ICU における PPI・H2B の副作用
2015年10月20日(火)
東京慈恵会医科大学付属病院
薬剤部
鮎川 英明
1
目次
• PPI vs. H2B
• 院内肺炎
•
Clostridium difficile
感染症
• 経腸栄養とH2B
• 低Mg血症
• まとめ
ü ストレス潰瘍予防の適応(参考)
ü クロピドグレルとオメプラゾール(参考)
2
PPI vs. H2B
ICU患者におけるメタ解析と副作用
ICU患者において上部消化管出血予防としてのPPIとH2B
を比較したメタアナリシス
Methods : MEDLINE、EMBASEなどで検索した1200以上
の文献から14のRCTを選択
Pa=ents : 成人のICU入室患者1720例
Outcome :
・Primary outcome
Clinically important upper gastrointes=nal bleeding
Overt upper gastrointes=nal bleeding
・Secondary outcome
院内肺炎、CD感染、ICU死亡率、ICU滞在期間
2014.7.22勉強会 「H2B vs. PPI」参照
Proton Pump Inhibitors Versus Histamine2 Receptor Antagonists for
Stress Ulcer Prophylaxis in CriDcally Ill PaDents: A SystemaDc Review
and Meta-Analysis.
Crit Care Med 2013; 41:693–705
4
•
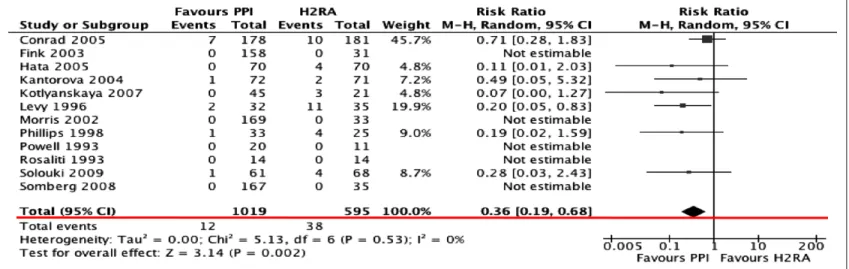
Clinically important upper gastrointes=nal bleeding
→
PPI
が
beSer (RR:0.36(95%CI:0.19–0.68), p =0.002, I
2
= 0%)
•
Overt upper gastrointes=nal bleeding
→
PPI
が
beSer (RR:0.35(95%CI 0.21–0.59), p <0.0001, I
2
=15%)
2014.7.22勉強会 「H2B vs. PPI」参照
Alhazzani et al 700 www.ccmjournal.org -ARCHSensitivity Analysis
Sensitivity analysis was conducted examining the effect of
using risk difference as an estimate of effect for clinically
im-portant bleeding (risk difference −0.03; 95% CI −0.05 to 0.00,
p = 0.06, I
2= 52%) and overt bleeding (risk difference −0.06;
95% CI −0.11 to −0.02, p = 0.009, I
2= 80%), although
signifi-cant heterogeneity was present. The second sensitivity analysis
excluded trials pub lished in abstract form (22–25). Clinically
important bleed ing (RR 0.42; 95% CI 0.21–0.84; p = 0.01;
I
2= 0%) and overt bleeding (RR 0.40; 95% CI 0.25–0.67;
p = 0.0004; I
2= 12%) were significantly reduced, consistent
with the main analysis.
DISCUSSION
In this meta-analysis, we found that PPIs were more effective than
H2RAs at preventing clinically important bleeding and overt
gastrointestinal bleeding. The main reservation about using PPIs
Figure 4. Forrest plot for clinically important gastrointestinal bleeding outcome. Data from 12 trials were included in the analysis using random effects
model. The use of proton pump inhibitor (PPI) was associated with a significantly lower risk of clinically important bleeding compared with histamine 2 receptor antagonist (H2RA) (risk ratio [the same as relative risk] [RR] 0.36; 95% confidence interval [CI] 0.19–0.68). M-H = Mantel Haenszel.
TABLE 3. Evidence Profile Using GRADE Approach
Quality Assessment No. of Patients Effect
Quality Impor-tance No. of
Stud-ies Design Risk of Bias Inconsistency Indirectness Imprecision Proton Pump Inhibitor Receptor AntagonistHistamine 2 Confidence Interval)Relative (95% Absolute
Clinically important bleeding
12 Randomized
trials Serious
a No serious
inconsistency indirectnessNo serious imprecisionSerious b 12/1019 (1.2%) 38/595 (6.4%) RR 0.36 (0.19–0.68) 46 fewer per 1000 (from 23 fewer to 58 fewer) Low Critical Overt upper gastrointestinal bleeding
14 Randomized
trials Serious
a No serious
inconsistency indirectnessNo serious imprecisionNo serious 41/1077 (3.8%) 101/643 (15.7%) RR 0.35 (0.21–0.59) 113 fewer per 1000 (from 72 fewer to 138 fewer) Moderate Important Mortality
8 Randomized
trials Serious inconsistencyNo serious indirectnessNo serious imprecisionNo serious 127/726 (17.5%) 100/470 (21.2%) RR 1.01 (0.83–1.24) 0 fewer per 1000 (from 42 fewer to 51 more) Moderate Critical Nosocomial pneumonia
8 Randomized
trials Serious
a No serious
inconsistency indirectnessNo serious imprecisionNo serious 66/626 (10.5%) 50/474 (10.5%) RR 1.06 (0.73–1.52) 6 more per 1000 (from 28 fewer to 55 more) Moderate Critical
This table is generated using the GRADEprofiler software that summarizes the quality of evidence for individual outcomes based on five main domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. For each outcome, the quality of evidence is presented along with the clinical importance of the outcome.
aDowngraded for risk of bias mainly due to lack of or incomplete blinding.
bDowngraded for low number of events rather than confidence interval. Feature Article
Critical Care Medicine www.ccmjournal.org 701
in the critical care setting rather than H2RAs is the potential to increase the incidence of nosocomial pneumonia (38, 39); how-ever, trials do not suggest such a difference. Mortality and length of ICU stay were not affected. None of the trials reported C.
dif-ficile infection, although a systematic review of 12 observational
studies evaluating 2,948 patients with C. difficile found an asso-ciation with antisecretory therapy (OR 1.94; 95% CI 1.37–2.75).
The association was present for PPI use (OR 2.05; 95% CI 1.47–2.85) and for H2RA use (OR 1.47; 95% CI 1.06–2.05), with no difference between PPIs and H2RAs (p = 0.17) (40).
There was no heterogeneity of results in this meta-analysis. Subgroup analyses examining dosing and frequency of PPI administration, and specific populations (medical vs. surgical ICU patients, and Asian vs. non-Asian patients) showed no
sig-Figure 5. Forrest plot for overt upper gastrointestinal bleeding outcome. Data from 14 trials were included in the analysis using random effects model.
The use of proton pump inhibitor (PPI) was associated with a significantly lower risk of overt bleeding compared with histamine 2 receptor antagonist (H2RA) (risk ratio [the same as relative risk] [RR] 0.35; 95% confidence interval [CI] 0.21–0.59). M-H = Mantel Haenszel.
TABLE 3. Evidence Profile Using GRADE Approach
Quality Assessment No. of Patients Effect
Quality Impor-tance No. of
Stud-ies Design Risk of Bias Inconsistency Indirectness Imprecision Proton Pump Inhibitor Receptor AntagonistHistamine 2 Confidence Interval)Relative (95% Absolute
Clinically important bleeding
12 Randomized
trials Serious
a No serious
inconsistency indirectnessNo serious imprecisionSerious b 12/1019 (1.2%) 38/595 (6.4%) RR 0.36 (0.19–0.68) 46 fewer per 1000 (from 23 fewer to 58 fewer) Low Critical
Overt upper gastrointestinal bleeding 14 Randomized
trials Serious
a No serious
inconsistency indirectnessNo serious imprecisionNo serious 41/1077 (3.8%) 101/643 (15.7%) RR 0.35 (0.21–0.59) 113 fewer per 1000 (from 72 fewer to 138 fewer) Moderate Important Mortality
8 Randomized
trials Serious inconsistencyNo serious indirectnessNo serious imprecisionNo serious 127/726 (17.5%) 100/470 (21.2%) RR 1.01 (0.83–1.24) 0 fewer per 1000 (from 42 fewer to 51 more) Moderate Critical Nosocomial pneumonia
8 Randomized
trials Serious
a No serious
inconsistency indirectnessNo serious imprecisionNo serious 66/626 (10.5%) 50/474 (10.5%) RR 1.06 (0.73–1.52) 6 more per 1000 (from 28 fewer to 55 more) Moderate Critical This table is generated using the GRADEprofiler software that summarizes the quality of evidence for individual outcomes based on five main domains: risk of
bias, inconsistency, indirectness, imprecision, and publication bias. For each outcome, the quality of evidence is presented along with the clinical importance of the outcome.
aDowngraded for risk of bias mainly due to lack of or incomplete blinding. bDowngraded for low number of events rather than confidence interval.
•
CD感染について検討し
た研究は、選択した
RCT
に含まれなかった
・院内肺炎
・
ICU死亡率
・
ICU滞在期間
に差は見られなかった
院内肺炎 相対リスク
1.06;
95%信頼区間
0.73–1.52; p = 0.76; I
2
= 0%
ICU死亡率 相対リスク1.01;
95%信頼区間
0.83–1.24; p = 0.91; I
2
= 0%
ICU滞在期間 相対リスク-0.54;
95%信頼区間
-2.20–1.13; p = 0.53; I
2
= 0%
2014.7.22勉強会 「H2B vs. PPI」参照
Alhazzani et al 702 www.ccmjournal.org -ARCH Figure 6. Forrest plot for nosocomial pneumonia outcome. Data from eight trials were included in the analysis using random effects model. The risk of nosocomial pneumonia was similar in both groups risk ratio [the same as relative risk] [RR] 1.06; 95% confidence interval [CI] 0.73–1.52). H2RA = hista-mine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.Figure 7. Forrest plot for ICU mortality outcome. Data from eight trials were included in the analysis using random effects model. The risk of death dur-ing the ICU stay was similar in both groups (risk ratio [the same as relative risk] [RR] 1.01; 95% confidence interval [CI] 0.83–1.24). H2RA = histamine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 8. Forrest plot for ICU length of stay outcome. Data from five trials were included in the analysis using random effects model. There was no statistically significant difference between groups (weighted mean difference −0.54; 95% confidence interval [CI] −2.20 to 1.13). H2RA = histamine 2 receptor antagonist; PPI = proton pump inhibitor.
Alhazzani et al
702 www.ccmjournal.org -ARCH Figure 6. Forrest plot for nosocomial pneumonia outcome. Data from eight trials were included in the analysis using random effects model. The risk of nosocomial pneumonia was similar in both groups risk ratio [the same as relative risk] [RR] 1.06; 95% confidence interval [CI] 0.73–1.52). H2RA = hista-mine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 7. Forrest plot for ICU mortality outcome. Data from eight trials were included in the analysis using random effects model. The risk of death dur-ing the ICU stay was similar in both groups (risk ratio [the same as relative risk] [RR] 1.01; 95% confidence interval [CI] 0.83–1.24). H2RA = histamine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 8. Forrest plot for ICU length of stay outcome. Data from five trials were included in the analysis using random effects model. There was no statistically significant difference between groups (weighted mean difference −0.54; 95% confidence interval [CI] −2.20 to 1.13). H2RA = histamine 2 receptor antagonist; PPI = proton pump inhibitor.
Alhazzani et al
702
www.ccmjournal.org -ARCHFigure 6. Forrest plot for nosocomial pneumonia outcome. Data from eight trials were included in the analysis using random effects model. The risk of
nosocomial pneumonia was similar in both groups risk ratio [the same as relative risk] [RR] 1.06; 95% confidence interval [CI] 0.73–1.52). H2RA = hista-mine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 7. Forrest plot for ICU mortality outcome. Data from eight trials were included in the analysis using random effects model. The risk of death
dur-ing the ICU stay was similar in both groups (risk ratio [the same as relative risk] [RR] 1.01; 95% confidence interval [CI] 0.83–1.24). H2RA = histamine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 8. Forrest plot for ICU length of stay outcome. Data from five trials were included in the analysis using random effects model. There was no
statistically significant difference between groups (weighted mean difference −0.54; 95% confidence interval [CI] −2.20 to 1.13). H2RA = histamine 2 receptor antagonist; PPI = proton pump inhibitor.