firstnormalized and then a stretch refiex isinduced inthe intestinalwaLl by squeezing out the
fecalbolus retained inthe descending colon.
Manual
manipulationby
aphysical
therapistfa-cilitates theevacuation. The stretch reflex prc)ducesperistalsis,which allows these children to learn the desireto defecate. The physical therapist also
has
the chiidren experience an in-creasein
intra-abdominal
pressure byfiexing
theirlower
trunkforward
while maintaining bothLegsinabduction and flexion,This
defecation
treatment was incorporated intothetherapeuticexercise of 32 children with severe brain damage
(exporimental
group),and 23 children under-went therapeutic exercise witheut defeeationtreatment(control
group).The
change in theircondition was assessed as remarkable, moderate, slight, or no improvement.
The
experimental group was treatedfor
a periodof up to1month or3
years and 9 months(mean
7.0
±8,4
months), and the control groupfor
a period of3
months or7
years and6
months
(mean
23.2±26.9 months). The improvement inconstipation was significantiygreat-er
(p<O.OI)
in
theexperimental group than in thecontrol group.In
the experirnental group,adjunct measures such as laxativeswere used in25 of Lhe children at the initialassessment,
but were only required
in
7{p<O.05)
for
thefinal
assessment.In
the control group, adjunctmeasures were being used in 20 of the children on the initialassessment and were still
required at the finalassessment in17of thechildren
(p>O.05).
The outcome was favorable in9 of the children in whom defecationtreatment was commenced
before
theage of 1year, witha remarkable
improvement
being
observedin
7
of them and a moderateimprovement
being
noted in2.Therefore, defecationtreatme-t should beincorporated
early into the therapeuticprograrn to prevent chronic constipation. Because anticonvulsants are likelyto induce con-stipation as a side effect, thisshould be noted early and prompt initiationof defecation
treat-ment started.
Key words
Chiidren
with severebrain
damage,
Constipation,
Therapeutic
exercise*Il・2]3)41,
E{ittEE'lft'MYt!oifiEif-Novaetrkza
Bobath Mernoria] Hospital
JuntendoUniversityHospital
Yokohama MunicipalRehabilitationCenter
SuitaMunicipal Health Center
5) Surnida Health
and Welfare Center fer the
Handi-capped
6>SakaiMunicipalAkebono Ryoiku Center
{Receivecl
:September21,1991,XAccepted:October 12, 1992)Japanese Physical Therapy Association
NII-Electronic Library Service
JapanesePhysicalTherapy Association
Defecation Treatment for
Constipation
inChildren
1.
Introduction
Inthe management of children with severe
brain
damage, the physical therapist
is
respensiblefor
vital
function
probiems.Management
ofcon-stipation, which
is
often chronicin
these children,must censtitute a part of thetreatment regimen.
Intake of vegetable drinksand fibrousfood is en-couraged as a dietary measure to prevent chronic
constipation in children with severe brain
damagei)'3).However, their oral motor dysfunction usually restricts ingestion Qf foeds, and dietary therapy has been found tobe an unsatisfactory
so-lutionto thisproblern. The use of laxatives and
enema, digital removal of feces4),abdominai
massage5]6), and acupuncture7)B) have also
been
attempted,
Drugs
are often ineffective,becausedrug
resistanceis
tikeEy
todevelop.
Furthermore,
abdominal massagedoes
not significantly promotedefecatien,inthese children whom
postural
tones are abnormal.Furusawa
(1982)9)
previousiy advocatedthera-peutic exercise Lo suppress the abnormal postural
tone in reflex inhibiting
patterns,
to increase the desiretodefecate,and to facilitatestraining. Inthepresent study,
32
children with severebrain
damage were treated by this method and compared
with 23 controls who
did
not receivedefecation
treatment.
Significantly
better
results wereob-tainedintheexperirnental group.
2.
Methods
The
chi]dren with severebrain
damage
who visited the outpatient clinics of BobathMemorial
Hospital,
Sakai
Municipal
Akebono
Ryoiku
Center
for
Handicapped
Children
in
Osaka,
Juntendo
Uni-versity
HospitaL
andTokyo
Women's
Medical
Col-lege
Hospital
in
Tokyo between April,1982 andOc-tober, 1989 were assessed.
Constipation
wasdefined
as the absence ofdefecation
for3-4
days
orlonger.
Thirty-two children consisting of 22 males and
10 femaies in whom defecation treatment was
with
Severe
Brain Damage 25corporated into the therapeutic exercise were
followed up as the experimental group. The
defeca-tjon
treatment
commenced frorn the age oi2
months to 12 years and 6 months with a mean of
2.8=I2.8 years. The
diagnosis
was cerebral palsyin22,rnicrocephatus in8,braindysfunction as a
se-quela of pneumonia in 1,and sequela of meningitis
in 1, According to a classification
by
the posturaltone,20
had
spastic quadriplegia,6had
athetosis,and 6
had
fiaccidity.
Six
of the children(18.7%)
on the initialassessrnent and 8
(25%)
at the final assessment retained some means of mobility, whichwas creeping in2,crawling in2,rolling over in2, and properling themselves
in
thesupine position bypushing
on theheels
in
2.Moderate
or severeintel-lectualhandicap was noted in 28
(87.5%),
and 22children were complicated by epilepsy
(71.9%}.
Twenty-three children with severe
brain
damage
consisting of
10
males and13
iemales
treated at the outpatient clinics of the same institutionswith-out
defecation
treatment werefollowed
up as thecontroL group. Inthis group, therapeutic exercise
commenced
from
the age 3 months to 12years and8
months with a mean of4.2
±3.5
years. Thedi-agnosis was cerebral palsy
in
12,microcephalus in8,
sequela of meningitisin
2,
and sequela ofJapa・
nese encephalitis in 1.According toa class{ficationby
the postural tone spastic quadriplegia wasob-served in 16, athetosis in 5, and flaccidityin
2.
Three
(13.0%)
had a means of tnobility, which wasby creeping. InteLLectualhandicap was observed
in
19
<82.796),
and epilepsy was noted in16(69.6%).
The subjects in both the experimental and
con-trolgroups were treated tonormalize posturaltone, so as toacquire the antigravitational control oi the head and neck, and toIearnto sit.iO)']2)
Defecation
treatment was given in addition to these
treat-ments
in
the
children ofthe
experimental group.Figure I shews a 21-month-old male with
dystonic athetosis due to microcephalus.
In
thephotograph, thischitd istrying to defecate,but he
shows an opisthotonic posture with a strong
26
-\dezatla.
and adducted.
his
anusis
closed.Therefore,
his
opisthotonus must
be
inhibitedfirst(Fig.
2,above).Fo[lowing
this,the therapisthelps
the child tolearnthe antigravitational control of the head and
neck in the midline and sitting position
(Fig.
2,
below). The head and neck control
in
the midlineisimportant for facilitatingclosure of the vocal
Fjg・1.
A
21-month-old
child with dystonico$is. As the child straine(l
for
defecation,
opisthotonus and adduction of the
legs
intensified
due
to associated reacLions,resulting inclosure of hisanus.
Fig. 2.Fig, 2.above
I
Inhibition
of opisthotonus.below 1Long sitting. Spasticityof the bi-lateralhipadduct.ors
is
suppressed byab-ducting
thelegs
toensure opening of theanus
for
defecation.ca
2otsee
1-g
cords
during
straining fordefecation.
Inthe
supineposition,fecalboluses retained in the descending colon are squeezed slowly towards
the
sigmoidcolon and the rectum while inhibitingopisthotonus
and relaxing the
intra-abdominal
pressure.This
is
toinduce
stretch refiexesin
theintestinal
wallCFig.
3,above) and, thus,to produce the desireto
cate. Sincestraining fordefecation tends toinduce
an associated reaction, which adducts the legs,the
therapistincreaseschild's intra-abdominal pressure
by bending histrunk with the legsabducted and
helps
the child experience proper straining(Fig.
3,・
below). The therapist confirms sLraining by the
child and opening of hisanus,
Thc
therapist
teaches
the
mother theseproce-Fig.
Fig.
3. above IThe physica! therapist squeezes
with
fingers
the fecalbolusesretained inthe dcscending colon toward thesig'moid
colon. This
induces
stretch reflexes inthe descending and sigmoid colons and
duces
thedesire
todefecate.
3.
below
lThe
intra-abdominal pressure isincreasqd by fiexing the trunk while
abductingthe]egs.
Thephysicaltherapist
confirrns elicitation of straining and
Japanese Physical Therapy Association
NII-Electronic Library Service
JapanesePhysicalTherapyAssociation
Defecation Treatment forConstipation
dures which are
practiced
for 5-10 mmutes dailywith therapeutic exercise. The treatment should,
however,
be
avoided within1
hour
after meals.In
both
groups, thechildren whohave
oral motordys-function
are also provided with an eating therapyprogrami3)'i6)
by
the speech therapist.The change
in
constipation ivas assessedaccord-ing
to a4.-grade
scale of remarkable, moderate,slight, and no
improvement
(Table
1),and theresults were compared
between
the experimental
Table
1.inChildren with SevereBrain Damage 27
and the control groups, Statisticalanalysls was made
by
thechi-square test.
3.
Results
Defecation
trcatment was continuedfor
up to1
month to
3
years and9
months(mean
7.0±8,4months) intheexperimental group.
Figure
4
sumrnarizesfindings
in
theexperimentaland control groups. Inthe experimental group,
re-markable
improvement
in
constipation wasob-Assessment criteria
for
constipation.Classification
Criterion
Remarkable
Improvement
Defecation
oncemeasures.
every one or two
days
without any adjunctModerate
ImprovementDefecation
once everyures once a fortnight.one
or
two
days,
but
with adjunctmeas-SlightImprovernent
Change
infrequency ofdefecation
from once every four or moredays toonce every two or threedays,with no more than
oceasion-al use of adjunct measures,
No
Improvement
No essentialmenced,changefrom
the time therapeutic exercise
com-(1
Remarkable
ImprovementModerateIrnprevementSlight
No
Improvement Irnprovement Fig. 4.Comparison between theexperimental and control
28
vaYdetu*
served
in
19
of the children(59,4%),
moderateimprovement in
7
(21
.8%),
slight improvement in3
(9,4%),
and noimprovernent
in
3
(9.4%).
Inthecontrol group, remarkable improvement was ob-served
in
4 of the children(17.4%},
and no im-provementin
19
{82.6%).
The
improvement
inthe experimental group was significantly greater(p<
O,Ol)than forthoseinthe control group.
Many mothers used adjunct measures such as
enema,
laxative,
digital
removal offeces,
andstimu-lationof the anus with a cotton swab to relieve
constipation
in
theirchildren.On
theinitial assess-ment, adjunct measures were usedin
25
chj]dren{78.1%)
ef the experimentat group,but
thisnumber was reduced significantly
{p<O.05)
to7
(21.9%)
at thefinal
assessment.In
thecontrol group, adjunct measures were usedin20 of the children
(87.0%)
on theinitial
assess-ment and in17children
(73,9%)
at thefinal assess-ment with no significant difference{p>O.05).
The change inconstipation ef the experimental
(%)1098
ooo70605040302010o
D
RemarkableImprovementua
Moderate Irnprevementeellli
SlightImprove'mentee
No lmpruvement AthetoidType(n:=6>SpasticQuadriplegia{n
;- 20) FlaccidType(n=6} 'fi' i'"20tseg
1."b-group was assessed according toa cLassification
by
the postural tonei7)
(Fig,
5).
Remarkable
improve-ment was ob$erved
in
all6
children with athetosis,but
in those with spastic quadriplegia,remarkableimprovement
was observed in9,moderateimprove-ment
in
6,
slightimprovernent
in
2,
and noim-provement in 3 of the 20 children. Of the 6
'dren
with flaccidity,4showed remarkable
improve-ment, 1 moderate improvement, and 1 slight
im-provement. However, no significant
difference
wasobserved inthe changes among these three
classifi-catlons,
Improvement
in
the experimental group wasanalyzed according to age
<Fig.
6).
The median ageof the children
in
thisgroup was25
months, andwe compared the 16 younger children under 25
months of age with the
16
children aged25
monthsor older.
No
significantdifference
was observed ofchange in constipation between the two groups.
Defecation treatment commenced prior to
the
agevf 1 year in9 children of the experimental group
(Fig.
7)
showed favorable results, with7
showingremarkable improvement and 2 moderate
impreve-ment.
D
fi:,M.l.i.",Ce,M,:"k,e.f
.T,re2aK"r.e.".t,b.e.fgr: M,.th.ua
Commencement of Treatmentafter 2Yearsand 1Month.
109 43 3 21 o Remarkable ]mprovement
{N=19)
Moderate].rnprovement(N
--
7} S]ight No Improvement Improvement(N=3)
CN
=t 3)Fig. 5. Comparison of changes in
stipaLion among three
tions
in
the experimental group.Fig.6. Comparison according toage
in
LheJapanese Physical Therapy Association
NII-Electronic Library Service
JapanesePhysicalTherapy Association
Defecation Treatment forConstipation in
7
2
Children
with SevereBrain Damage
DEFECATiON
29
o
{N=
9)o Remarkable Moderate Slight No
Improvement Improvement Improvement Improvement Fig.
7.
Changein
the constipated condition ofchildren younger than
1
year inmental group.
4.
Discussion
Without appropriate management, constipation
may cause anorexia and abdominal pain,reduce
at-tention span, and
induce
epilepsyiS),pyelone-phritisi9),hemorrhoids, ileus,and flatu]ence,posing
major heatthand social problems.
The improvement in constipation was
signi-ficantlygreater
in
the experimental group thanin
the control group. Since the descending colon
shows no marked pendular segmentatien, or
peri-staltic movement20), tecesare Iikelytobe retained at thissite inchildren with severe brain damage, in
whom the
level
of physical activity is lew,Clinically,
retention of fecalboluses inthedescend-ing
colons of such children can oftenbe
cenfirmedby
palpation.
Hirst
andMcKirdy2i}
induced
the stretch reflexin
the smeoth muscle of theco]on
by
insertingabal-loon intothe guinea pig colon and infiatingit,and
confirmed that the afferent excitation returned to
the colon via autonomic nerve ganglias to induce
peristalsis.
Squeezing of
fecal
boluses retained in thedescending
colon toward thesigmoid colon and therectum using thetherapist'sfingersisconsidered te
elicita similar stretch reflex and promote
peristal-sis. In healthy individuals,
esophago-proximal-colonic reflexes are
induced
by ingestion of food,followed by a gastro-intestinalrefiex and
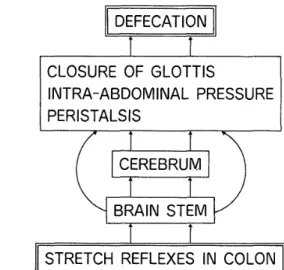
gastro-CLOSURE
OF
GLOTTIS
INTRA--ABDOMINAL
PRESSURE
PERISTALSIS
CEREBRUM
BRAIN
STEM
STRETCH
REFLEXES
IN
COLON
Fig. 8. Mechanism of defecation.
colonic refiex, which produce the desire to
defecate22)'26)
(Fig.
8).Inchildren with severe braindamage,
however,
restriction in food intakedue
tooral motor dysfunction isconsidered to be related
to a lack of desiretodefecate. Even ifthereisthe
desire,the cerebral area thatreceives thissensation may
be
suppressedin
itsresponse.In these chjldren, a stretch reflex was elicited by
squeezing out the
fecaL
boluses
in
theintestine
withthe
fingers
of the ±herapist
and the resultantperi-stalsi$ was considered to have served as sensory
stimuLi, which eLicited the desire todefecate from
thecerebrum.
The
physical therapist needs to modify the in-struction of straining according tothe types ofcer-ebral palsy. In the children with spastie
quad-riplegia or those with dystonic athetosis, crossing of the legs and hyperextension or torsion of the
trunk must
be
inhibited,and the symmetry ofthe
body
be
maintained during the training forstrain-ing.
In athetoid children showing unstable andfluctuatingpostura] tone, the therapistmust
first
stabilize the postural tone and then teach them tocontinue straining without interruption. In
chil-dren with flaccidity,cocontraction of the neck and
trunk muscles isenhanced firstin order to help
them resist gravity. This isconsidered as having
30
ffijZfith\
volving straining.
AIL6 children with athetosis showed remarkable
improvement,
probablybecause
the principalmotility27), which
is
considered to be relativelyintact
in
such children,is
related todefecaLional
maneuvers. The lack of a significant differencein
the changes among the three types of children may
be
ascribedto
the
limitednumber of cases ineachgroup,
In order
to
increasethe
intra-abdorninalpressureby means of closing the vocal cords during
strain-ing,
the
therapist
repeatedlyinterrupted
the
breath
of the children
by
applying strong vibrations withthe hands tothechest. as well as teaching them to
hold
thehead
and neckin
midlinefor
variousbody
positions. This type of handling was considered to
have been helpfulintheprocess of learninghow to straln.
Daily repetition of this
defecation
treatment aspart of the therapeutic exercise was considered as
inducing the development of perception by the
cer-ebrum for
the
desire
to
defecate
as well as of the physical ability tostrain. Itistherefore veryim-portant
to
understand that constipationis
a resultof sensorimotor impairment. The physical thera-pistmllst recognize
that
the
therapeutic
exercise to promote defecationis
by
treatment of thesensorimotor regions of the centraL nervous system.
Contents
and number of meals and waterintake
must be assessed on Lhe basisof thisapproach in connection with the sensorimotor system.
Constipation is more likely to take a chronic
course
in
older children andis
moredilficult
totreat
(Fig.
6),but easier and lesslikelytorecur ininfants
(Fig.
7). Therefore, defecation treatmentshould be initiatedearly ifthereisany sign of con-stipation.
Children
with severe braindamage
are oftencomplicated
by
epilepsy. Anticonvulsantdrugs
were administered to
18
of the22
children withep-ilepsy
inthe experimenta] group and to 15of the17
children with epilepsyin
the
control group. Thesedrugs
have a side effect olsuppres$ingintes-eg
20igeg
1Il;Fig. 9.
Holding
thechild ina positiontopromote
defecation.
tinal peristalsiswhich is a cause of
constipa-tion28)29).
Therefore,
caution is necessary whenthe children with severe brain damage are taking
these drugs,
The
physical therapist isexpectedto
prevent constipationby
introducing
defecation
treatment early when the signs of constipation are noted.
Recurrence of constipation
is
more likelyduring
summer when perspirationincreases,
andduring
winter when activity
is
reduceddue
tocoldweath-er. Iti$thereforeimportant forthe therapisttoask
the parents at the times whether their children
have
any sign of constipation.
Along
with thedefecation
treatment,it
is
recorn-mended toteachmothers theway toholdthechildren
in
a position thatincreases
theintra-abdominal
pressure
(Fig.
9).Presently,more than 60% of preschool children
who go to day care centers for the handicapped
have severe disabilitiesand are dependent for
put-ting on and taking off clothes, eating, toiletting,
social mobility, and communication3D). Therefore,
many children encounter the problem of con-stipation, and itsmanagement by the parents with
such measures as was
introduced
here
is
needed.Japanese Physical Therapy Association
NII-Electronic Library Service
JapanesePhysicalTherapy Association
Defecation Treatment forConstipation inChildren with
Severe
Brain
Damage31
forthat matter, many physical therapiststend to
think
thatthe
management of constipation isnot apart of their responsibility. Therapists shouLd
make a cornbined effort with the mothers in the
treatrnentof constipation so as toprevent its per-slstence.
5.
Conclusion
Constipation
improved
significantlyin
the experi-mental group, in which thedefecation
treatmentwas
incorporated
with the therapeutic exercise.This treatment may
produce
satisfactory resultswhen
it
is
initiated
early at thefirst
signs of con-stipation,References
1)KajiuraI:Management of habilitationincerebral
sied children.
Iin
Japanese],,
Rinsho Kange 6(14):
2]66-2176,1980.
2) Yoneyama A, Kodama K,Kitazumi E IConstipation.
rin
Japanese]
ShoniKango 11(1):83-87,
1988.3) Mineshima N :Milk feeding and rneals.
[in
Japanese]Hagemi 307:12-14, 1981.
4) Riggs H :The GastrointestinaiTracL InIChild Health
and the Family:NursingConcept$and Managemeiit.
(ed.by SteeleSLMasson Publishing,New York,1981,
pp 293-324.
5) Tappen FM :Massagc Techniques.Macmiltan.New
York, 1961,pp 77-78.
6) Kamenetz HL :Historyof Massage,In:Massage,
nipulation and Traction.
(ed,
by Licht S),ElizabethLicht Publisher,New Haven,1960,pp 3-37.
7) Yamashita M:Sinkyu Chiryougaku
[Acupuncture
Treatment]
[i]
Japanese]
IshiyakuShuppan, Tokyo,1975,pp 230-240.
8) YamashitaM 1Chugoku Shinkyugaku Kougi
[Lecture
on Chinese Acupuncture]
[in
Japanesellkanpo,Tokye,1977,pp 450-452.
9) Furusawa M INeurodevclopinentaltreatment for
stipation in children with scvere brain dysfunction.
[in
Japanese]
Ri・ Su・
Ryoho 16 <3)I199-2e3,1982.10) Bobath K :A Neurophysiological Basis forthe
ment of CerebralPalsy, WilliamHeinemann Medical
Books Ltd.,London, 1980, p5.
11)Bebath K,Bobath B :The Neuro-Developinental ment, ClinicsinDevelopmental Medicine, No, 90.
(ed.
byScruttonD),SpasticInternational Medical
tions,Oxford,1984,pp 6-18,
12) Bryce J:The management of spasticity in children.
Physiotherapy6Z
<11)
:353-357,1976.13)Mueller HA:Facilitating Feeding and Prespeech.
Physica] Servicesin the Developmental Disabilities,
CharlesC.Thomas, London, 1972,pp. 183-205.
14)Morris SE:Program GuidelinesforChildrcn with
Feeding Problems,ChildcraftEducation Corp. New
Jersey,1977.
15)Comior FP, WilliamsonGG, Siepp
JM
:Pre-spccch.Program Guide forInfants and Toddlers, Teacher$
!egePress,New York,1978,pp 183-205.
16)WaltR :The feeding experience :Psychologicalaspects.
The Seuth African
J
NeurodeveloprnentalTherapy10{z):12-14,1986,
17)BobathB,BobathK :MotorDcvelopmentinthe
ent Types of CerebralPalsy.WilliamIIeinemann
cal BooksLtd.London,1978,pp 57-82.
18}Roy C C,Silverrnan A :GastrointestinalTract.In:
rent PediatricDiagnosis& Treatment,Ed, 6,{ed.by
Kempe CH, Silver HK and O'Brien),Lange Medical
Publications,LosAItos,CA,1980,pp 441-475.
19)Kumita K:Why is Defecation Training Needed?
ToiletTraining forChildren.
[in
Japanese]
IryoTosheShuppansha,Tokyo, 1976,pp 5-17.
20)Higashihara Y:Seirigaku
[Physiology]
[in
nese] ,Bukkyo Univ,Kyoto
Japan,
1988,pp 99-11O.21}HirstGDS, McKirdy HC :A nervous mechanism for
descendinginhibition inguinea-pig small intestine.
J
Physiol238:l29-143,1974.
22) Wood JD:Physiolegy of the Enteric Nervous
System.Physiologyof the GastrointestinalTract,Vol.
1.Laven Press,New York, 1981,pp ] 37.
23)SchotteliusBA, SchottcliusDD ITextbook of ogy. Ed.18,C V Mosby, St.Louis, 1978,pp 388-404.
24)Kutchai HC:The GastreintestinalSystem. In:
Physiolegy,
(ed
by Bern RM, Levy MN, CV Mosby,St.I.ouis),1983, pp 743-820.
25)Okabe H :DigestiveSystems.Autonomic Nerves in
rustration.
[in
Japanesol,(ed
byIrikiM),FujitaKikakuShuppan,Saitama,
Japan,
1985,pp 250-268.26) Okabe HIPhysielogy of defecation.
Iin
Japanese]
Sogo Rihabiriteshon]5
<6)
:433-440,1987.27) Schaltenbrand GIThe Development of human
tnotility and motor disturbances, Arch Neurol
Psychiat 20:720 728,1927.
28)LivingstonS:Comprehensive Management of sy in Infancy, Child and Adolescence. Charles C.
Thomas, Springfield,1972,pp 350-377.
29)SaikiM IDisordersof defecation inchildren,
lin
nese, ShoniKungo 3: 1237-1243,]980.
30)Associationof All
Japan
Day Care Ccntcrs forschool Children with Handicap :Summary of
tion Surveys
[in
Japane6el/
, Associatioll of AllJapan
Day Care Centers for Preschool Children with