第 52 回日本感染症学会東日本地方会総会学術講演会座長推薦論文
Erysipelothrix rhusiopathiae による感染性心内膜炎の 1 例
1)国保旭中央病院内科,2)同 検査科,3)聖路加国際病院内科感染症科,4)国立感染症研究所細菌第二部
小寺 聡
1)中村 朗
1)大江 健二
2)古川 恵一
3)柴田 尚宏
4)荒川 宜親
4)(平成 17 年 7 月 23 日受付)
(平成 18 年 2 月 15 日受理)
Key words : Erysipelothrix rhusiopathiae , endocarditis, serotype
序 文
Erysipelothrix rhusiopathiae(豚丹毒菌)は,人に感 染する場合には限局性の皮膚軟部組織病変が多い.
我々は E. rhusiopathiae による感染性心内膜炎を経験
したが,敗血症例の報告はまれであり,海外での報告 を含めて 100 例程度である.また,人の敗血症で血清 型まで明らかにされたのは本症例が世界初である.
症 例
症例:67 歳,男性.
主訴:腰痛,発熱.
生活歴:日本酒 1 升! 日,タバコ;30 本! 日.
既往歴:特記事項なし.
職業:漁師.
現病歴:2002 年 10 月より腰痛が出現した.2002 年 11 月下旬より週 1 日 39℃ の発熱が出現した.2003 年 3 月 18 日に発熱,腰痛が持続するために当院内科を 受診し,精査加療目的で入院となった.
入院時現症:身長 158cm,体重 48kg,血圧 118 ! 66 mmHg,脈拍 100 回! 分(整),体温 36.0℃,眼瞼結膜 に貧血なし,眼球結膜黄疸なし.心音:収縮期雑音 Levine II! VI(胸骨左縁第 2 肋間).呼吸音:正常.
腹部:平坦かつ柔軟,腫瘤をふれず.両手掌にびらん を認めた.
入院時検査所見(Table 1):末梢血では白血球は 8,400! µL,CRP が 7.8mg! dLであった.血液生化学で LDH の上昇と,尿潜血を認めた.血液培養から E. rhu- siopathiae(血清型 1b 型)が検出された.感受性は PCG に対して良好であった.心エコーで,僧帽弁に長径 20 mm,大動脈弁に 6mmの可動性のある疣贅を認めた.
また,僧帽弁逆流 III 度,大動脈弁逆流 II 度を認めた.
臨床経過(Fig. 1):入院後,ABPC 12g! 日で治療 を開始した.入院 4 日目より解熱傾向を認め,入院 9 日目の血液培養は陰性であった.入院 15 日目の心エ コーでは疣贅は消失していた.
入院後より自発性が低下し,頭部 MRI で感染性心 内膜炎による多発性脳塞栓症を認めた.また,入院 10 日目よりうっ血性心不全を認めたが,弁置換を行うこ となく改善した.その他,腹部 CT で左腎梗塞を認め た.ABPC を計 6 週間投与した後,入院 66 日目に独 歩で自宅退院した.
考 察
E. rhusiopathiae は,細菌学的には芽胞を形成しな
いグラム陽性桿菌で,通性嫌気性,非運動性の菌であ る.グラム陽性桿菌と同定後,Listeria monocytogenes, Lactobacilli, Corynebacteria とは溶血の型,運動性,
カタラーゼ産生性,H
2S 産生性により区別され得た
1). 本症例では,菌の同定はアピコリネ(bioM rieux)
にて可能であり,国立感染症研究所にて 16S rRNA 解析を行い,確定診断を得た.
現在,E. rhusiopathiae はその菌体抗原とそれに対す る家兎免疫血清を用いたゲル内沈降反応により,少な くとも 1〜23 の血清型と N 型(型特異抗原性を欠く)
に分類される
2).人に感染した E. rhusiopathiae の血清 型の報告は,これまで Cross らの 1 例のみで,2b 型 であった
3).Cross らの報告では感染型の記載はない.
敗血症型の血清型の報告はなく,我々が初めて同定を 行い,1b 型との結果を得た.豚においては,血清型 と症状との関係も指摘されており,血清型 1a,1b は 急性の経過が多く,2 型は慢性な経過が多いとの報告 がある
4).しかし,報告により血清型と臨床経過の関 連は異なり,今のところ意見の一致は得られていな い
5).また,豚の扁桃からは 1,2 型(1a,1b,2a,2b)
症 例
別刷請求先:(〒876―0851)佐伯市常盤東町6 番 80 号
小寺内科医院 小寺 聡
Fig. 1 Clinicalcourse Table 1 Laboratory data on admission
MIC mg/dL
7.8 CRP
/μL 8,400 WBC
S 0.03 PCG
g/dL 8.2 T.P.
% 74 Neu.
S 0.03 ABPC
g/dL 3.1 Alb
% 17 Lym.
S 0.25 CEZ
IU/L 556 LDH
% 5 Mono.
1 CTM
IU/L 18 GOT
% 3 Eos.
S 0.03 CDTR
IU/L 8 GPT
% 0.5 Baso.
S 0.25 CTX
mg/dL 0.6 T.Bil
/μL 346×104 RBC
S 0.13 CFDM
mg/dL 16 BUN
g/dL 10.4 Hb.
S 0.13 IPM/CS
mg/dL 0.8 Cr
% 31.0 Ht.
R 8 EM
mEq/L 141 Na
/μL 11.5×104 Plt.
S 0.13 CLDM
mEq/L 3.6 K
S 0.5 MINO
mEq/L 104 Cl
が高頻度に分離されるが
6),本症例の感染経路と考え られる魚においては,血清型の検討はなされていな い.
E. rhusiopathiae と生化学的に非常に同一性が高
く,鑑別が困難な菌として Erysipelothrix tonsillarum がある
2).本菌は犬に病原性はあるが,豚,鶏には病 原性がなく,人の感染例の報告もない. E. rhusiopathiae と E. tonsillarum との鑑別は,16S rRNA 解析のみで は困難であり,Shimoji らにより報告されたプライ マー
7)を使用し,PCR を行う.同様の方法で我々も鑑 別を行い,E. rhusiopathiae との結果を得た.
E. rhusiopathiae は自然界に広く存在しており,腐
敗した物質のなかでも数カ月感染性を保つことができ る.また,魚,貝,鳥,昆虫などあらゆる動物から検 出される.感染動物からの菌の排出が環境への汚染と なり,人への感染につながると考えられている.すべ ての感染動物のなかで,豚が最も重篤に E. rhusiopa-
thiae に感染するとされている
1).
E. rhusiopathiae の人への感染は,この菌を保菌し
た物質による皮膚損傷,創傷部への保菌物質の混入に
よりおこるとされている.そのため,保菌物質との接
触が多い肉屋,漁師などの職業に多く,職業病として
認識されている
1).MOLIN らの報告
8)では,オースト
ラリアの食肉処理場勤務者 138 人のうち,20 人が E.
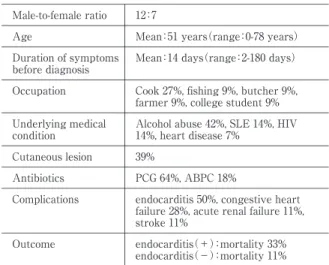
Table 2 Clinicalfeatures of19 cases ofErysipelothrix rhu- siopathiaesepticemia10-28)
12:7 Male-to-female ratio
Mean:51 years(range:0-78 years)
Age
Mean:14 days(range:2-180 days)
Duration ofsymptoms before diagnosis
Cook 27%,fishing 9%,butcher 9%, farmer 9%,college student 9%
Occupation
Alcoholabuse 42%,SLE 14%,HIV 14%,heart disease 7%
Underlying medical condition
39%
Cutaneous lesion
PCG 64%,ABPC 18%
Antibiotics
endocarditis 50%,congestive heart failure 28%,acute renalfailure 11%, stroke 11%
Complications
endocarditi(+)s :mortality 33%
endocarditi(-)s :mortality 11%
Outcome
rhusiopathiae 抗体陽性であり,類丹毒の既往歴が 16
人にあった.このことから,食肉処理場などで E. rhu-
siopathiae が広く存在していると考えられる.
感染は限局性皮膚病変型(類丹毒),全身性皮膚病 変型,敗血症型の 3 つのタイプがある
1).限局性皮膚 病変型が最も多く,辺縁明瞭で軽度隆起を伴う紫色の 病変となる.これは手に起こることが多く,類丹毒と して知られている.潜伏期間は 4 日以下で,かゆみ,
痛みなどが強いことが特徴である.無治療でも 3〜4 週間で改善する.全身性皮膚病変型は,原発病変から その他の部位に進展するもので類丹毒のうち 1! 100 程 度とされている.この場合,発熱,関節痛,筋肉痛,
頭痛などが生じる
5)9).
敗血症型は極めてまれで,世界での報告は 100 例程 度である.過去 13 年間の E. rhusiopathiae による敗血 症の英語論文 19 例
10)〜28)をまとめた(Table 2).男女 比は 12 対 7 と男性に若干多く,年齢は中高年に多く みられた.潜伏期間は 2〜4 週が多く,中央値で 14 日 であった.職業はコックが 27% と多く,そのほか漁 師,肉屋など動物を扱う職種を多く認めた.背景は,
アルコール多飲が 42% と多く,心疾患は 7% と稀で あった.皮膚病変を有する症例は 39% と高率であり,
感染経路は経皮,経口とも同程度認めた.敗血症の治 療に用いられた抗菌薬はペニシリン系が 8 割を占め,
合併症は感染性心内膜炎が 50% と高率であった.予 後は感染性心内膜炎を起こした場合には半数以上の症 例で弁置換術が施行されており,死亡率も 33% と高 率であった.Gary らの報告
9)では,感染性心内膜炎で は弁破壊性が強く,塞栓症状を伴うことが多いとさ れ,大動脈弁を含む症例は 70% と他の菌の感染性心 内膜炎(50%)に比べて多い.近年,感染性心内膜炎 の死亡率は低下しているが,E. rhusiopathiae において
は 38% と依然として高く,他の菌と比べ 2 倍であっ た.
心内膜炎を起こすグラム陽性桿菌として L. monocy- togenes,Diphtheroids,Lactobacilli,Bacillus が あ げ ら れる.鑑別点として Diphtheroids は人工弁,三尖弁へ の感染が多いとされている
9).Bacillus は薬物乱用者に 多く,三尖弁への感染が特徴的である
9).E. rhusiopa-
thiae は,L. monocytogenes とは類似点が多いが,皮膚
病変を持つこと(36%),動物と接する職業に従事し ていること(89%),アルコール多飲歴(33%)があ ることなどが特徴的である
29).
抗菌薬の感受性は,ペニシリン系,セフェム系,ク リンダマイシン,エリスロマイシンは良好である.テ トラサイクリン,クロラムフェニコールの感受性は一 定でない.ST 合剤,アミノグリコシド,バンコマイ シンには耐性を示す
1).バンコマイシンはグラム陽性 菌敗血症の初期治療薬(empiric thyerapy)として使 用されることが多いが,E. rhusiopathiae では無効であ り注意が必要である.本菌に対 す る ペ ニ シ リ ン の MICs が 0.0025-0.06 µ g ! mLであり MBCs が 0.0025-0.75 µg! mLであることからペニシリン G 1,200 万〜2,000 万単位が第一選択となる.感染性心内膜炎において治 療期間は 4〜6 週が適切とされるが,より短い期間の 治療で成功した報告もある.
E. rhusiopathiae による感染性心内膜炎はきわめて
稀である.グラム陽性桿菌による感染性心内膜炎では 職業歴,動物との接触歴に注意し,E. rhusiopathiae の 鑑別が必要である.本菌は弁破壊性が強く,感染性心 内膜炎例での死亡率が高いため早期の診断と治療開始 が重要である.また,E. rhusiopathiae の血清型と病型 に関しては,今後更なる検討が必要である.
謝辞:E. rhusiopathiaeの血清型を同定して戴いた動物衛 生研究所の横溝祐一先生,下地善弘先生に深謝します.
文 献
1)Annette CR, Farrar WE:
Erysipelothrix rhusiop- athiae
. In :Mandell GL, Bennett JE, Dolin R(eds).Principle and Practice of Infectious Dis- eases, (ed 5). New York, Churchill Livingstone, 2000;p. 2226―7.
2)Takahashi T, Fujisawa T, Tamura Y, Suzuki S, Muramatsu M, Sawada T,
et al.:DNA
related- ness amongErysipelothrix rhusiopathiae
strains representing all twenty-three serovars and Ery- sipelothrix tonsillarum. Int J Syst Bacteriol 1992;42(3):469―73.3)Cross GMJ, Claxton PD:Serological classificati- on of Australian strains of
Erysipelothrix rhu-
siopathiae
isolated from pigs, sheep, turkeys and man. Aust Vet J 1979;55:77―81.4)Kucsera G:Serological typing of
Erysipelothrix rhusiopathiae
strains and the epizootiological sig- nificance of the typing. Acta Vet Acad Sci Hung 1979;27:19―28.5)Brooke CJ, Thomas V:
Erysipelothrix rhusiopath- iae
: bacteriology, epidemiology and clinical mani- festations of occupational pathogen. J. Med. Mi- crobiol 1999;48:789―99.6)Stenstr m IM, N"rrung V, Ternstr m A, Molin G:Occurrence of different serotypes of
Ery- sipelothrix rhusiopathiae
in retail pork and fish.Acta vet. Scand 1992;33:169―73.
7)Shimoji Y, Mori Y, Hyakutake K, Sekizaki T, Yokomizo Y:Use of an enrichment broth culti- vation-PCR combination assay for rapid diagno- sis of swine erysipelas. J Clin Microbiol 1998;
36:86―9.
8)Molin G, S derlind O, Ursing J, Ternstr m A, L wenhielm C:Occurrence of
Erysipelothrix rhu- siopathiae
on pork and in pig slurry, and the dis- tribution of specific antibodies in abattoir work- ers. J Bacteriol 1989;67:347―52.9)Gary L Gorby, James E Peacock Jr:
Erysipe- lothrix rhusiopathiae
Endocarditis:microbiologic, epidemiologic, and clinical features of occupa- tional disease. Rev Infect Dis 1988;10:317―25.
10)Fakoya A, Bendall RP, Churchill DR, Doherty JF:
Erysipelothrix rhusiopathiae
Bacteraemia in a patient without endocardits. J Infect 1995;30:180―1.
11)Venditti M, Gelfusa V, Catelli F, Brandimarte C, Serra P:
Erysipelothrix rhusiopathiae
endocardi- tis. Eur. J. Clin. Microbiol. Infect Dis 1990;1:50―2.
12)Umana E:
Erysipelothrix rhusiopathiae
:an un- usual pathogen of infective endocarditis. Int J Cardiol 2003;88:297―9.13)Hill DC, Ghassemian JN, Fayetteville :
Erysipe- lothrix rhusiopathiae
endocarditis:clinical featu- res of an occupational disease. South Med J 1997;90:1147―8.14)Garcia-Restoy Enric, Espejo Elena, Bella Feliu, Llebot Juanjo:Bacteremia due to
Erysipelothrix rhusiopathiae
in immunocompromised hosts without endocarditis. Rev of Infect Dis 1991;13:1252―3.
15)Gim nez M, Fern!ndez P, Padilla E, Matas L, Ausina V:Endocarditis and acute renal failure due to
Erysipelothrix rhusiopathiae
. Eur. J. Clin.Microbiol. Infect. Dis 1996;15:347―8.
16)Artz AL, Szabo S, Zabel LT, Hoffmeister HM:
Aortic valve endocarditis with paravalvular ab- scesses caused by
Erysipelothrix rhusiopathiae
. Eur. J. Clin. Microbiol Infect. Dis 2001;20:587―8.
17)Sheng WH, Hsueh PR, Hung CC, Fang CT, Chang SC, Luh KT:Fatal outcome of
Erysipe- lothrix rhusiopathiae
bacteremia in a patinent with oropharyngeal cancer. J. Formos Med. As- soc 2000;99:431―4.18)MacGowna AP, Reeves DS, Wright C, Glover SC:Tricuspid valve infective endocarditis and pulmonary sepsis due to
Erysipelothrix rhusiopa- thiae
successfully treated with high doses of ciprofloxacin but complicated by gynaecomastia.J Infect 1991;22:100―1.
19)Jones N, Khoosal M:
Erysipelothrix rhusiopathiae
septicemia in a neonate. Clin Infect Dis 1997;24:511.
20)Totemchokchyakarn K, Janwityanujit S, Sathap- atayavongs B, Puavilai S:
Erysipelothrix rhusiop- athiae
septicemia in systemic lupus erythemato- sus. Int J Dermatol 1996;35:818―20.21)Asnis DS, Bresciani AR:Bacteremia due to
Er- ysipelothrix rhusiopathiae
. South Med J 1992;85:332―3.
22)Callon RA, Brady PG:Toothpick perforation of the sigmoid colon : an unusual case associated with
Erysipelothrix rhusiopathiae
septicemia. Gas- trointest Endosc 1990;36:141―3.23)Ruiz ME, Richards JS, Kerr GS, Kan VL:
Ery- sipelothrix rhusiopathiae
septic arthritis. Arthritis Rheum 2003;48:1156―7.24)Hollick GE, Edinger R:
Erysipelothrix
bactere- mia Clin Microbiol Newsletter 1995;17:15―6.25)Schuster MG, Brennan PJ, Edelstein P:Persis- tent bacteremia with
Erysipelothrix rhusiopathiae
in a hospitalized patient. Clin Infect Dis 1993;17:783―4.
26)Fernandez-Crespo P, Serra A, Bonet J, Gimenez M:Acute oliguric renal failure in a patient with an
Erysipelothrix rhusiopathiae
bacteremia and endocarditis. Nephron 1996;74:231.27)Nandish S, Khardori N:Valvular and myocar- dial abscesses due to
Erysipelothrix rhusiopa- thiae
. Clin Infect Dis 1990;29:1351―2.28)Ko S, Kim D, Kwon H, Roh J:A case of multi- ple brain infarctions associated with
Erysipe- lothrix rhusiopathiae
endcarditis. Arch. Neurol 2003;60:434―6.29)Reboli AC, Farrar WE:
Erysipelothrix rhusiopa-
thiae
: An occupational pathogen. Clin Microbiol Rev 1989;2:354―9.One Case with Erysipelothrix rhusiopathiae Endocarditis
Satoshi KODERA
1), Akira NAKAMURA
1), Kenji OOE
2), Keiichi FURUKAWA
3), Naohiro SHIBATA
4)& Yoshitika ARAKAWA
4)Department of Inernal Medicine1)and Department of Clinical Laboratory2), Asahi General Hospital,3)Department of Infectious Diseases, St, Luke s International Hospital,4)Department of Bacterial Pathogenesis and Infection Control,
National Institute of Infectious Disease